
Research Article | DOI: https://doi.org/10.31579/2641-0419/173
*Corresponding Author: Akbar Molaei, Pediatric cardiologist, Shahid Madani Hospital, Tabriz Iran,
Citation: Ahmad J. Khosroshahi, Mahmoud Samadi, Akbar Molaei., (2021) Complete heart block after open heart surgery in children with congenital cardiac diseases Feasibility of more waiting time before PPM administration. J. Clinical Cardiology and Cardiovascular Interventions, 4(11); Doi:10.31579/2641-0419/173
Copyright: © 2021 Akbar Molaei, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 April 2021 | Accepted: 11 May 2021 | Published: 17 May 2021
Keywords:
Introduction: Congenital cardiac disorders are the most prevalent congenital disorders which require interventional or surgical treatments. The most common causes of complete heart block (CHB) are degeneration of cardiac conduction system, acute myocardial infarction and congenital cardiac disorders. CHB after congenital heart surgery is of paramount importance which causes post-operation death and heart failure.
Application of a pacemaker is a standard treatment for CHB. The purpose of this paper is to study the frequency of early postoperative CHB in patients with congenital cardiac diseases and also the need for temporary (TPM) and permanent (PPM) pacemakers.
Materials and methods: This descriptive-analytical and cross-sectional study was conducted on children with congenital heart defects who had undergone open-heart surgery in Tabriz’s Shahid Madani Hospital from 2011 to 2016. Patients with early postoperative CHB were included in the study. Those who had improved on their own and those who needed TPM and PPM were identified and at the end, the frequency of CHB and the need for TPM and PPM were assessed.
Results: Of the 2100 operated patients, 109 patients developed early postoperative heart block. The frequency of early CHB after open heart surgery was 5.19%. Of the 109 patients, 69 patients (63.3%) with early postoperative CHB needed TPM, 9 patients needed PPM and 22 patients improved without pacemaker.
Conclusion: The prevalence of early CHB in patients operated for congenital cardiac diseases was 5.19%. The need for TPM was high and most of the patients had improved cardiac rhythm with no need for PPM or TPM.
Permanent complete heart block (CHB) is a significant complication of intracardiac repair for congenital heart disease. It refers to post-operative heart block that does not spontaneously revert to the pre-operative rhythm (usually within 10 days of the operation). Treatment entails lifelong dependence on an artificial pacing system requiring replacement at least once every decade. The relevant part of the cardiac conduction system in this setting is the atrioventricular (AV) node and the bundle of His. Improved surgical techniques and better understanding of the anatomy of the conduction tissue in various congenital cardiac anomalies have reduced this risk to 1–4% in the current era.
Cardiac conduction disorders (especially atrioventricular conduction) are among the important complications following congenital open-heart surgeries [1, 2, 3]. In CHB with cardiac conduction system defect, no conduction passes through the atrioventricular (AV) node and atrioventricular dissociation will occur [3]. In CHB, escape rhythm may arise from the AV node resulting in narrow QRS in the ECG, but if the scape rhythm occurs below this node and Purkinje system occurs in the cardiac conduction system, then wide QRS will be seen in the ECG [3]. The most common causes of CHB are degeneration of cardiac conduction system, acute myocardial infarction and congenital cardiac disorders [4].
Over the last 2 decades, reports from single or few institutions have been published describing the incidence of postoperative heart block. However, the true incidence of this complication in a large cohort of patients is unknown [5].
These disorders sometimes require embedding a TPM or PPM. The incidence of CHB affects the length of hospital stay, morbidity and even in-hospital mortality [6,7,8]. Transient CHB can be a risk factor for late CHB [9]. The risk factors for postoperative CHB include age, sex, weight, endocarditis, and aortic valve replacement [10]. Use of a pacemaker is a standard treatment for postoperative CHB [11]. If no pacemaker is embedded, the mortality rate from postoperative permanent CHB varies from 28 to 100 percent [12]. Transient CHB will usually disappear in 7 days in most of the cases and the 7th day of block persistence is a good time for embedding a PPM [10].
