
Case Report | DOI: https://doi.org/10.31579/2690-4861/478
1 Resident, Department of Pathology and Molecular Medicine, McMaster University, Hamilton, Ontario, Canada.
2 Professor, Department of Pathology and Molecular Medicine, Juravinski Cancer Centre and McMaster University, Hamilton, Ontario, Canada.
*Corresponding Author: Nermeen Feltaos, Resident, Department of Pathology and Molecular Medicine, McMaster University, Hamilton, Ontario, Canada.
Citation: Nermeen Feltaos, Monalisa Sur, (2024), Concurrent primary extranodal marginal zone lymphoma and malakoplakia in the vagina: pearls and pitfalls, International Journal of Clinical Case Reports and Reviews, 18(3); DOI:10.31579/2690-4861/478
Copyright: © 2024, Nermeen Feltaos. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 May 2024 | Accepted: 10 June 2024 | Published: 05 July 2024
Keywords: Marginal zone lymphoma; Malakoplakia; Michalis Gutmann bodies; Granulation tissue
Primary lymphomas of the female genital tract are rare, representing approximately 1% of extranodal lymphomas. The most common histological subtype is diffuse large B-cell lymphoma, followed by follicular lymphoma. Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma) in the female genital tract is rare and usually discovered incidentally. While MALT lymphoma is often linked to infections or autoimmune diseases, its cause in the female genital tract is generally unknown. On the other hand, malakoplakia is a chronic inflammatory condition resulting from an impaired histiocytic response to common bacterial infections.
In this report, we present an extremely rare case of concurrent primary MALT lymphoma and malakoplakia in the vagina of a 79-year-old woman who exhibited postmenopausal bleeding and a soft tissue mass. Tissue examination revealed malignant lymphoid cells obscured by abundant inflammatory cells interspersed with numerous blood vessels, mimicking granulation tissue. A significant diagnostic challenge lies initially in missing the concurrent presence of malignant lymphoma and malakoplakia. Therefore, we emphasize the importance of clinicopathological correlation to accurately diagnose these rare conditions.
Primary lymphomas of the female genital tract (PLFGT) are rare, with the ovary being the most frequently affected site, followed by the cervix, uterus, and vagina. When the disease is disseminated at presentation, it usually indicates secondary involvement of the female genital tract (FGT) [1]. MALT lymphoma of the FGT is exceedingly rare, constituting only 3–5% of all primary FGT lymphomas [2]. It predominantly affects older women, with a median age of 66 years [3]. While primary MALT lymphoma of the FGT is often an incidental finding, lymphomas generally can present as mass lesions or with abnormal vaginal bleeding [4]. In contrast, malakoplakia is a reactive process that can appear as yellow plaques or nodules, sometimes mimicking cancer [5]. Its diagnosis depends on identifying characteristic histiocytes called von Hansemann cells, which contain pathognomonic inclusions known as Michalis-Gutmann bodies [6]. In this case, the initial clinical impression suggested an epithelial malignancy. However, the absence of malignant epithelial cells during the histological examination necessitates further clinicopathological correlation to achieve a definitive diagnosis.
A 79-year-old patient presented with postmenopausal bleeding and fatigue. Her medical history included type 2 diabetes mellitus and hypertension. No palpable lymph nodes were found during the examination. Radiological studies revealed a 6.5 cm soft tissue mass in the vagina extending to the cervix. The patient was referred to a gynecologist, and a speculum examination showed a narrow vagina with irregular and fractured mucosa. The lesion was biopsied and sent to the pathology lab.
Histological examination initially suggested a reactive process due to numerous eosinophilic histiocytes, small lymphocytes, plasma cells, and numerous blood vessels resembling granulation tissue (Figure. 1). Closer inspection revealed von Hansemann cells and Michaelis-Gutmann bodies, indicative of malakoplakia (Figure. 2). Immunohistochemistry (Figure. 3) identified diffuse clusters of CD20-positive B cells amidst CD3-positive reactive T cells, partially expressing BCL2 and CD43. CD10, CD5, and BCL6 were negative, but about one-third of the cells expressed cyclin D1.
