
Case Report | DOI: https://doi.org/10.31579/2690-8808/215
1Specialist in General Medicine, Pakistan Atomic Energy Commission General Hospital, Islamabad, Pakistan.
2General surgeon, Pakistan Atomic Energy Commission General Hospital, Islamabad, Pakistan.
3Diploma, Health Office Administration, Canada.
4Trainee in vascular surgery, Klinikum Nordfriesland Husum Schleswig –Holstein Germany.
5Anesthesiologist, Pakistan Atomic Energy Commission General Hospital, Islamabad, Pakistan.
6Honours Bachelor of Health Sciences, University of Ottawa Canada.
7Diploma of anesthesia, Pakistan Atomic Energy Commission General Hospital, Islamabad, Pakistan.
*Corresponding Author: Anum Ashfaq, Specialist in General Medicine, Pakistan Atomic Energy Commission General Hospital, Islamabad, Pakistan.
Citation: Ashfaq A, Jamil K, Ashfaq R, Semeen H, Khan MA, et al, (2024), Contemporaneous Presentation of Acute Appendicitis and Acute Cholecystitis: A Rare Entity, J, Clinical Case Reports and Studies, 5(7); DOI:10.31579/2690-8808/215
Copyright: ©, 2024, Anum Ashfaq. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 August 2024 | Accepted: 23 August 2024 | Published: 28 August 2024
Keywords: acute appendicitis; acute cholecystitis; laparoscopic surgery
Acute appendicitis and acute cholecystitis, presenting separately, are two most common entities encountered by surgeons on daily basis; but coevality of both diseases is a very rare phenomenon. Here we present a case of 32 years female who presented with right hypochondrial, flank pain and right iliac fossa pain accompanied by nausea, vomiting and fever. Examination revealed positive Murphy’s and McBurney’s sign. Investigations revealed acute appendicitis along with acute cholecystitis. Appendectomy and cholecystectomy was done by single laparoscopic surgery. Surgery went uneventful and patient had good recovery.
Acute appendicitis and acute cholecystitis are two of the various causes of acute abdominal pain presenting in surgical emergency department worldwide. These diseases usually present with fever, nausea and abdominal pain. Presenting separately, these two diseases are most common causes of emergency abdominal surgeries but it is very rare for these two presenting simultaneously in a single patient as symptoms are often vague and ambiguous.
Here, we present a rare case of a patient presenting with ambiguous right sided abdominal pain and diagnosed and treated on lines of acute appendicitis along with acute cholecystitis.
A 32-year-old female with no premorbids presented in emergency department with vague right sided abdominal pain for 1 day. She also complains of associated fever, anorexia and nausea. Fever was associated with chills and it was continuous which relieved only with antipyretics. Her past history was positive for subacute appendicitis and subacute cholecystitis 3 years back which was treated with oral antibiotics. She also has the history of incidental finding of septated gallbladder found on ultrasonography 3 years back.
On examination, she was vitally stable with blood pressure of 125/79mmHg, pulse 82bpm regular, temperature 100 F, respiratory rate 16/minute and oxygen saturation 96% at room air. Abdominal examination revealed tender right hypochondrium with positive Murphy’s sign, tender right flank area and tender McBurney’s point with rebound tenderness. Other systemic examination was unremarkable. Laboratory studies showed raised total leukocyte count with neutrophilia and raised levels of C-reactive proteins. All other baselines including liver function tests, renal function tests, urine routine examination, blood and urine cultures were normal. Urine pregnancy test was also negative. Ultrasonography of abdomen showed 4mm thick septated gallbladder with gallbladder sludge and small amount of pelvic free fluid although appendix was not visualized. Patient was admitted and given intravenous antibiotics for a day with strict monitoring. After 24-hours, she did not get better with antibiotics and decided to have laparoscopic surgery.
