
Research Article | DOI: https://doi.org/10.31579/2692-9562/054
1 Otolaryngologist, Universidade Estadual de Campinas (UNICAMP), Campinas, São Paulo, Brasil. Telephone: +55 41 998158181.
2 Otolaryngologist, Universidade Estadual de Campinas (UNICAMP), Campinas, São Paulo, Brasil.
3 Otolaryngologist, Universidade Federal de Goiás (UFG), Goiania, Goiás, Brasil.
4 Otolaryngologist, Universidade Estadual de Campinas (UNICAMP), Campinas, São Paulo, Brasil.
5 Thoracic surgeon, Universidade Estadual de Campinas (UNICAMP), Campinas, São Paulo, Brasil.
6 Pediatric surgeon, Universidade Federal de Goiás (UFG), Goiânia, Goiás, Brasil.
7 Otolaryngologist, Universidade Federal de Goiás (UFG), Goiânia, Goiás, Brasil.
*Corresponding Author: Leticia Raysa Schiavon Kinasz, Universidade Estadual de Campinas (UNICAMP), Campinas, São Paulo, Brasil. Telephone: +55 41 998158181.
Citation: Leticia Raysa Schiavon Kinasz, Rebecca Maunsell, Melissa Avelino, Debóra Bressan Pazinatto, Luciahelena Prata, Miguel Angelo Corrales Coutinho, Lais Botacin, Tiago Henrique de Souza, Marcelo Barciela Brandão, (2023). Congential tracheal stenosis: from diagnosis to surgical treatment, what the airway surgeon must know. Journal of Clinical Otorhinolaryngology 5(1); DOI: 10.31579/2692-9562/054
Copyright: © 2023 Leticia Raysa Schiavon Kinasz. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 December 2022 | Accepted: 10 January 2023 | Published: 23 January 2023
Keywords: tracheal; stenosis; tracheoplasty; congenital tracheal stenosis; children
Congenital tracheal stenosis (CTS) is a rare pathology characterized by complete tracheal rings and may be associated with cardiovascular and pulmonary malformations. Despite its rarity otolaryngologists that perform airway endoscopy and airway surgery must be aware of this malformation since endoscopic manipulation and tracheostomy in these children are of great risk and may jeopardize definite treatment and trigger emergency fatal situation. Meticulous sizing of the airway and recognition of malformations is crucial for diagnosis, staging and surgical planning. Slide tracheoplasty has been described as the gold standard treatment for long segment CTS with low mortality and complications. We report two cases of long segment CTS in toddlers that were surgically treated with emphasis on precise diagnosis and the possibility of concomitant airway malformations in children.
Congenital tracheal stenosis (CTS)
Neonatal Intensive Care Unit (NICU)
Microlaryngobronchoscopy (MLB)
Pediatric Intensive Care Unit (PICU)
Non-invasive ventilation (NIV)
Próton pump inhibitors (PPI)
Computed tomography (CT)
Congenital stenosis (CTS) is a rare pathology representing 0,3-1% of all laryngotracheal stenosis in children[1]. It is characterized by the presence of complete tracheal rings, that is, a tracheal circumference consisting of 360º cartilage instead of the normal 270o [1-4]. Despite its rarity CTS is still more common than acquired tracheal stenosis that may also be encountered in children due to intubation, infections, surgeries (tracheostomies) or aspiration of caustic substances [1,4-6]. This condition is frequently associated with other cardiovascular anomalies and some authors have described that only 10-25% of the cases tracheal are not associated with other malformations. The most common malformation encountered is left pulmonary artery sling and tracheomalacia [1,4,7,8]. Otolaryngologists must be trained to recognize airway malformations and be aware of the possibility of the presence of concomitant lesions. Due to its rarity CTS may be difficult to recognize and inadvertent manipulation of the trachea in this situation can lead potential airway obstruction and seriously compromise further treatment.
The need for treatment is determined by degree of stenosis and clinical symptoms. Some cases may be managed conservatively and tracheal lumen may be sufficient with childs growth [4,9,10]. Since the 80’s various surgical procedures have been reported but in the past 20 years slide tracheoplasty has been elected as the gold standard treatment [1,2,4,5,7-9,11-15]. A resection with end-to-end anastomosis may be considered for short length stenosis nevertheless, when more than a third of the trachea is involved a slide tracheoplasty is nowadays considered the safest procedure.