Given the predominance of B lymphocytes and their diffuse clustering, a lymphoid neoplasm was suspected. The tissue was subjected to polymerase chain reaction (PCR) for B cell clonality testing and fluorescence in situ hybridization (FISH) analysis for t(11;14) to exclude Mantle cell lymphoma. PCR confirmed a monoclonal B cell population with a monoclonal IgH chain in various regions, but FISH testing failed.
Following the pathology report, the patient was treated with azithromycin for malakoplakia, resulting in the cessation of her abnormal uterine bleeding. She was also referred to a hematologist who ordered a positron emission tomography (PET) scan for staging. The scan showed intense fluorodeoxyglucose (FDG) uptake confined to the vagina, establishing stage IE. The patient then underwent radiation therapy.
After the antibiotic treatment, a second biopsy showed a similar morphology with reduced inflammation. FISH analysis was repeated, and no evidence of mantle cell lymphoma or CCND1 rearrangement was detected, concluding a diagnosis of extranodal marginal zone lymphoma.
Upon follow-up, the patient's symptoms had resolved, and imaging studies showed no residual pelvic mass.
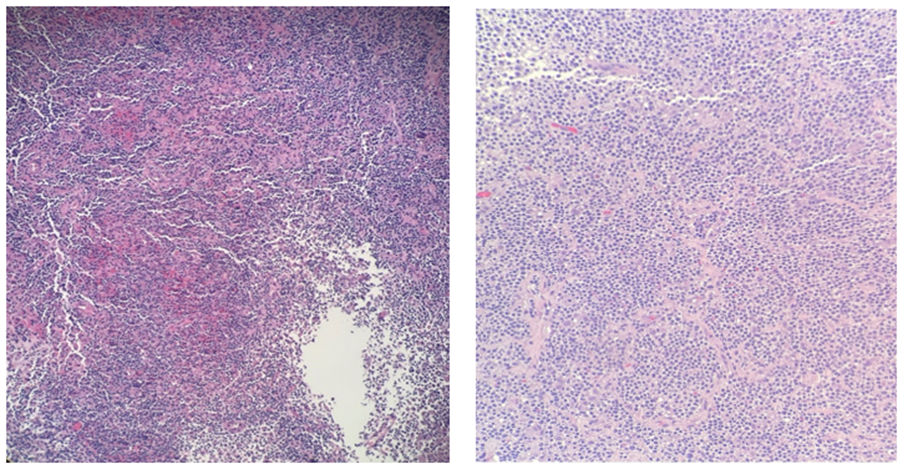
a) H&E x 100 b) H&E x 200
Figure 1: H&E sections, low power showing a mixture of inflammatory cells; histiocytes, plasma cells and lymphoid cells, with blood vessels.
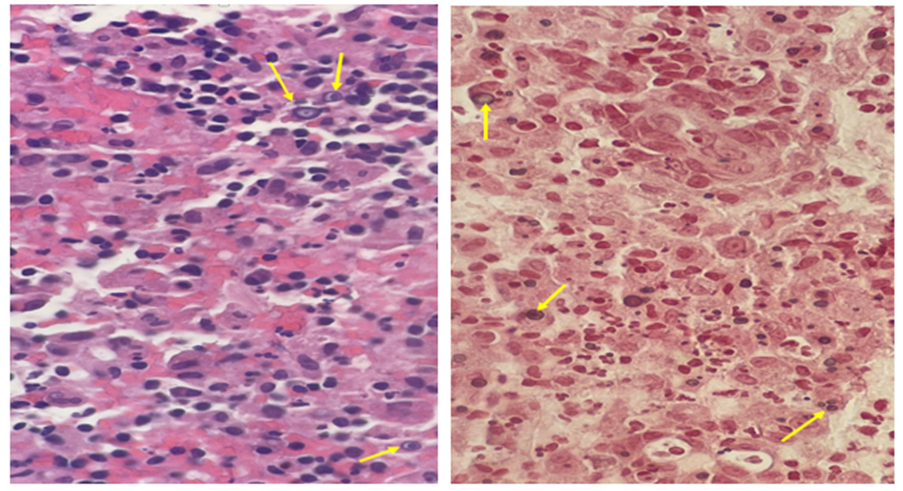
a) H&E x 400 b) Von Kossa stain x 400
Figure 2: High power sections demonstrating von Hansemann cells and Michaelis-Gutmann bodies. Yellow circles mark Michaelis-Gutmann bodies
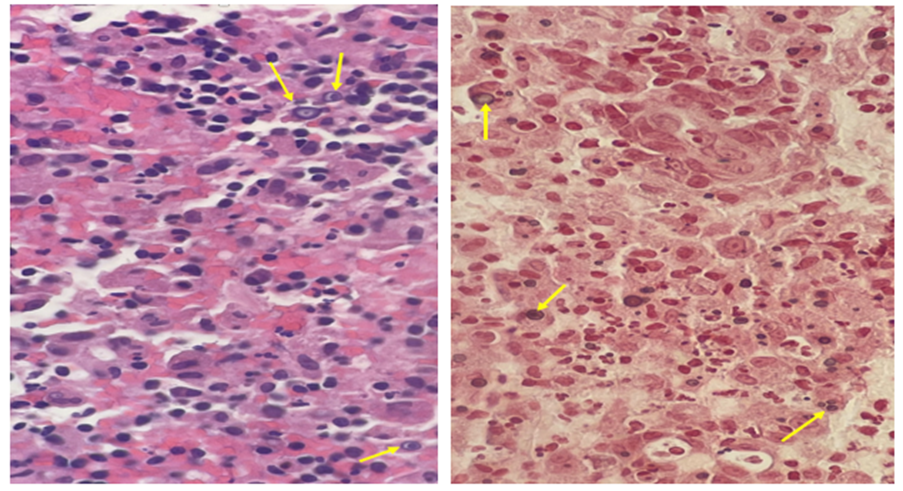
c) H&E d) Von Kossa stain
Figure 2: Zoomed-in pictures demonstrating von Hansemann cells and Michaelis-Gutmann bodies. Yellow arrows mark Michaelis-Gutmann bodies
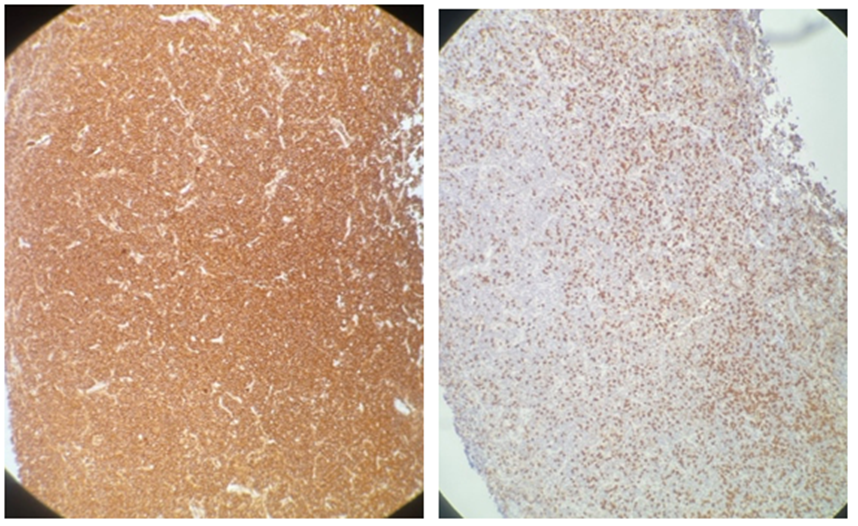
a) CD20 shows Strong and confluent expression b) CD3 highlights reactive T cells in the background
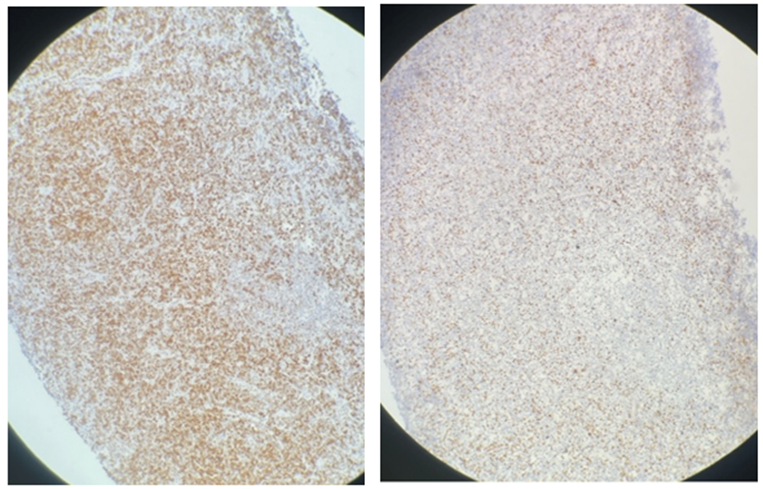
c) BCL2 shows partial expression by B cells d) Cyclin D1 is expressed by about 30% of the cells
Figure 3: Immunohistochemistry of the lymphoid cells.