Considering the advances in state-of-the-art surgical techniques, differences in types of surgery and the amount and types of hospital facilities, this study was conducted in Tabriz’s Shahid Madani Hospital at the north west of Iran to investigate the frequency of early CHB after open heart surgery in children and also the need for TPM and PPM [12,13]. Study ethical license No was Ir.tbzmed.rec.1397.555.
Materials and methods
This descriptive-analytical and cross-sectional study was conducted on 1-month to 15-year-old patients with congenital cardiac diseases who had undergone open heart surgery from 2011 to 2016.
Medical histories of the patients were completely reviewed.
Patients who were older than 15 years, their medical history was incomplete, and those with a history of preoperative heart block were excluded from the study.
The sample size was calculated at 90 patients based on a 95% confidence interval, an 80% test’s power and a 5% acceptable error rate. Considering the existing resources, 109 patients with early CHB were included in the study.
Medical histories of the 2100 patients who had undergone open heart surgery during 2011-16 and had developed CHB were reviewed. The pieces of information obtained were demographic information, type of congenital disease, block type, need for pacemaker, no need for TPM and/or PPM, time interval between surgery and CHB onset and termination, duration of the need for TPM and, the need for PPM, and length of hospital stay.
The rate of postoperative CHB, the number of cases who had improved on their own, and those who needed TPM and PPM were identified and the collected data were analyzed in SPSS version 22.
Of the 2100 patients with congenital cardiac diseases who had undergone open heart surgery, 109 patients, whose demographic information is presented in table 1, developed early CHB.

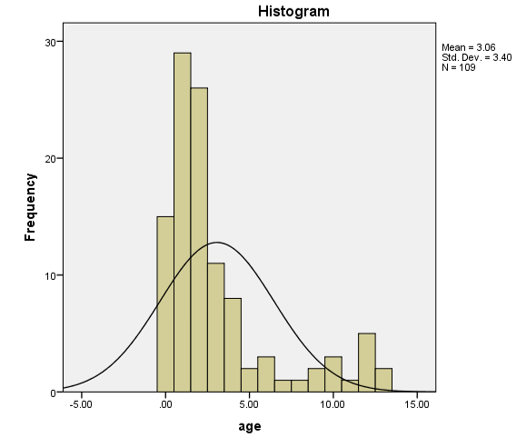
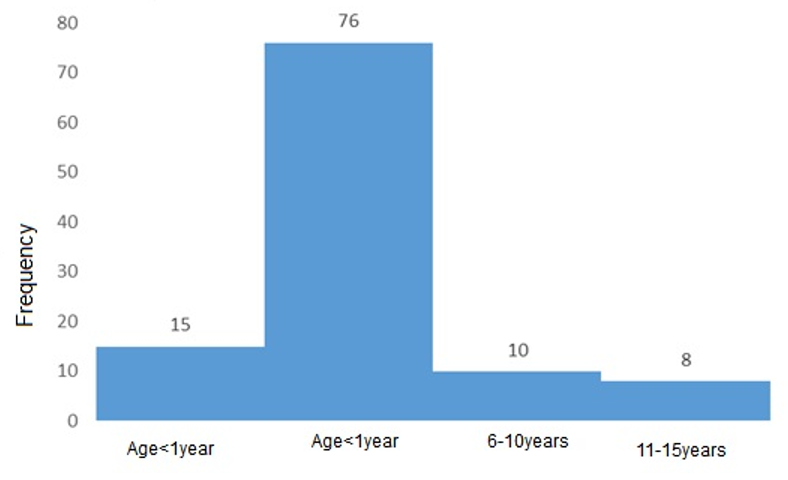
The patients’ age varied from 2 months to 15 years. The age range of the patients who had developed early CHB varied from 4 months to 13 years and the mean age of the patients was 3.33±3.14. Most of the patients with early CHB aged 1-5 years. The frequency of this age group was 76 patients or 69.72% (diagrams 1 and 2).
