
Case Report | DOI: https://doi.org/10.31579/2690-4861/435
Department of Medical-Surgical Specialty, Radiology and Health Care, Cardiovascular Disease Section, School of Medicine, Spedali Civili Hospital, Brescia, Italy
*Corresponding Author: Luca Rodella, Department of Medical-Surgical Specialty, Radiology and Health Care, Cardiovascular Disease Section, School of Medicine, Spedali Civili Hospital, Brescia, Italy via Naviglio Grande 74, 25123 – Brescia (BS), Italy.
Citation: Luca Rodella, Alessio Nicolai, Mattia di Pasquale, Matteo Pagnesi, Elio Gorga, et al, (2025), Coronary Vasospasm and Heart Rhythm Disorders: A Case Report, International Journal of Clinical Case Reports and Reviews, 8(2); DOI:10.31579/2690-4861/435
Copyright: © 2025, Luca Rodella. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 January 2025 | Accepted: 15 January 2025 | Published: 30 January 2025
Keywords: vasospasm; vasospastic angina; coronary angiography; electrocardiogram, atrioventricular block; inflammation
Vasospastic angina (VSA), also known as variant angina, is a condition characterized by recurrent episodes of chest pain, frequently during the night or in the early hours in the morning, due to spasm and contraction of the muscular tonaca of the coronary arteries, differentiating therefore from classic angina. The real physiopatological mechanisms of VSA are still a field of considerable research, although it is now clear that inflammation plays an important role in the genesis of the spasm. Pharmacological therapy, based today primarily on the use of nitrates and calcium channel blockers, is also an area of study to guarantee a bassetter prognosis for these patients.
We present the case of a 56-year-old patient, affected by arterial hypertension and with no cardiac history, who called the Emergency number because of an episode of resting angina at home. When emergency vehicles arrive the patient was initially asymptomatic and electrocardiogram was normal. For recurrence of chest pain, a second ECG tracing was performed and it highlighted a second degree atrio-ventricular block, Mobitz 2, ST-segment elevation in the infero-lateral and sub-ST segment in leads V1-V2 (Figure. 1). The patient was then taken to the Hemodynamics of our Hospital for urgent coronary angiography. The exam did not find significant coronary atherosclerosis affecting the epicardial coronary arteries (only a 30-40% stenosis of the right coronary artery in the middle section was described). At the transthoracic echocardiogram performed in the Coronary Unit, significant valvular defects were excluded, the left ventricular ejection fraction (LVEF) was preserved with only a mild hypokinesia of the inferior-posterior wall. In the suspicion of vasospastic angina on the documented atherosclerotic plaque of the right coronary artery, Diltiazem i.v. was introduced into therapy and then orally. In the following 48 hours the patient experienced two different episodes of angina with an ECG tracing compatible with inferior-STEMI and third degree atrioventricular block (Figure. 2). The symptoms rapidly reduced after intravenous nitroglycerin administration, with prompt restoration of sinus rhythm (Figure. 3). Enzyme curve was not significant (hs-TnT 10 ng/L, Ck-Mb 3.4 mcg/L). During the hospitalization the therapy with calcium channel blocker was up-titrated and nitrate was also introduced, without further anginal episodes or major brady-arrhythmias. Considering the mild coronarosclerosis and the high lipoprotein-A levels (Lp(a) 85 mg/dl), we decided to maintain the therapy with acetylsalicylic acid and the Rosuvastatin/Ezetimibe combination. After 5 days the patient was transferred, asymptomatic and with good haemodinamic status, to a cardiac rehabilitation facility. At the follow-up visit in the Day Hospital Ambulatory, 3 months later, the echocardiogram was normal, and the drug therapy was well tolerated. No new arrhythmic events were detected at the control Holter ECG.
