
Case Report | DOI: https://doi.org/10.31579/2578-8965/211
Reproductive Endocrinology and Infertility Atrium Health Fertility Center 1025 Morehead Medical Plaza Unit 500 Charlotte, NC 28204.
*Corresponding Author: Bradley S Hurst, Reproductive Endocrinology and Infertility Atrium Health Fertility Center 1025 Morehead Medical Plaza Unit 500 Charlotte, NC 28204.
Citation: Kathryn M Goldrick, Michelle L Matthews, Rebecca S Usadi, Tasha L Gill, Bradley S Hurst, (2024), Comparison of Two Types of Endometrial Scratch before Embryo Transfer and Patient-Reported Pain Scores: A Prospective Randomized Pilot Study, J. Obstetrics Gynecology and Reproductive Sciences, 8(3) DOI:10.31579/2578-8965/211
Copyright: © 2024, Bradley S Hurst. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 March 2024 | Accepted: 27 March 2024 | Published: 05 April 2024
Keywords: endometrial scratch; assisted reproductive technology; in vitro fertilization
Background: The impact of various methods of endometrial scratch during assisted reproductive technology (ART) is not well established.
Objective: To compare patient-reported pain scores and ART outcomes following two types of endometrial scratch prior to embryo transfer.
Study design: In this prospective, non-blinded, randomized controlled trial, patients were assigned to either Pipelle or Shepard catheter. The primary outcome was mean pain score. Secondary outcomes included implantation rate (IR) and clinical pregnancy rate (CPR).
Results: One hundred seventy transfers were included (Pipelle: n=78, Shepard: n=92). Mean pain scores were significantly lower in the Shepard group compared to the Pipelle group (3.0±2.4 vs. 3.9±2.2, respectively; p=0.01). There was no significant difference in IR (Shepard: 59.7%±52 and Pipelle: 56.5%±48; p=0.9) and CPR (Shepard: 67.6%±47 and Pipelle: 71.8%±45; p=0.6).
Conclusions: In our study, the Shepard catheter was a less painful method of endometrial scratch without compromising ART outcomes.
In the United States, approximately 2.3% of infants are conceived using assisted reproductive technologies (ART) (1). Over the past three decades, there have been significant improvements in clinical outcomes of ART procedures. Notably, implantation and clinical pregnancy rates associated with in vitro fertilization (IVF) are 35% and 40%, respectively (2, 3). Interventions such as endometrial scratch have been evaluated to improve implantation and ART success. Endometrial scratch, a procedure that involves intentional disruption of the endometrium prior to embryo transfer, may increase endometrial receptivity and implantation (4-6). However, while some studies suggest that endometrial scratch prior to embryo transfer may improve implantation rates and clinical pregnancy rates, patients report experiencing moderate pain and discomfort during the endometrial scratch procedure (6-10)
Endometrial scratch is associated with significantly higher pain scores compared to patients who did not receive endometrial scratch during ART (11). In a multicenter randomized control trial of 1,364 patients, the median pain score reported by patients who underwent endometrial scratch was 3.5 out of 10 on a visual analogue scale (IQR=1.9-6.0) (Lensen, 2019). Furthermore, two additional studies found patients who underwent endometrial scratch experienced moderate to severe pain with mean pain scores of 6.42 and 6.93 (11, 12). However, these studies utilized the Pipelle catheter for endometrial biopsy. To our knowledge, no studies have assessed pain scores in women who underwent endometrial scratch using the Shepard intrauterine insemination catheter.
The objective of this study was to compare the effects of two endometrial scratch techniques – an endometrial biopsy with a Pipelle catheter and a four-quadrant endometrial scratch using a Shepard insemination catheter – on patient-reported pain scores. Through this study, we aim to elucidate implications for clinical practice of endometrial scratch during ART for women undergoing IVF procedures, to achieve comparable ART success while minimizing patient discomfort.
Study Design and Participants
This prospective, non-blinded randomized controlled trial with parallel treatment arms was conducted from 2014 to 2017 at an academic fertility center. This study was reviewed and approved by the Carolinas Healthcare System Institutional Review Board. Patients undergoing embryo transfer who were in the cycle prior to their planned embryo transfer were included in this study. Patients who did not undergo an embryo transfer, had a known pregnancy, active pelvic infection, known endometrial hyperplasia or cancer, inability to tolerate endometrial catheter placement, severe cervical stenosis, and patients who were planned for operative hysteroscopy in the cycle prior to embryo transfer were excluded.
