
Case Report | DOI: https://doi.org/10.31579/2768-2757/065
1 General Surgeon, Emergency Department, General acute hospital donation Francisco Santojanni, Argentina.
2 General Surgeon and Trauma, Emergency Department, General acute hospital donation Francisco Santojanni, Argentina.
3 General and vascular surgeon, Emergency Department, General acute hospital donation Francisco Santojanni, Argentina.
4 General and trauma surgeon, gastroenterology and endoscopy, Emergency Department, General acute hospital donation Francisco Santojanni, Argentina.
*Corresponding Author: Federico E. Labanca, general Surgeon, Emergency Department, General acute hospital donation Francisco Santojanni, Argentina.
Citation: Federico E. Labanca, Patricia M. Delnero, Alonso V., Raúl E. Paganini., (2023), Computed Tomography With 3d Reconstruction for The Diagnosis of Traumatic Urethral Injuries, Journal of Clinical Surgery and Research, 4(1); DOI:10.31579/2768-2757/065
Copyright: © 2023, Federico E. Labanca. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 February 2023 | Accepted: 17 February 2023 | Published: 01 March 2023
Keywords: trauma; urethra; tomography; 3D reconstruction
The retrograde urethrogaphy is considered the Gold Standard method used for diagnosis of urethral injury. We present a patient in which computed tomography with 3D reconstruction with endovenous and endourethral contrast is performed, allowing us to reconstruct the urethra in a three-dimensional form making possible to diagnose urethral injuries as well as others of the entire urinary tract, solid or hollow organs and pelvic ring injury, in the context of acute trauma, with high sensitivity and specificity without other complementary studies.
In August of 1087, the King William I of England was riding a horse when he suffered an incident, the doctor realized that his bulbar urethra was injured, evidenced by the change of his urine´s color, it was considered a fatal injury at that moment, and so he died a few months later1. With the advent of new technologies, the severity of these injuries was relegated in history, generally having a favorable course with on term diagnosis.
Urethral injuries are rare in emergency departments; they commonly follow an acute trauma, most of them as a consequence of blunt trauma, whether or not associated with pelvic fracture.
People in their third and fourth decade of life are more frequently affected, with a slight predominance in men, because of the longer (para mi esto en rojo no va) length of their urethra and its means of fixation [2]. Patients could be asymptomatic or present symptoms like perineum or groin pain, perineum and scrotum hematoma, distended bladder (aca quiero poner globo vesical) Vero lo buscó y se dice así, no nos sonaba el baloon, impossibility to urinate, associated urethrorrhagia whose quantity cannot be related to the severity of the injury.
It should always be suspected in any pelvis and perineum blunt trauma, even though the rate of traumatic urethral injury is less than 1.5% of the total of trauma, affecting 1/45.000 inhabitants per year [3].
The mechanism of injury is divided into an iatrogenic group (for example, the urethral injury made by the catheterization that affects 3.2/1.000 patients at hospital) and non – iatrogenic- traumatic, that is the most frequent and severe, since it requires a greater force (trauma) to injure the urethra. Straddle injuries, such as fallings or incidents with motor vehicles are examples of these traumatic injuries, commonly seen at the emergency department.
The classification according to the degree of injury may be contusion, complete or partial ruptures, and according to the anatomical location [4], could be anterior or posterior portion of the urethra. The latter generally is associated with pelvic fracture according to the American Association for Surgery of trauma classification.
Currently, multi-slice computed tomography scanners perform high-resolution images with three-dimensional reconstructions; so Computed Tomography Urography is the method preferred for evaluating the urinary tract, replacing the traditional retrograde urography, in patients with urine bleeding and risk factors for developing cancer [5]. Although the Computed Tomography Urography allows us to evaluate the collecting systems, ureters and bladder, but it is not possible to study the entire urethra with this method, since it has not been possible to replace retrograde urethrography to make radiological diagnosis of urethral injuries yet [5].
The aim of this clinical case is to demonstrate through a single complementary study with 3D reconstruction, that is possible to both diagnose a urethral injury and plan the specific treatment, knowing the location, size, and severity of the injury, and at the same time it could be useful for the diagnosis all pathologies associated with acute trauma, like solid or hollow organ injury or bone injuries.