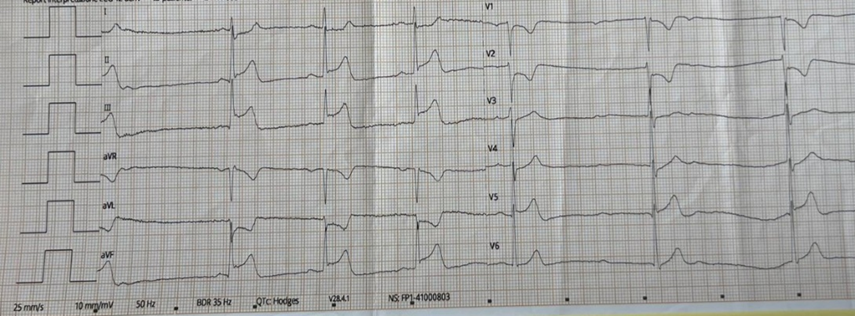
Figure. 1: ECG performed by the Emergency Service at first contact with the patient experiencing chest pain
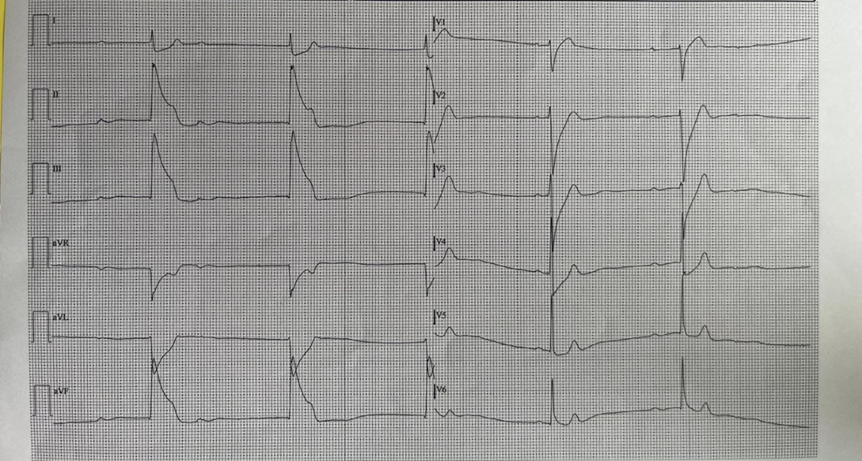
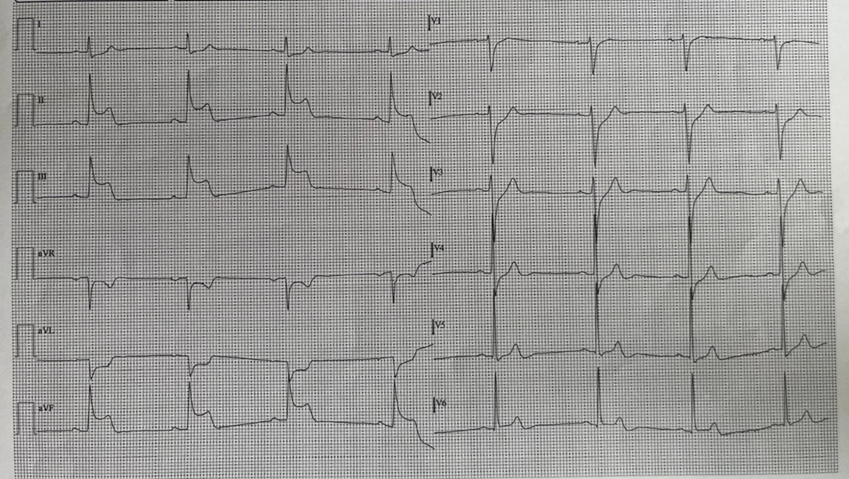
Figure. 2: ECG changes during angina attacks
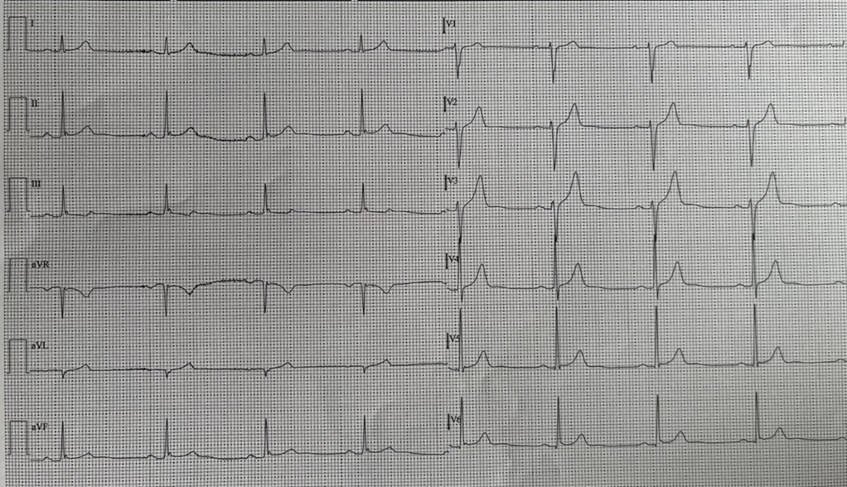
Figure. 3: Normalization of the trace and restoration of sinus rhythm after administration of nitrate i.v. during coronary spasm
Printzmetal et. al introduced the concept of vasospastic angina (VSA), also known as variant angina, for the first time in 1959. It is a condition characterized by episodes of thoracic pain with onset independent of effort, often during the night or in the early hours in the morning, due to spasm and transient contraction of the muscular tunica of the coronary arteries with consequent myocardial ischemia [1,2]. The angina is not necessarily associated with concomitant alterations on the ECG trace. Coronary vasospasm is considered one of the aetiological causes of myocardial infarction without significant coronary obstruction (MINOCA), although today still underdiagnosed because provocative tests are not used as a routine tecnique [3]. The symptoms are certainly heterogeneous: chest pain, tachy- or brady-arrhythmias, syncope and dyspnea can occur [4]. Traditionally, vasospastic angina can be classified in relation to ECGgraphic disturbances of ventricular repolarization (i.e. ST-elevation or depression) or based on the anatomical location of the spasm: epicardial or microvascular, although the two can coexist [5]. ST elevation is usually the main and more frequent alteration, with the underlevelling in the specular leads, negative T waves are also frequent [6] (Table. 1).
| Vasospastic angina | Classic angina | |
Clinical manifestations |
|
|
| ECG changes |
|
|
| Physiopatology |
|
|
Drug treatments |
|
|
Epidemiology:
Calculating the exact prevalence of VSA is not so simple because provocative tests are not frequently used in clinical practice. A recent meta-analysis which involved 6500 patients without obstructive CAD calculated a prevalence of epicardial vasospasm of 40% and 24% for microvascular spasm [3]. In patients with angina attacks and with no coronary artery disease a further trial reported that vasospasm was present in 62% of cases (45% epicardial, 55% microvascular respectively) [7]. According to data from Hung et. al VSA is more frequent among the Asian population, primarily Japanese, and in a smaller percentage among the Caucasian ethnic group [8].
Pathophysiological mechanisms:
The precise mechanism responsible for coronary vasospasm is still not completely clear. Among the factors that can favor the development of this condition there are certainly inflammation, oxidative stress, endothelial dysfunction, genetic and lifestyle factors. Numerous evidences show that inflammation of the perivascular and myocardial tissue may be involved in the genesis of spasm [9]. To confirm this hypothesis, it is estimated that coronary vasospasm is responsible for angina symptoms in approximately 70% of patients with viral myocarditis [10]. Klonaris et al. described a case of myocarditis in a patient with VSA in 1978. In patients with VSA the inflammation of the adventitia of the coronary arteries was also confirmed by the increased uptake of fluorodeoxyglucose (18 F-FDG) at PET [11]. In 1991 Kounis and Zavras discovered that the inflammatory response secondary to an anaphylactic reaction can be responsible for coronary artery spasm with increased risk of sudden cardiac death. The hyper-reactivity of the smooth muscle cells of the vessels (VSCM) certainly plays a central role. This condition is favored by the production of vasoconstrictor molecules such as endothelin-1 and oxygen free radicals (ROS), and also by the deficiency of vasodilatory factors such as nitric oxide (NO) or prostaglandins with consequent endothelial dysfunction and alteration of vasomotor tone: this condition prevents the adaptation of coronary flow in relation to oxygen demand with consequent vasoconstriction [9].
If the association between the inflammatory substrate and atherosclerotic coronary artery disease is now well established, it is now increasingly evident that the levels of pro-inflammatory mediators (CRP, IL-1, IL-6...) are also increased in patients with VSA. Tanaka et. al propose Tocilizumab, an anti-IL-6, as a potential therapeutic agent in these patients. The greater M1-differentiation of macrophages, responsable of endothelial dysfunction, was also confirmed in these subjects [12]. Other inflammatory metabolites involved in the pathophysiology of VSA are IFN-alpha, PD-L1, macrophage inflammatory protein (MIP)-1alpha and MIP-1beta. A recent Japanese trial, performed on 5720 patients with VSA (average age 67 years), and without atherosclerotic disease, showed that the RNF213 gene, especially in its missense variant, is frequently associated with vasospastic angina. This gene codes for NO synthase and its mutation determines a reduced activity of the enzyme with consequent lower production of NO [13]. Another trial examined the function of RNF213 by showing how its activity increases in response to blood vessel shear stress [14].
