
Case Report | DOI: https://doi.org/10.31579/2641-0419/116
1Department of Cardiovascular Medicine, Kizilisu Krighiz, The People’s Hospital of Kizilisu Kirghiz Autonomous Prefecture, Xinjiang, China.
2Department of Cardiology, the First Affiliated Hospital of Nanjing Medical University.
*Corresponding Author: Yanrong Liu and Dianfu Li, Department of Cardiology, the First Affiliated Hospital of Nanjing Medical University.
Citation: Tianbao Xu, Esmayilaji Patiway, Gulistan Alim, Chenghui Tong, Jinghe Zhao, Patigul Rozi, Eslamgul Hayrilla, Zemu Wang, Dianfu Li, Yanrong Liu (2020) Coronary Artery Embolism and Antiphospholipid Syndrome: A Case Report and Review of the Literature. J. Clinical Cardiology and Cardiovascular Interventions, 3(13); Doi:10.31579/2641-0419/116
Copyright: © 2020 Yanrong Liu and Dianfu Li, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 November 2020 | Accepted: 01 December 2020 | Published: 09 December 2020
Keywords: coronary embolism; antiphospholipid syndrome; anticoagulation; hydroxychloroquine (HCQ); statins.
Coronary artery embolism is an uncommon cause of acute myocardial infarction (AMI), while antiphospholipid syndrome (APS) is one of the rare reasons due to premature AMI. Coronary angiography can diagnose coronary artery embolism, and the positive serum of aPLs may infirm APS. We report a 32 years old man with ST-elevation AMI, without any high-risk factors of coronary artery disease. Coronary thrombosis was founded in the M1 sub-coronary of Left Anterior Descending (LAD), and the coronary artery was recanalized, the artery was not obstructive, Thrombolysis in Myocardial Infarction (TIMI) grade was III. He became shortness after exercise, the echocardiography showed his left ventricular was enlarged and LVEF was decreased. High titers of an anticardiolipin antibody (aCL) IgG of 46U (positive >20.0U), and it was positive at two dosages with an interval greater than 12 weeks. But there was no evidence of any other serum markers suggesting other associated pathologies such as SLE, so the primary APS was diagnosed. We gave him anticoagulation with warfarin and a single antiplatelet with Aspirin, the target INR was 2.5-3.0. Meanwhile, statins and hydroxychloroquine (HCQ) were all prescribed. After 6-months follow-up, his heart failure symptoms were disappeared, the LVDd and LVEF were all normal, the titer was decreased to nearly normal. In clinical background, young AMI without traditional high-risk factors of CAD, we should suspect APS. Therefore, we believed that HCQ may low thrombotic rate, down-trending aPLs titer, and prevent thrombotic recurrences in patients with primary antiphospholipid syndrome.
Coronary artery embolism is an uncommon cause of acute myocardial infarction (AMI), being identified as an etiology in 3-4% of the diagnosed cases, and it is easy to be ignored in clinical practice [1]. AMI is rarely associated with antiphospholipid syndrome (APS), therefore, the development of thrombosis in the coronary arteries is highlighted, and it is estimated that approximately 2.8-5.5% of cases of AMI in young individuals are secondary to APS [2].
The APS is defined by a state of hypercoagulability secondary to a wide spectrum of presentations. Its presentation is quite variable, constituting a spectrum of findings ranging from the presence of cutaneous alterations to the involvement of multiple organs, leading to systemic collapse. It is associated with thrombotic events involving venous and arterial territories, large arteries and veins as well as microvascular circulation and obstetrical events, in association with persistent antiphospholipid antibodies (aPLs), one or more of lupus anticoagulant (LA), and anticardiolipin antibodies (aCL) and /or IgM anti-beta 2 glycoprotein 1(ß2GP1) [3], which are implicated in the development of endothelial dysfunction among the factors. This syndrome is classified as primary when there is no association with other pathologies or secondary when it is linked to an underlying disease [4].