Primary lymphomas of the female genital tract (PLFGT) are rare and can often mimic gynecological malignancies, posing a diagnostic dilemma [7&8]. According to the National Cancer Database, only 1.5% of extranodal non-Hodgkin lymphomas originate in the female genital tract [9]. Clinically, PLFGT present with nonspecific symptoms or abnormal vaginal bleeding, but systemic B symptoms are infrequent [3]. The prognosis for localized PLFGT is generally favorable, with radiation therapy being the recommended first-line treatment due to its high response rates and low morbidity [1].
Primary female genital tract (FGT) MALT lymphoma is an indolent disease, and the stimulus for its development is generally unknown. However, it can be associated with infections or autoimmune diseases, similar to MALT lymphoma in other locations. For instance, Noack et al. reported a case of tubal marginal zone lymphoma (MZL) with salpingitis [10], and Magnoli et al. described a case of endometrial MALT lymphoma associated with rheumatoid arthritis [11]. Diagnosing MALT lymphoma requires histological identification of proliferative monoclonal CD5−, CD10− marginal zone B cells in diffuse and vaguely nodular patterns. Clonality can be confirmed by immunophenotyping or gene rearrangement studies [4]. It is crucial to differentiate indolent MALT lymphoma from more aggressive lymphomas requiring intense therapy. Cyclin D1 is typically expressed in mantle cell lymphoma due to CCND1 rearrangement and can stain histiocytes, serving as an internal control. In our case, cyclin D1 expression in a subset of cells necessitated additional molecular testing for CCND1 to rule out mantle cell lymphoma, which requires systemic chemotherapy. Aberrant cyclin D1 staining in MZL, though rare, can occur [12].
Malakoplakia was first described by David Paul von Hansemann in 1901 and later reported by Leonor Michaelis and Carl Gutmann [13]. It is a chronic granulomatous disease caused by bacterial infection, impaired systemic immune response, and impaired local macrophage response [5].
While the urinary tract, particularly the bladder, is the most common site of malakoplakia, involvement of the FGT is rare [13]. FGT malakoplakia may present with abnormal vaginal bleeding, as seen in our patient, who experienced cessation of bleeding after receiving azithromycin [14].
Histologically, malakoplakia is characterized by sheets of large histiocytes with foamy pink cytoplasm, von Hansemann cells, and Michaelis-Gutmann bodies. These bodies result from phagolysosomal fusion and subsequent mineralization and can be highlighted by the von Kossa stain (Figure. 2) [15]. Despite its rarity, the association of malakoplakia with lymphoma has been documented in the literature [15-17].
PLFGT are not commonly encountered and should be considered in the differential diagnosis alongside more common gynecological lesions. Early diagnosis is challenging and requires integrating all available information and ancillary tests. Clinicopathological correlation is crucial for a definitive and accurate diagnosis.
We propose some key points to avoid misdiagnosis and guide clinicians toward appropriate treatment. Granulation tissue usually results from prior insults such as malignancies, radiation therapy, and injuries. A rapidly growing mass is often indicative of a neoplastic process. A lymphocyte-abundant lesion without neutrophils suggests a process beyond what is typical for malakoplakia. Confluent staining of CD20, which marks B cells, implies a lymphoproliferative process.
Pathologists can better differentiate between PLFGT and other gynecological conditions by paying close attention to these factors, ensuring timely and accurate treatment.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