Randomization
Patients were randomized by a random number generator for allocation to either: 1) endometrial biopsy with a Pipelle catheter or 2) four-quadrant endometrial scratch with a Shepard insemination catheter.
Endometrial Scratch Technique
Patients were scheduled for the endometrial scratch procedure during days 21-27 of the cycle prior to embryo transfer. For patients in the Shepard catheter group, a four-quadrant technique was performed by inserting the Shepard catheter to reach to uterine fundus then rotating it in quarter-turns at the 12:00, 3:00. 6:00, and 9:00 o’clock positions.
The Shepard catheter has a 1.8 mm diameter tip that is smaller than the Pipelle, more pliant, and can curve the tortuous endocervical canal. This catheter is frequently utilized to perform saline infusion sonogram (SIS) in our clinic.
In the Pipelle group, the endometrial biopsy technique was performed using the Pipelle catheter. The Pipelle was inserted into the upper section of the intrauterine cavity. Suction was applied while rotating the catheter during withdrawl to remove an adequate endometrial tissue sample. Endometrial disruption was confirmed via ultrasound. The remainder of the IVF cycle and embryo transfer proceeded in accordance with standard institutional protocol.
Pain Scores:
The primary outcome was pain scores. Patients were given a Numerical Rating Scale (NRS) to assess pain immediately following the endometrial scratch procedure for both techniques. Pain was assessed using a visual analog scale of 1-10, where 1 represented no pain and 10 indicated maximum pain (13). Secondary outcomes included implantation rate and clinical pregnancy rate. Implantation rate was defined as the number of fetal sacs per embryos transferred. Clinical pregnancy was confirmed by ultrasound and measured as the rate of pregnancies per embryo transfer.
ART Cycles:
Demographic and ART outcome data were recorded from electronic medical records. Demographic data included age, sex, and ethnicity. Data on the number of embryos, embryo transfer, implantation, and positive pregnancy tests were collected within 1 year after the last embryo transfer.
Descriptive statistics of the sociodemographic and ART characteristics were used to describe the study population. Mean and standard deviation were used for continuous, while categorical variables were described using frequencies and percentages. Mann Whitney U or student’s t-test was used to compare pain scores across groups. Implantation rates and clinical pregnancy rates were compared using chi-square test. Statistical significance was set at p less than0.05. Data were analyzed in partnership with statisticians from the Carolina Medical Center’s Dickson Advanced Analytics using DA2 software.
A total of 162 patients were recruited and 29 of these patients were re-randomized in subsequent embryo transfer cycles. Of the 195 transfers included in this study, 25 cycles were excluded for cervical stenosis, patient intolerance of procedure, patient drop-out of study, and no available embryos for transfer. Thus, 170 transfers remained. Seventy-eight patients were assigned to the to the Pipelle arm, and 92 patients were randomized to the Shepard arm (Figure 1).
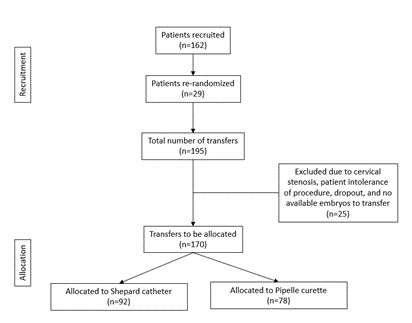
Figure 1: Flow diagram of participants.
The two groups were well-balanced with regard to age, body mass index (BMI), number of prior live pregnancies, and AMH (Table 1). The mean age for the Pipelle and Shepard catheter groups was 33.8 and 34.2 years, respectively. There were no significant differences in the number of prior pregnancies and prior live births. In addition, there were no significant differences in ART cycle characteristics between the two groups (Table 2).
| Pipelle (n=78) | Shepard (n=92) | p-value | |
| Maternal age | 33.8 ± 4.6 | 34.2 ± 3.9 | 0.6 |
| BMI | 24.9 ± 4.3 | 24.8 ± 5.5 | 0.9 |
| Number of prior pregnancies | 0.9 ± 1.1 | 1.1 ± 1.3 | 0.3 |
| Number prior live births | 0.4 ± 0.7 | 0.4 ± 0.6 | 0.9 |
| AMH | 4.2 ± 3.3 | 4.4 ± 4.0 | 0.9 |
Data reported as mean ±SD.