In APS, the mechanism of myocardial ischemia differs from that which occurs classically in coronary artery disease, a fact that implies the need for a specific therapeutic approach for patients with this syndrome [5].
Herein, we describe the case of a patient with APS who had AMI with ST-segment elevation on electrocardiogram and subsequent coronary stent thrombosis and then the thrombosis was autolysis. But the myocardial cells were damaged, left ventricular was enlarged and the LVEF was decreased.
Case Presentation
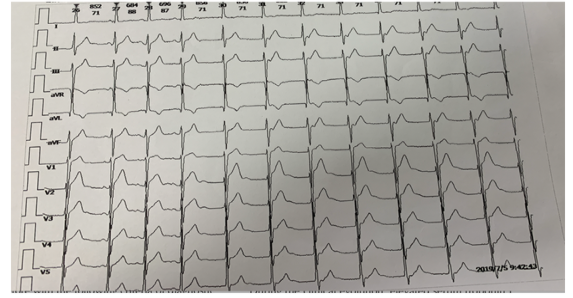
A young Chinese man, 32 years old, was admitted with chest pain for six hours in 6 months before, according to the ECG of V1-V4 ST elevation (Figure 1) and increased troponin T, the diagnosis of AMI was confirmed.
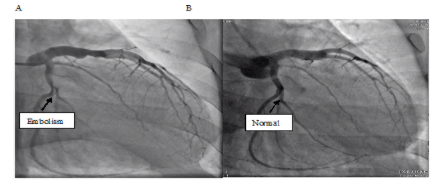
The laboratory findings were as follows: hemoglobin, platelets count, prothrombin time, liver and renal functions were all normal. But the troponin T and NT-proBNP were elevated. He received dual antiplatelet aggregation therapy (aspirin and Ticagrelor) and performed with coronary angiography after 6 hours of the symptom onset. Coronary thrombosis was founded in the M1 sub-coronary of LAD, and the coronary artery was recanalized, the artery was not obstructive, TIMI grade was III (Figure 2).
On the 20 days after discharge, the patient was readmitted with fatigue and a little shortness while he was climbing upstairs. During the laboratory evaluation, there was no significant change in the results, except for high titers of an anticardiolipin antibody IgG of 46U (positive >20.0U) and IgM of 14.6U (negative < 20.0U) and anti-β2-Glycoprotein I with IgG of 10.6RU/ml (negative < 20.0RU/ML). This test result was positive at two dosages with an interval greater than 12 weeks, there was no evidence of any other serum markers suggesting other associated pathologies such as SLE.
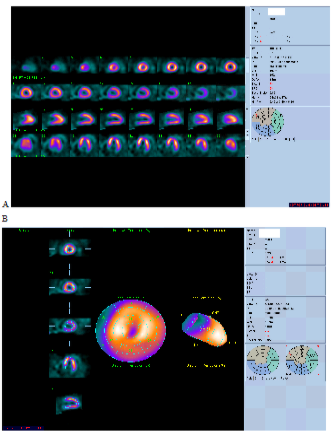
The myocardial scintigraphy with Thallium-201 at rest was performed to evaluate myocardial viability on 1-month of re-hospitalization, demonstrating viability associated with LAD artery territory [6]. It was an abnormal motion of the left ventricular and the left ventricular was enlarged (Figure 3).
Transthoracic echocardiography was also demonstrated that the left ventricular was enlarged (LVDd 59mm) the ejection fraction was decreased as 43.8%, and akinesis of segments: basal anterior septal, mid-anterior septal [7].
As such, primary APS was diagnosed according to the Sydney consensus statement on classification of APS [8] and oral anticoagulation (Warfarin) plus low-dose aspirin(LDA). Hydroxychloroquine (HCQ, 400mg/day, 200mg twice a day) and statin (fluvastatin 80mg/day) with early outpatient follow-up were indicated [9]. According to the patient has symptoms and signs of heart failure, ACEI, beta-blocker, and spirolactone were added to anti-heart failure, and we added ACEI and beta-blocker and tittered to target dosage gradually.