Of the 109 CHB patients, 62 patients (56.6%) were male 47 (43.1%) were female. The patients weighed from 3.5 kg to 36 kg and the mean weight was 7.49 kg. The weight distribution of the patients is shown in diagram 3.

Of the 109 operated patients with early CHB patients, 69 patients (63.3%) or 3.28% of all of the patients, needed TPM and only 9 patients (8.3% of patients with postoperative CHB) or 0.42% of all of the patients ultimately needed PPM.
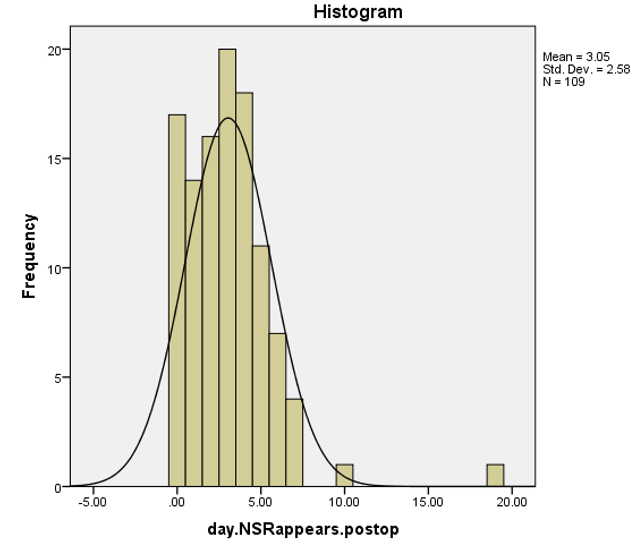
Heart block occurrence varied from the day of operation to 4 days after. The average number of days after the operation when CHB had appeared was 0.61+/-0.69 day with a frequency of 52 patients after the operation (diagram 4).

The time interval that the rhythm would return to normal sinus rhythm after CHB, varied from 1 to 19 days with average of 3.63 days (diagram 5).
The time when the patients required PPM varied from 14 to 28 days after the operation with an average of 17.11±4.34 days (table 2).

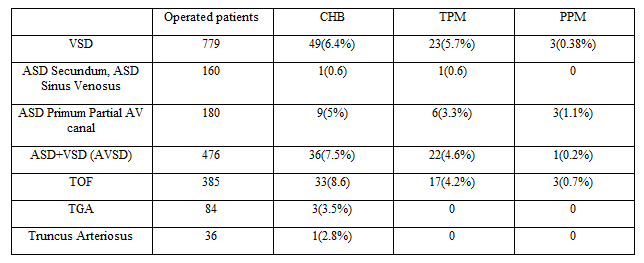
The frequency of the type of preoperative congenital heart diseases and the counterpart need for TPM and PPM is summarized in table 3.
Tremendous advances in the surgical management of congenital heart disease (CHD) have been achieved over the past half century. Nevertheless, the conduction system injury continues to be a leading cause of long-term postoperative cardiac morbidity, especially with performance of more surgical procedures in increasingly younger patients. Transient or permanent CAVB is not a common complication after congenital heart surgery, and the frequency has been reported to range from 0.5% to 3% in wide series in the literature.
CHB following surgical repair may be transient or permanent. Transient CHB in this setting generally reverts to sinus rhythm within the first 7–10 days after surgery though recovery several months later is not unknown. By definition then, permanent CHB is not expected to exhibit spontaneous recovery. The occurrence of CHB after open-heart surgeries, especially when patients have conotruncal lesions, has long been a concern for doctors and researchers.
The importance of accurate diagnosis and inspecting the prevalence of CHB after open-heart surgeries, besides being rooted in epidemiological considerations and the effects of CHB anatomical factors, has been more related to advancement of surgical techniques for cardiac congenital diseases, identifying the need for TPM, PPM and the best time to embed a PPM, and the outcomes of CHB. This is because it has been shown that the incidence of CHB affects the length of hospital stay and the rates of morbidity and mortality.