Table 1: Demographic characteristics of the Pipelle and Shepard catheter groups.
| Pipelle (n=78) | Shepard (n=92) | |
PGT-A/PGT-D Screened Unscreened |
27 (35) 50 (65) |
37 (42) 52 (58) |
Type cycle Fresh Frozen |
1 (1) 77 (99) |
2 (2) 90 (98) |
| Donor egg | 5 (6) | 6 (7) |
Type of freezing Slow freeze Vitrification |
0 (0) 77 (100) |
3 (3) 85 (97) |
| Number eggs retrieved | 17.8 ±9.0 | 19.1 ±10.3 |
| Number eggs fertilized | 10.9 ± 5.7 | 11.1 ± 6.7 |
| Number embryos transferred | 1.1 ± 0.2 | 1.1 ± 0.3 |
| Number eggs retrieved | 17.8 ±9.0 | 19.1 ±10.3 |
| Number eggs fertilized | 10.9 ± 5.7 | 11.1 ± 6.7 |
| Number embryos transferred | 1.1 ± 0.2 | 1.1 ± 0.3 |
Data reported as n (%) or mean ±SD.
No significant differences were reported.
Table 2: ART cycle characteristics of the Pipelle and Shepard catheter groups.
Pain and ART Outcomes
Patients who underwent endometrial scratch using the Shepard catheter reported experiencing statistically significant lower pain scores compared to patients who received the Pipelle (Shepard: 3.0 ± 2.4 and Pipelle: 3.9 ± 2.2, p=0.01) (Table 3). Although the implantation rate was slightly higher in the Shepard group at 59.7% compared to 56.5% in the Pipelle group, this finding was not statistically significant (p=0.9). Similarly, there was no significant difference in clinical pregnancy rates between Shepard and Pipelle groups (Shepard: 67.6% ±47 and Pipelle: 71.8% ± 45; p=0.6).
| Pipelle | Shepard | p-value | |
| Pain score1 | 3.9 ± 2.2 | 3.0 ± 2.4 | 0.01 |
| Implantation rate | 56.5% ± 48 | 59.7% ± 52 | 0.9 |
| Clinical pregnancy rate | 71.8% ± 45 | 67.6% ±47 | 0.6 |
Data reported as mean ±SD.
1Pain score reported by visual analog scale (1-10).
Table 3: Pain scores and ART outcomes between Pipelle and Shepard Catheter groups.
In this prospective randomized control trial of patients who underwent endometrial scratch prior to embryo transfer, patients who received the Shepard catheter had statistically significant lower pain scores than patients who received the Pipelle. The mean pain scores for both the Pipelle and
Shepard catheter groups were 3.9 and 3.0, respectively. Despite the lower pain scores in the Shepard catheter group, there were no significant differences in implantation and clinical pregnancy rates between the 2 groups.
Patients who received the Pipelle in our study reported a pain score of 3.9, which is congruent with findings from a prior large-scale study that found a median pain score of 3.5 on a visual analog scale among patients who underwent endometrial scratch using the Pipelle (13). While additional studies of endometrial scratch reported pain scores of 6.42 and 6.93, these discrepancies may be due to several factors including differences in ART cycle characteristics, pre-procedure preparations and variability in clinician technique (11, 12). For instance, all patients in the Nastri, Ferriani (11) study received oral contraceptive pretreatment and the majority of these patients had 2 or more unsuccessful embryo transfers, which may contribute to higher patient-reported pain scores.
Findings from this study suggest that patients who underwent endometrial scratch using the Shepard catheter have significantly lower pain scores compared to those who underwent the Pipelle. Low to moderate pain and discomfort are commonly reported by patients who received the Pipelle for endometrial biopsy (7, 8, 10). However, to our knowledge, no prior studies have assessed pain scores and ART outcomes using the Shepard catheter compared to the standard Pipelle. One possible mechanism for patients’ decreased pain with the Shepard catheter is the smaller diameter 1.8 mm compared with the 3.1 mm diameter of the Pipelle. Moreover, the Shepard catheter is malleable while the Pipelle is semi-rigid. Both factors may contribute to decreased pain since the catheters must pass through the cervix for the endometrial scratch procedure. Finally, endometrial scratch using the Pipelle involves removal of endometrial tissue, whereas endometrial scratch with the Shepard catheter involves only endometrial disruption.