The authors report two cases with initial diagnosis of more common airway malformations but associated CTS successfully treated with slide tracheoplasty with emphasis to the challenging diagnosis, surgical planning and pos operative care of such cases.
A 17-month-old girl with a history of prolonged stay in the Neonatal Intensive Care Unit (NICU) at birth due to respiratory distress and persistent biphasic stridor since birth was referred to the airway clinic. The child had never been intubated but described recurrent “laryngitis” requiring numerous admissions to emergency services. At initial evaluation a nasofibroscopy reavealed an apparently narrow subglottis (Figure 1a). A congential subglottic stenosis was suspected and a microlaryngobronchoscopy (MLB) was scheduled. Before the MLB 7 months later the child was admitted with fever, coughing, respiratory distress and was intubated in the Pediatric Intensive Care Unit (PICU) with a 4.0 cuffless tracheal tube. After 12 days of intubation a MLB was performed and revealed signs of acute laryngotracheitis with edema and hyperemia and mucosal laceration. Sizing of the airway revealed a grade II subglottic stenosis (Figure 1b) but also an unexpected finding of complete tracheal rings extending through the entire trachea in a “funnel-type” fashion with only two normal rings distally (Figure 1c and d). A computerized tomography was performed and no associated vascular or pulmonary malformations were encountered. After persistent endoscopic and systemic treatment for the secondary laryngeal and tracheal inflammation due to intubation with topical corticoesteroids, systemic corticoesteroids, antibiotics and non-invasive ventilation (NIV) the patient could not be kept more than 12 days without ventilatory support. After team discussion, a slide tracheoplasty was planned despite persistence of mild-moderate airway inflammation.
The slide tracheoplasty was performed in cardiopulmonary bypass as technique revised by Rutter and Manning [16]. The trachea was assessed through a cervicotomy associated with a sternotomy and the airway was exposed from the cricoid to the Carina. After the child was put in bypass a 0degree 4mm and 2.2mm telescopes were used to mark the middle and distal limit of the tracheal stenosis. The trachea was then transected at the midpoint of the stenosis in an oblique fashion, the cranial segment of the airway was split open at the midline of the anterior wall all the way through the anterior cricoid ring to include the subglottic stenosis in the slide, and the distal airway was open posteriorly up to the distal end of the stenosis two rings above the Carina (Figure 1e). The distal segment of the trachea was then slided into the cranial segment and 5.0 PDS running sutures were used for the anastomosis as previously described (Figure1f). At the end of the procedure endoscopic control of the suture as performed and the child was intubated with an age appropriate cuff less tracheal tube. The patient was extubated four days after the procedure and kept on NIV for 10 days. Two control endoscopies were performed on post operative days 7 and 14. On both occasions airway was cleared of secretions, sutures were revised and proven to be adequate, airway was gently calibrated with age appropriate tubes smeared with corticoid ointment and the child was not reintubated. Two weeks after the procedure there was considerable improvement of mobilization of tracheal secretions and intermittent respiratory noise. Antibiotics and a feeding tube were used for 10 days and the child was discharged from the hospital with very mild stridor and no respiratory distress 20 days after surgery. Follow-up 8 months after surgery can be appreciated on Figure 1 g and h, the airway shows no sign of restenosis neither at the subglottic level or trachea, the child is completely asymptomatic with no dysphonia.