Numerous data have confirmed that the signaling promoting the hyper-reactivity of vascular smooth muscle cells is responsible for an amplification of the inflammatory response, determining a process that worsens coronary spasm. Finally, T lymphocytes are involved in this process and are hyper-activated [9].
Drug therapy
VSA therapy is based on the use of nitrates, currently first-line drugs, to reduce the frequency of angina attacks although they ca not favorably modify the long-term prognosis [9]. Bugiardini et. al report that the use of nitrates can, however, be associated with a reduction in coronary flow reserve with a consequent increase in the discrepancy between myocardial oxygen demand and supply [15]. The other major pharmacological class commonly used in patients with VSA is represented by calcium channel blockers, capable of reucing myocardial contractility and O2 consumption by decreasing calcium intake into the myocardiocyte during depolarization, and increasing blood flow. The positive effects of this class of drugs in alleviating the symptoms of vasospasm have been known since 1980 [16], subsequent studies have shown how they are also able to control arrhythmic events [9]. Beta-blockers, particularly non-selective ones, have been found to be contraindicated in the treatment of VSA since by potentially also acting on alpha-adrenergic receptors they could reduce the dilation capacity of the artery with consequent possible intensification of vasospasm. Antiplatelet agents are commonly used in patients with VSA and concomitant atherosclerosis (approximately 60% of cases) [17]. Statins still have a controversial role: in the study by Ishii et al. their use was associated with a lower incidence of cardiovascular events and an improvement in prognosis although in two subsequent trials, conducted by S.R. Kim, high-dose statins improved the lipid profile without impacting outcomes in terms of symptom reduction [18].
Cases in literature
Costa et. al [19] describe the case of a 70-year-old patient, hypertensive and with no cardiological history, who entered the emergency department for recurrent chest pain and syncope. Episodes of angina were frequent, especially during the night. In the previous days the woman perform a 24-hour Holter ECG monitoring which she was wearing at the moment of Emergency department admission. Although the echocardiogram and ECG were normal, the Holter ECG showed ST-segment elevation during the night and also in the occasion of syncope, followed by second degree atrioventricular block type 1 and 2. Non significant coronary atherosclerosis was documented at the angiography. Authors decided to introduce pharmacological therapy with Isosorbide dinitrate 40 mg, Amlodipine 5 mg and atorvastatin 40 mg with clinical benefit and without further similar episodes.
Ferreira et. al [20] instead present the case of a young pre-menopausal woman, dyslipidemic and smoker, who underwent a cardiological evaluation for repeated episodes of chest pain, independent of physical exertion, and syncope. Among the documentation viewed by the patient, an ECG-Holter highlighted moments of third degree AV block with pauses of up to 4.5 seconds associated to ST-segment elevation. During the evaluation the patient experienced angina and on the ECG tracing she presented ischemic changes in the ventricular repolarization in the inferior leads. After sublingual nitrate administration ECG returned gradually normal. Also in this situation coronary arteries have no significant stenosis; therapy with nitrates, nifedipine and statin was introduced. At the follow-up control the patient still complained of recurrent symptoms, and at the control ECG-Holter significant pauses persisted. The nitrate was replaced with Verapamil and definitive PM implantation was performed. In the our case, device implantation was postponed considering the complete resolution of the symptoms after the medical therapy optimization and because no further brady-arrhythmias were documented.
Significant progress has been made to understand the exact pathophysiological mechanism underlying VSA- The fundamental role played by inflammation is now clear but it is surely a field that will need to be explored in ever greater depth in the years to come. In the future it will also be necessary to resolve the current uncertainties regarding the optimal therapeutic management of these patients, in particular to guarantee them a better long-term prognosis and not just a lower recurrence of symptoms. Another notable question regards the predisposing factors of coronary vasospasm developement. Current research is concerned with providing answers to our countless questions as soon as possible.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