There were no significant differences in implantation rates and clinical pregnancy rates across both groups. These findings contribute to the ongoing discussion about the effectiveness of endometrial scratch procedures on ART outcomes. Recent studies have challenged the purported clinical benefits of endometrial scratch (6, 9, 14). In a systematic review of 12 studies involving 3,382 participants undergoing their first cycle of IVF, endometrial scratch had no significant effect on clinical pregnancy rates, and any minimal observed effects on implantation rates was deemed unreliable (9). However, a recent meta-analysis of 41 randomized control trials found that endometrial scratch improved implantation and clinical pregnancy rates in patients undergoing IVF when conducted during the follicular or luteal phase (8). Consequently, our study highlights the importance of optimizing endometrial scratch procedures to reduce patient discomfort, a valuable clinical consideration when the efficacy of specific techniques appears limited.
Endometrial scratch procedures using the Shepard catheter can be performed in office, are relatively quick and easy to use, and incur minimal cost to the patients. Due to the use of the Shepard catheter for saline SIS, we most commonly select a single patient visit during the cycle preceding the ovarian stimulation for IVF. At that time, we accomplish the following procedures in order: 1) trial transfer with a soft embryo transfer catheter, then 2) a saline infusion sonogram with the Shepard catheter using the adjustable sliding positioner of the Shepard catheter to limit fluid back flow, followed by 3) the four quadrant Shepard catheter endometrial scratch. These procedures are completed in one patient visit with a single speculum exam. This practice optimizes patient convenience, lowers procedural costs, and reduces the overall discomfort involved in multiple pelvic exams. While some studies have suggested hysteroscopy as another means of performing endometrial scratch, this modality is more costly, invasive, and time consuming than the two types of endometrial scratch that we chose to study.
The present study maintains several limitations. The lack of blinding in the study design may introduce bias. However, patient-reported pain scores are less likely to be influenced by blinding and secondary outcomes included objective clinical measures such as implantation rate and clinical pregnancy rate. In addition, approximately 10% of patients were excluded due to factors such as cervical stenosis, patient intolerance of procedure, dropout, and absence of embryos for transfer. However, patients were randomized which should potential selection bias. In addition, there were only 3 fresh embryo transfers were performed, which may limit the generalizability of these study findings to fresh embryo transfers. Our study primarily consisted of frozen embryo transfers, which aligns with the growing preference for such procedures within the field and increasing use of preimplantation genetic testing (PGT). Lastly, the relatively small sample size may reduce power to detect significant differences in the study findings. However, this pilot study is the first of its kind to assess pain scores in patients who underwent endometrial scratch using the Shepard catheter. These study findings warrant larger randomized controlled trials in populations with diverse demographic and ART cycle characteristics.
Despite these limitations, this study maintains several strengths. The robust study design as a prospective randomized control trial with parallel treatment arms minimizes selection bias and allows for the control of potential confounding variables. This study design ensures that the differences observed in pain scores are likely attributable to the 2 procedural endometrial scratch techniques. In addition, the visual analog scale is a valid and reliable measure for patient-reported pain scores and has been used to evaluate pain in patients undergoing endometrial scratch (11, 13, 15). Lastly, inclusion of the secondary ART outcomes such as implantation rates and clinical pregnancy rates provided for a comprehensive assessment of the impact of endometrial scratch techniques. Thus, findings from this study provide valuable context for clinical decision-making during ART, particularly for patients undergoing endometrial scratch prior to embryo transfer.
Findings from this study warrant further research to Findings from this study warrant further research to assess the utility of the Shepard catheter in reducing patient-reported pain and discomfort during endometrial scratch procedures and its impact on clinical outcomes. Further research is needed to investigate the impact of using the Shepard catheter on pain and ART outcomes for endometrial scratch procedures in large, diverse samples. Additional studies that explore the biological mechanisms underlying the potential benefits of endometrial scratch in the context of different scratch techniques, such as endometrial disruption, will provide a more comprehensive understanding of the use of endometrial scratch in ART.
In our study, endometrial scratch using the Shepard catheter was a less painful alternative method for women undergoing IVF while maintaining comparable ART outcomes. While the efficacy of endometrial scratching in ART continues to be the subject of scientific discourse, efforts to mitigate patient discomfort during such procedures should be prioritized. The Shepard catheter may be a promising tool for clinicians conducting endometrial scratch prior to embryo transfer. As advancements in ART continue to be developed, strategies that minimize patient discomfort and improve clinical outcomes must be integrated into clinical practice to support patients embarking on the journey of ART.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