This patient is a young man without any other high-risk factors of coronary artery disease. The diagnosis of APS was established by the presence of antipholipid antibodies and coronary thrombosis formation and the cTnT was higher and the evolution of ECG characteristics.
We followed him six months, the anticardiolipin antibody IgG of 27.8U and IgM of 15.6U, anti-β2-Glycoprotein I with IgG of 10.7 RU/ml (negative < 20.0RU/ML), NT-proBNP <5.0pg/mL, D-dimer 0.18mg/L. The echocardiography showed that LVDd 49mm, LAD 36mm, EF was normal. And six minutes’ walk was 602 miles, and we prescribed him for Mon-antiplatelet therapy of Aspirin and antithrombotic agents of warfarin adjusted the INR between 2.5-3.0.
Literature Review and Discussion
The pathology of acute coronary syndrome involves coronary thrombosis and platelet accumulation(10). Acute Coronary Syndrome (ACS) is categorized into unstable pectoris, ST-segment elevation, and non-ST-segment elevation. Coronary embolism is uncommon and is difficult to distinguish from other causes of AMI solely based on symptoms. The common risk factors of ST-segment myocardial infarction were hypertension, diabetes mellitus, dyslipidemia, glucocorticoid use, and smoking [11]. If a young male suddenly appears as AMI, without any atherosclerotic risk factors, but with a history of one of the following: atrial fibrillation, endocarditis, valve replacement, or venous thrombosis should be suspected as coronary embolism, while APS was an uncommon cause of coronary embolism. In this case, the patient did not have such risk factors as mentioned above, so we believed that the hypercoagulable state resulting from APS contributes to the progression and development of ST-elevation myocardial infarction.
Since the first description of APS in 1983, a long way has already been overcome [12]. However, new exciting knowledge is coming up in this field since the wider awareness of this disease has increased in interest. The heart is an important target organ in APS. Cardiac manifestations of APS include heart valve disease, stenotic or occlusive thrombotic coronary artery disease, intracardiac thrombus, left ventricular hypertrophy and dysfunction, and pulmonary hypertension. Myocardial small vessel involvement can be highly prevalent in APS patients [13].
APS may be a cause of coronary embolism as these above situations are absent [14]. Typically, APS has 3 major presentations: arterial and venous thrombosis, pregnancy loss and thrombocytopenia. Clinically, APS patients are divided into 4 types: I, positive for at least one laboratory indicator; type IIa, only positive for LA; type IIb, only positive for aCL; type IIc, only positive for ß2GP1 [15].
The frequency of myocardial infarction in patients with APS is reportedly 4% and the presence of antiphospholipid antibodies has been associated with myocardial infarction in young patients [16] There is an increased risk of myocardial infarction in patients with APS caused by coronary thrombosis rather than by premature atherosclerosis.
Anticoagulation should be achieved with warfarin or a novel anticoagulant rather than antiplatelet drugs [17]. Patients who received a coronary stent at the time of coronary angiography are more complex. Management may either be with triple therapy or a single antiplatelet agent coupled with oral anticoagulation, such as warfarin and Aspirin. Again, in the absence of guidelines, decisions are at the discretion of the individual clinician and assessment of bleeding risk against the risk of further thromboembolic events [18]. If the underlying vessel appears free of atherosclerosis according to coronary angiogram and without implanting the stent, the patient may be managed with anticoagulation alone.