That is why pediatric surgeons and cardiologists should be completely informed about the prevalence of CHB in their centers and how to face this complication so that they would be prepared to handle it and take the necessary measures to minimize subsequent complications; they also should seek solutions to reduce the incidence of CHB through using state-of-the-art techniques and appropriate instruments during surgery.
In this study, 91.7% of the early postoperative CHB patients improved with or without a TPM and did not require a PPM and 8.3% of the patients needed PPM.
63.3% of the CHB patients required a TPM, while 28.4% improved without a pacemaker which seems to be higher compared to other centers and studies about the postoperative CHB prevalence, but the need for PPM was less than what has been reported in other centers and studies [14,15,16]. This finding may be an indication of the fact that the likelihood of recovery from CHB is more than reported numbers in these patients and therefore they should be under surveillance for a longer period before embedding a PPM for such patients [17].
Tremendous advances in the surgical management of congenital heart disease (CHD) have been achieved over the past half century. Nevertheless, the conduction system injury continues to be a leading cause of long-term postoperative cardiac morbidity, especially with performance of more surgical procedures in increasingly younger patients. Transient or permanent CAVB is not a common complication after congenital heart surgery, and the frequency has been reported to range from 0.5% to 3% in wide series in the literature.
CHB following surgical repair may be transient or permanent. Transient CHB in this setting generally reverts to sinus rhythm within the first 7–10 days after surgery though recovery several months later is not unknown. By definition then, permanent CHB is not expected to exhibit spontaneous recovery. The occurrence of CHB after open-heart surgeries, especially when patients have conotruncal lesions, has long been a concern for doctors and researchers.
The importance of accurate diagnosis and inspecting the prevalence of CHB after open-heart surgeries, besides being rooted in epidemiological considerations and the effects of CHB anatomical factors, has been more related to advancement of surgical techniques for cardiac congenital diseases, identifying the need for TPM, PPM and the best time to embed a PPM, and the outcomes of CHB. This is because it has been shown that the incidence of CHB affects the length of hospital stay and the rates of morbidity and mortality.
That is why pediatric surgeons and cardiologists should be completely informed about the prevalence of CHB in their centers and how to face this complication so that they would be prepared to handle it and take the necessary measures to minimize subsequent complications; they also should seek solutions to reduce the incidence of CHB through using state-of-the-art techniques and appropriate instruments during surgery.
In this study, 91.7% of the early postoperative CHB patients improved with or without a TPM and did not require a PPM and 8.3% of the patients needed PPM.
63.3% of the CHB patients required a TPM, while 28.4% improved without a pacemaker which seems to be higher compared to other centers and studies about the postoperative CHB prevalence, but the need for PPM was less than what has been reported in other centers and studies [14,15,16]. This finding may be an indication of the fact that the likelihood of recovery from CHB is more than reported numbers in these patients and therefore they should be under surveillance for a longer period before embedding a PPM for such patients [17].
The prevalence of CHB was not high in the patients operated for congenital cardiac diseases and was around 5.19%. Given its clinical importance, this rather small amount is significant and slightly higher than other centers. The need for TPM was high and most of the patients ultimately improved with or without a TPM. The need for PPM was found to be 0.42% which is higher than some studies and lower than several others.
The average time when PPM had been used after the surgery was 17.11±4.34 days which is more in comparison with previous studies. By considering the more wait time before PPM insertion and low percentage of the PPM requirement it may be feasible to wait more (about two weeks) before PPM administration.
Taking the clinical significance of CHB and other influential factors into account, complementary research studies are required for better and efficient decision-makings.
For sure having the possibility of getting hands on sufficiently enough number of patients, with accurate information, which were the limitations of this study, will give us more accurate results and can be considered in subsequent studies.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