An 18 years old male patient was presented in the emergency department with symptoms of pain, urinate inability, and small amount of hematuria; he referred an incident, collision of motorcycle with genital blunt trauma. On physical examination, he presented twelve points of Revised Trauma Score, without perineum injury, with mobility of his four limbs. Blood test performed within normal parameters, a retrograde uretrography (Figure 1) and abdomen and pelvis Computed Tomography with 3D reconstruction with endovenous and endourethral contrast (Figure 2) was performed. These studies showed a partial urethral injury in the posterior location, with contrast leak, and five milimeters distance between both ends, associated with an iliac crest line fracture that did not require any surgical treatment.
He was surgically intervined in the Emergency room with a percutaneous suprapubic cystostomy, and in a second time, the Urology Department performed a cystoscopy, confirming the diagnosis, performing a urethra`s catheterization for subsequent endoscopic repair of the injury satisfactory.
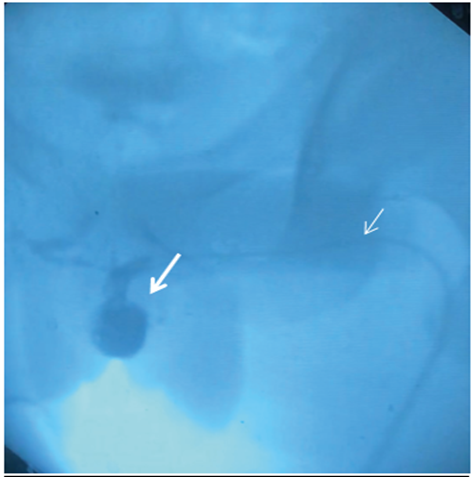
Figure 1: Retrograde urethrography with endourethral contrast where the larger arrow indicates contrast leakage in the posterior urethra and the smaller arrow indicates the bladder catheter through which the contrast substance is instilled.
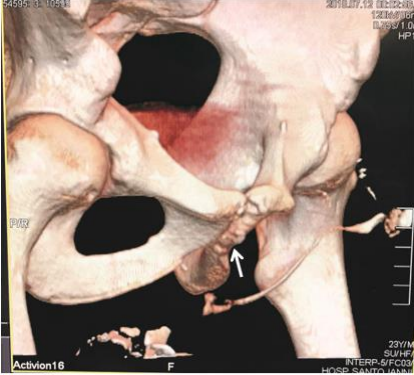
Figure 2: Multislice computed tomography with 3D reconstruction where the arrow indicates the lesion of the posterior urethra with a distance between ends of 5mm, patent urethra with passage of contrast to the bladder.
There is no published evidence of the use of computed tomography multislice 3D reconstruction with endourethral contrast as a method of diagnosis of urethral injury. According to our experience as a trauma center, this method allows to evaluate the location of the urethral injury, the distance between both ends, as well as other associated injuries, such as a pelvic ring fracture or intra-abdominal organs injuries. In the literature revised, we found tomographic indirect signs that reveal a probable urethra injury such as: contrast extravasation, high riding prostate gland, ischiocavernosus muscle hematoma, distortion and obscuration of the prostate contour and bulbocavernosus muscle, that is more frequently associated with complicated pelvic fractures and those cannot be seen in retrograde urethrography [6]. The Gold standard technique used to diagnose these lesions is the retrograde urethrography, it needs 20-30 milliliters of water-soluble contrast administered through the urethral meatus. This method has the advantages that it is cheaper and faster than computed tomography, which is quite important in Public Health Centers, but still little conclusive as for the degree of injury, the distance between both ends, the location and anatomic features6. As already mentioned, the use of computed tomography for diagnosis of intra-abdominal urinary tract is widely accepted due to its great sensitivity and specificity, and so is the use of magnetic resonance imaging for the diagnosis urethral injury. In this case the trauma team performed a retrograde urethrography and a computed tomography with intravenous and hydro-soluble contrast administrated through the urethra to reconstruct the urinary tract from the kidney to the meatus and made possible the diagnosis of associated injuries in the context of acute trauma, while also scanning other parts of the body such as the chest or brain. It was useful for the Urology team, as the patient was immediately treated with endoscopic bladder catheter. The disadvantages of this method are the cost and availability of this equipment in health’s center. At our hospital we have compute tomography Aquilian Toshiba [1, 6]. But we emphasize that this disease has a low frequency and usually these injuries occur in the big cities and their management is carried out in healthcare´s center that has this type of scanner.
The indisputable advantage of this technique is being able to identify greater associated injuries with just one Imaging examination and imparting simultaneous treatment or priority treatment to the lesion of the final urinary system, without the need to perform any other complementary methods such as radiography, retrograde urethrography, which would delay patient's treatment. As a working group of traumata, we propose a possible change in the gold standard diagnosis of this pathology given the benefits found with this technique.
None Declared.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