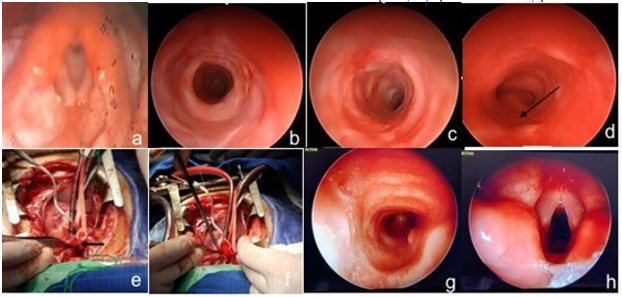
Figure 1 - Case 1: a - nasofibroscopy with the view of a reduced subglottic lumen; b – subglottic stenosis under 4mm telescopic view; c – endoscopic view of the trachea with complete tracheal rings at proximal limit of the CTS with a 4mm telescope; d - endoscopic view of the trachea at the inferior limit the CTS with view of the membranous portion of the adjacent distally normal tracheal rings (black arrow) above Carina; e – Intraoperative view showing the posterior midline incision of the distal trachea (arrow); f – intraoperative view suturing the slided trachea; g- post operative view of the trachea with 4mm telescope at 8 months; h- post operative view of the larynx with 4mm telescope at 8 months.
A female newborn full term was delivered with no complications and developed respiratory distress with retractions and stridor in the delivery room and was put on a 30% oxygen hood. Two days later after no improvement, a nasofibroscopy was performed revealing short ariepiglottic folds and an ômega shaped epiglottis with supraglottic collapse consistent with laryngomalacia. The child was started on próton pump inhibitors (PPI) with no success and continued to present difficulty feeding so at 21 days a MLB was performed. A suprglotoplasty was performed to treat the laryngomalacia but examination of the trachea revealed a long segment CTS with complete tracheal rings in a funnel-shape that did not allow progression of a 4mm telescope nor a 2.5mm tube through its narrowest portion at the midtrachea. A computed tomography (CT) was performed and no other malformations were detected, a new MLB with a 2.7mm telescope was performed confirming a long segment funnel-shaped CTS with two normal distal rings above Carina.
When the child was 4 months old a slide tracheoplasty was performed in cardiopulmonary bypass. The child was extubated three days later after an endoscopic evaluation. Twenty-six days after the surgery a new MLB was performed because the child had persistent mild to moderate retractions and stridor. A slight narrowing was noted at the superior limit of the anastomosis and balloon dilation was performed twice with a three-week interval in an attempt to improve lumen at this point. Two months after the slide tracheoplasty the child still showed signs of mild respiratory distress and a laryngotracheal reconstruction with an anterior cartilage costal graft was performed to address the residual stenosis at the cranial segment of the slide tracheoplasty. The patient was extubated after 3 days with improved respiratory symptoms.
Eighteen months after slide tracheoplasty cartilage graft the child has occasional mild exertional stridor but endoscopic examination reveals no residual stenosis.

Figure 2 – Case 2: A - endoscopic view of complete tracheal rings seen from level of vocal cords; B – intraoperative view of slide tracheoplasty; C – endoscopic view of immediate postoperative aspect of inferior limit of suture with two normal distal tracheal rings; D – immediate endoscopic postoperative view of tracheal suture line; E – endoscopic view of restenosis at superior limit of suture line 26 days after surgery; F – endoscopic view of anterior tracheal costal cartilage graft.
Tracheal stenosis is a rare entity and is of high risk if not diagnosed. CTS is classified into four main types following Grillo [10]. generalized tracheal hypoplasia (type I), funnel-shape tracheal narrowing (type II), segmental tracheal stenosis (type III) and bridge-bronchus stenosis (type IV). Patients may be asymptomatic or mildly symptomatic symptoms may be present and significant in the first days/weeks of life, and as in the case 2, or later as in case 1 [2,10,18]. The most characteristic manifestations include: biphasic stridor sometimes described as “washing-machine noise”, coughing, repeated acute respiratory events, cyanotic spells and respiratory distress [2,4,18,19]. Diagnosis as always in cases of persistent or recurrent stridor is confirmed with airway endoscopy. When complete tracheal rings are identified on endoscopy, imaging is important to exclude associated cardiac, vascular and lung malformations that may occur roughly in 50% of cases [2,12,18-20]. In some cases, bronchography may be useful to fully evaluate the segment distal to the narrowing particularly if an endoscope cannot progress. Concomitant airway anomalies such as congenital subglottic stenosis and laryngomalacia as described in the case reports are much more frequent than CTS. The importance of adequately and skillfully evaluating the pediatric airway cannot be stressed enough, this requires training, documentation and repeated exposure to a good number of cases considering the rarity of some of these malformations.