Standard-of-care secondary thromboprophylaxis with dose-adjusted VKAs such as warfarin has several drawbacks, including adverse interactions with food and other drugs, the need for careful monitoring to keep patients with a desired range of the international normalized ratio (INR) and increased risk of bleeding [19]. The Non-Vitamin K Antagonists Oral Anticoagulants (NOACs,) are designed to provide predictable anticoagulation that can be delivered at a consistent dose and that does not require continuous monitoring [20]. But there are possible disadvantages to their use because of their pharmacokinetic profiles. Unlike warfarin, direct oral anticoagulants (DOACs) have only 1 molecular target so could be less effective in potent thrombophilic states. Anticoagulant doses needed to prevent arterial thrombosis are higher, so DOACs may not be adequate. Lastly, DOACs short half-lives may theoretically lead to additional “breakthrough” thrombosis and anticoagulation failures. Evidence is needed before we can widely adopt the use of DOACs in these high-risk populations [21]. DOACs role in the therapy of APS is under investigation but not verified [22]. It seems clear that the identification of subgroups of patients with distinct clinical features will allow a more precise therapeutic strategy and better patients care. However, the best clustering strategy is still a matter of debate. Probably, several other underappreciated factors might influence the risk of moving the balance to or away from the thrombotic state [23].
The actual mechanism of thrombosis in APS is as yet unknown, but numerous mechanisms have been proposed. Mammalian target of rapamycin (mTOR) is associated with APS-related vasculopathy. Of note, a growing pool of evidence suggests that mTOR inhibitors might induce a prothrombogenic phenotype in patients, leading to thrombosis and limiting their use in patients with aPL [24]. mTOR inhibitors such as sirolimus may be especially useful in APS patients with AMI requiring percutaneous intervention (PCI) to decrease in-stent vascular proliferation occurring several months after stent implantation [25].
The relapse rate in APS remains high, around 20%-21% at 5 years in thrombotic APS. Several pharmacological mechanisms explain the therapeutic potential of Hydroxychloroquine in rheumatic and related diseases. Hydroxychloroquine (HCQ) has various immunomodulatory, metabolic, cardiovascular, antithrombotic, and antineoplastic effects [26]. And HCQ has shown its efficacy in primary and secondary thromboprophylaxis, both in aPL positive and aPL negative SLE patients. HCQ could exert its anti-thrombotic ability through more than one mechanism and it shows an excellent safety profile [27]. HCQ can low thrombotic rate, down-trending aPL titer, and prevent thrombotic recurrences in patients with systemic lupus erythematosus and recently also in patients with primary antiphospholipid syndrome [28]. Despite the promising result, further evidences are needed in order to confirm the effective role of HCQ in preventing thrombotic recurrences in APS setting.
The patient’s decreased titer of aPL maybe relate to the HCQ, according to the previous studies, although other studies did not confirm this association. The titers of aPL frequently decrease and eventually become negative during the follow-up period [29]. The negativization has been related to a lower risk of thrombotic event, allowing to discontinuation of anticoagulation after aPL seroconversion seems to be reasonably safe, at least in primary APS [30].
While APS patients’ autoantibodies to phospholipid-binding proteins are thought to be pathogenetic through a variety of mechanisms, including interacting with the coagulation and fibrinolytic systems, monocyte and neutrophil activation, endothelial cell activation, and complement-mediated processes [31]. Statins are widely used for the treatment of hypercholesterolemia and in secondary prevention of atherosclerotic coronary disease. Stains have pleiotropic effects including the inhibition of vascular adhesion molecules, interleukin 6, and tissue factor in endothelial cells. In humans, Fluvastatin has been shown to significantly reduce pro-inflammatory and prothrombotic markers in APS patients [32].
Conclusions
Coronary embolism is uncommon in young adults and generally presents with chest pain and dyspnea. The diagnosis of coronary embolism is made definitively by cardiac catheterization. Echocardiography is needed to explore the origin of the thrombus. The antiphospholipid syndrome may be one of the etiologies. Thus, immunological tests should be performed. Long-term anticoagulant and antiplatelet therapies are recommended. HCQ and statins may reduce the titer of aPL to reduce the recurrence of coronary artery thrombosis. But we need more studies and case-control studies to confirm this conclusion. It is still needed to clarify if the future integration of artificial intelligence and big data to patient care might help in the management of the patients with APS considering hundreds of other risk factors unappreciated until now.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