Patient was shifted to operation theatre for laparoscopic appendectomy and cholecystectomy. Anesthesia was given which was smooth and then laparoscopic procedure was started. Four ports were made as follows: 10mm in infraumblical region, 10mm in pigastric region, 5mm in right mid-clavicular and 5mm in right anterior axillary line (figure 1)
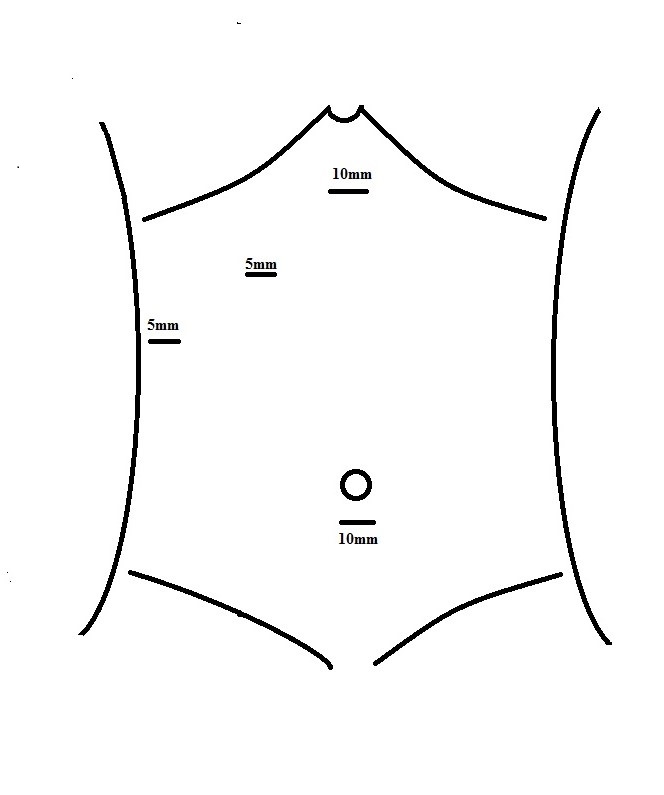
Figure 1: diagrammatic representation of laparoscopic ports
Appendix was retrocecal and acutely inflammed, gallbladder was slightly inflamed and contained gallbladder sludge seen during laparoscopy. Patient was stable after operation and shifted to room. After 8 hours, she started having liquid diet and tolerated well. She was discharged after a day.
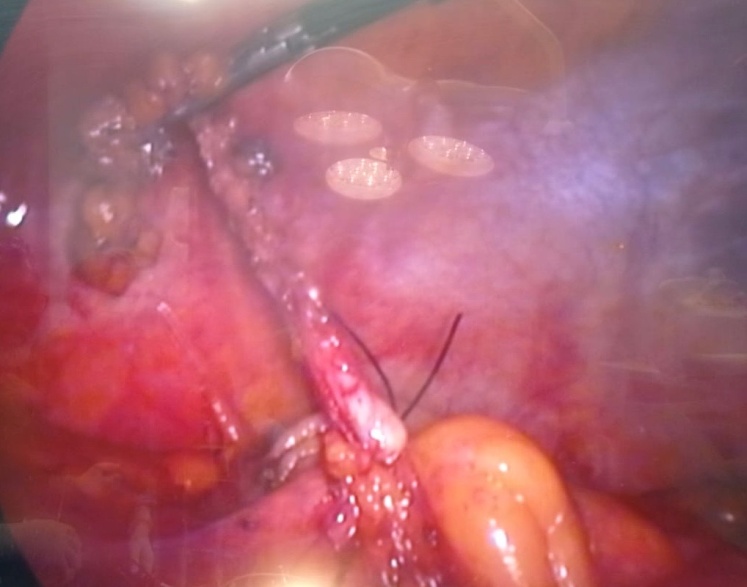
Figure 2: laparoscopic image showing acute appendicitis
Acute appendicitis and acute cholecystitis are most common individual causes for acute abdominal pain [2]. Surgeons perform emergency appendectomies and cholecystectomies on daily basis worldwide but combined surgical procedure is rare [5]. Co-occurrence is a rare entity but known fact bound to acute appendicitis and acute cholecystitis and very few cases are reported in literature till date although exact incidence is not known [2]. Coevality of both diseases is thought to be result of bacterial involvement but exact etiology is not known yet [6]. Patient usually present with right upper and lower quadrant pain along with fever, nausea and vomiting. Kancheva M, et al reported right flank pain in his patient along with right upper and lower quadrant pain similar to our patient, which is also a rare entity [3]. Synchronous presentation is usually diagnosed by foci of pain and eliciting signs on clinical examination [4,5]. It is often difficult to diagnose this dual presentation and to elicit findings on clinical examination like tender McBurney’s point or Murphy’s sign in co-existent disease especially when the pain limits eliciting these signs [2].
To reach diagnosis, CT-scan is performed for acute appendicitis and ultrasonography is a modality for diagnosing acute cholecystitis although CT scan and MRI abdomen are also performed to look for any complications [3]. Abdominal CT-scan has become standard of care in cases of lower abdominal pain for being more accurate than ultrasonography [5].
Combined laparoscopic surgery is a gold standard and safest method for efficient treatment of acute appendicitis and cholecystitis [1,3,7]. Usually 5 ports are used in combined laparoscopic surgery of appendectomy and cholecystectomy [1,2,4,5] but 4 ports can be used for more conservative approach and efficient surgery like in our case. [5]
Contemporaneous presentation of acute appendicitis and acute cholecystitis is a rare entity but it is crucial for surgeons to keep in mind the double diagnosis before operation especially in patients with ambiguous presentation of right sided abdominal pain to avoid any further complications leading to morbidity and mortality.
Proprietary Interest: No conflict of interest with any institution / organization.
No grant or fellowship supporting the writing of the paper.
Institutional approval: Institutional approval was obtained in compliance with regulation of our institution and generally accepted guidelines governing such work.
Author’s contribution: both authors fulfilling the ICMJE criteria.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