In a minority of cases surgery may not be needed and the patients may be followed with reevaluations to check on the expansion of the tracheal lumen with growth and worsening of symptoms. A recent study by Yamoto et al has proposed follow up with CT reconstruction that might help define which cases are candidates for surgery [21]. These authors suggest that, if the diameter of the narrowest part of the airway is not smaller than 40% and symptoms are not significant there may not be a need for surgical repair. Another criteria for conservative management according to these authors would be a trachea with a lumen not less than 2.7mm at its narrowest point.
The first surgical approach proposed for CTS in 1982 by Idriss et al was a pericardial graft to perform an enlargement tracheoplasty [2,8,9,18,22]. Since then several techniques have been used such as primary resection and anastomosis, tracheoplasty with autologous and homologous grafts, balloon dilation and stenting and laser sectioning [2-6,12,14,20]. In 1989 Tsang et al described the slide tracheoplasty that was then popularized by Grillo et al [2,4,8,12-18,20]. This has been the gold standard surgery for long segment CTS due to its versatility, use of the patients tracheal tissue and low rate of complications, reinterventions and mortality (less than 5%) [1,2,4-8,11,14]. The slide tracheoplasty doubles the trachea’s circumference, quadruples its diameter and reduces its length by half [24]. Complication rates are low but consist of: granulation tissue in the suture sites an “eight-shape” deformity, suture dehiscence and restenosis [2,4,7]. In 2003 Rutter and Manning [25] reported that after two years using this technique as there first choice for CTS it could be considered superior to other techniques they had used previously. Mortality rates have been decreasing as reported my large series from Cincinatti and London from 30% to 5%. Zenner et al reported that when CTS is associated to Syndromes such as Down, VATER/VACTERL and Apert repairing is more challenging [4,26].
When cardiac malformations are associated these should be corrected preferably at the same time as the slide tracheoplasty [19,21] reinforcing the need of an airway team where otolaryngologists and or dedicated airway and cardiovascular surgeons are integrated. Elliot et al, described association of left pulmonar artery sling in 60% of their cases [27]. In 2016, the Cincinnati group described lung malformations in 18 (13,8%) of their 130 patients submitted to slide tracheoplasty amongst these unilateral pulmonary agenesia was the most frequent finding (61%) followed by unilateral lung hypoplasia (39%).
Tracheostomy should be avoided since it increases the risk of complications, compromises surgical repair of the stenosis and increases risk of granulation tissue, obstruction and death [19,26]. This is why the importance of airway endoscopy cannot be underestimated when considering a tracheostomy for children with respiratory symptoms. As described in both cases there may be coexisting airway pathologies and/or malformations (congenital subglottic stenosis in case 1 and laryngomalacia in case 2) therefore it is essential that the airway endoscopist and /or surgery be familiar with all possible anomalies. Airway endoscopies may need to be repeated with smaller endoscopes as was done in case 2. More narrow stenosis may require bronchographies to further “map” the airway and plan the best surgical approach. In case 1 surgical planning to include the cricoid in the slide was essential or the child would have been left with subglottic stenosis after the slide. In case 2 sizing of the airway post operatively was also essential in recognizing the need for further expansion of the airway after the slide tracheoplasty.
Due to its rarity, large case series of CTS are limited to major international pediatric airway reference centers that have reported over 100 cases [4,6,8,11,24]. Large case series have not been reported in Latin America. Terra et al in 2000 published their results in 7 children surgically treated for CTS but only one was a slide tracheoplasty28. The interest in reporting these two cases is particularly an alert to this probably underdiagnosed pathology. Surgeons must bare this diagnosis in mind, take great care when manipulating complete tracheal rings and particularly when considering a tracheostomy. Airway surgeons must be mindful of the appropriate airway size for the child and size the airway even when treating other airway conditions and ideally be exposed and trained to be familiarized with these rare anomalies.
Surgical success of airway malformations is a result of: precise diagnosis, surgical technique and post-operative management and this is why team evaluation and discussion is paramount: from the otolaryngologist to the thoracic and cardiac surgeon, anesthesiologist and intensive care staff [6,9,12,17,21,24].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
