
Case Report | DOI: https://doi.org/10.31579/2641-0419/207
1 General Hospital Presidente Perón. Avellaneda. Interventional Cardiology.
*Corresponding Author: Rodrigo A. Martin, General Hospital Presidente Perón. Avellaneda. Interventional Cardiology.
Citation: Rodrigo A. Martin, Ricardo Marcelo Cetera, Amalia Descalzo, Sergio Zolorza (2021) Coronary Angioplasty of the Circumflex Artery with anomalous Left Coronary Artery and origin from the Right Sinus of Valsalva ¨A Case Report¨. J. Clinical Cardiology and Cardiovascular Interventions, 4(14); DOI:10.31579/2641-0419/207
Copyright: © 2021 Rodrigo A. Martin, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 August 2021 | Accepted: 30 August 2021 | Published: 03 September 2021
Keywords: coronary artery; cardiac catheterization; anomalous couse; atherosclerotic disease; coronary angioplasty
We report a patient in the sixth decade of life with a benign anomalous course and a history of atherosclerotic disease in the right coronary artery with the presence of ischemia. We present a clinical case of infrequent finding of abnormal left coronary artery and obstructive atherosclerotic lesion in the circumflex artery. The authors decided to perform coronary angioplasty on the lesion found. Because it is an infrequent condition, we conducted a literature search in which we focused on the statistical findings, the clinical presentation and detailed the treatment of the patient by means of coronary angioplasty. Despite the difficulty of the case, success was achieved.
The coronary arteries originate from the right and left sinuses of Valsalva. There are causes that can alter their normal origin, course or anatomical arrangement and, although such malformations are rare, they carry a significant risk of arrhythmias, angina, infarction and sudden death, a risk that is higher during childhood and adolescence. The origin of the left coronary artery from the right sinus of Valsalva corresponds to a very infrequent coronary anomaly, with an incidence between 0.2 and 1.2%. It does not usually produce clinical repercussions and its diagnosis is usually an occasional finding. However, it can be associated with myocardial ischemia and even sudden death, especially in young patients during exercise. In case of coronary atherosclerotic disease, it does not usually develop over an anomalous coronary pathway. We present the case of a patient in whom obstructive disease of the circumflex artery was found with origin of the left coronary trunk at the level of the right coronary sinus in which coronary angioplasty with stenting was performed.
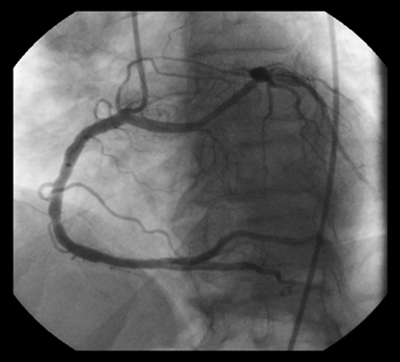
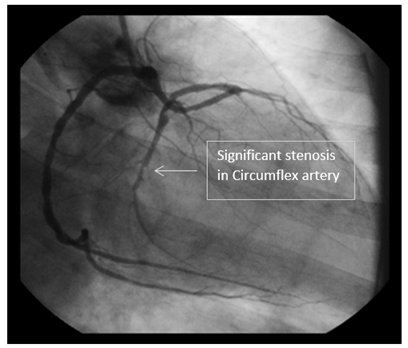
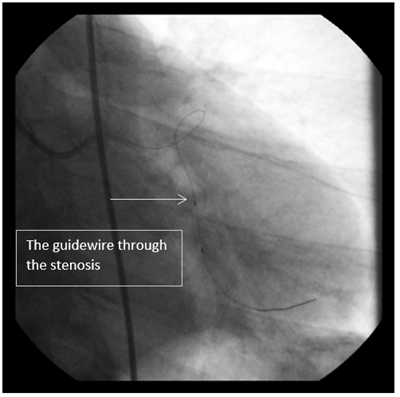
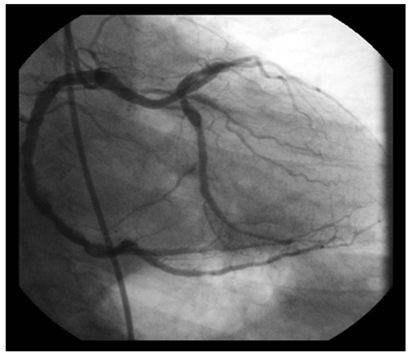
A 66-year-old male patient with positive cardiovascular risk factors for hypertension, smoking and dyslipidemia. He had a history of non-ST-segment elevation acute coronary syndrome two years earlier, during which he underwent coronary angioplasty on the right coronary artery. The patient was asymptomatic until six months prior to his consultation, when he started with angina type II and SPECT was performed, which showed moderate ischemia in circumflex territory. He was referred to the Interventional Cardiology Unit for percutaneous coronary intervention. Coronary angiography was performed by femoral access with Super Sheath introducer (Boston Scientific) 6 FR and diagnostic catheters 6 FR Judkins Left 3.5 and Judkins Right 3 Impulse (Boston Scientific) finding the right coronary artery without significant angiographic lesions and the birth of the left coronary artery trunk was observed from the same right coronary sinus. At this level the presence of a significant obstruction from the middle segment of the circumflex artery can be observed (Figures 1 and 2). In a programmed way (Figures 3 and 4) and by Femoral access with Super Sheath 6 FR introducer and Convey Left 6 Fr Guide Catheter (Boston Scientific) was performed through Choice Floppy guide wire 0.014 x 180 (Boston Scientific), which with difficulty due to severe tortuosity was positioned in the distal segment of the Circumflex artery, dilatation with Emerge 2. 5 x 15 mm Coronary Balloon. (Boston Scientific) and final implantation of a 3.0 x 16 mm Promus Premier type Everolimus Coronary Stent (Boston Scientific).
Coronary artery anomalies identified by coronary angiography are unusual findings [1], among which the origin of the left coronary artery in the right sinus of Valsalva is a very rare pattern with an incidence between 0.2 and 1.2
Not declared
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
