
Research Article | DOI: https://doi.org/10.31579/2641-0419/508
1 University of Zurich, Switzerland.
2 HeartClinic Hirslanden, Zurich Switzerland.
*Corresponding Author: Oliver Gaemperli, MD, FESC, HeartClinic Hirslanden, Witellikerstrasse 40, 8032 Zürich, Switzerland.
Citation: Jonas Schulthess, Patric Biaggi, Peter Wenaweser, Roberto Corti, Jurg Grunenfelder, et al, (2025), Comparison of Transcatheter Edge-to-Edge Repair versus Medical Therapy in Patients with Secondary Mitral Regurgitation A Systematic Review and Meta-Analysis of Published Data, J Clinical Cardiology and Cardiovascular Interventions, 8(13); DOI: 10.31579/2641-0419/508
Copyright: © 2025, Oliver Gaemperli. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 August 2025 | Accepted: 26 August 2025 | Published: 03 September 2025
Keywords: heart failure; secondary mitral regurgitation; transcatheter edge-to-edge repair; systematic review and metaanalysis
Background / Aim: Transcatheter edge-to-edge repair (TEER) is a widely spread treatment option in high-risk surgery patients with heart failure with reduced ejection fraction (HFrEF) and secondary mitral regurgitation (SMR). However, recent randomized controlled trials (RCT) have yielded conflicting results. The aim of this study was to perform a systematic review and meta-analysis of available published evidence comparing TEER with GDMT in patients with HFrEF and SMR.
Materials and Methods: We conducted a systematic search of five online databases (PUBMED / MEDLINE, Cochrane Library, EMBASE, Scopus and Web of Science) and current guidelines for appropriate RCT’s and non-randomized controlled studies (non-RCT’s). Two investigators independently extracted study data and assessed quality. The primary outcomes were heart failure (HF) hospitalizations, all-cause, and cardiovascular (CV) death. We performed a meta-analysis of relative risks (RRs) with 95% confidence intervals (CI) with the Mantel–Haenszel method using a random-effects model. Study risk of bias was assessed for all RCT’s using Cochrane’s Risk of Bias 2 (RoB2) tool.
Results: The literature search identified three appropriate RCT’s (n = 1,423 patients) and six non-RCT’s (n = 1,382 patients). Meta-analysis of the three RCT’s revealed a significant reduction of HF hospitalizations (RR 0.71; 95% CI, 0.56 to 0.90; p=0.005) and non-significant trends towards reduced all-cause and CV death (RR 0.80; 95% CI, 0.63 to 1.02, p=0.07; and RR 0.81; 95% CI, 0.62 to 1.06, p=0.12; respectively) for TEER compared to GDMT. Adding non-RCT’s increased the treatment effect for all three primary endpoints. Furthermore, patient-centred outcomes such as 6-minute walk distance, quality-of-life, and New York Heart Association class showed significant improvement with TEER versus GDMT.
Conclusion: In HFrEF patients with SMR, TEER results in significant reductions of HF hospitalizations, and non-significant trends towards a reduction in all-cause mortality and CV death compared to GDMT.
Mitral regurgitation (MR) is the most prevalent valvular pathology with approximately 1.7% of the general population affected in the United States [1]. Up to one quarter of patients with heart failure and reduced ejection fraction (HFrEF) suffer from severe secondary (also known as functional) mitral regurgitation (SMR) [2, 3]. SMR can be caused by alterations of the geometry of the left ventricle (LV) or the left atrium through mechanisms such as dilated or ischemic cardiomyopathies, myocardial infarction (MI) or atrial fibrillation (AF) [4]. In all cases, SMR increases LV volume overload and is associated with impaired prognosis [5].
Surgical repair or replacement is often considered in severe cases. However, approximately half of patients with severe symptomatic MR are denied surgery due to advanced age, comorbidities and/or poor left ventricular ejection fraction (LVEF) [6]. Furthermore, isolated mitral valve (MV) surgery has not been shown to provide any mortality benefit in patients with SMR [7]. Recently, transcatheter edge-to-edge repair (TEER) has been introduced as a safe and effective alternative to surgical repair: Recent multicentric post-approval registries with the latest-generation TEER devices document reductions of MR severity to mild or less in approx. 9 out of 10 patients with high periinterventional safety profiles (in-hospital mortality less than 2%) [8].
Whether effective TEER of SMR improves patient longevity and reduces HF hospitalizations compared to guideline-directed medical therapy (GDMT) is currently unclear. While observational data suggest improved outcomes of TEER over GDMT [9], recent randomized controlled trials (RCT) have yielded conflicting results [10, 11, 12, 13]. In surgical high-risk patients with severe SMR, current guidelines suggest considering TEER given anatomical suitability of the MV, but based on the current lack of convincing evidence the strength of recommendation is limited (class of recommendation IIa) [14].
Current RCT's are limited by small sample size and underpowered statistics. We hypothesize that this may have resulted in statistical type II errors rendering differences in endpoints insignificant in some trials [10, 11, 12, 13]. Moreover, the trials tended to test for combined endpoints and were generally underpowered to allow any conclusions on the individual components of the composite outcomes. Therefore, the purpose of the present study is to perform a systematic review and meta-analysis of available published evidence comparing TEER with GDMT in patients with HFrEF and SMR.
Literature search
We performed a systematic search of medical articles in peer-reviewed journals published in English, German and French in five online databases (PUBMED / MEDLINE, Cochrane Library, EMBASE, Scopus and Web of Science) using the following search terms in title, abstract or keywords: (mitral regurgitation OR mitral insufficiency) AND (edge-to-edge repair OR percutaneous repair OR MitraClip OR transcatheter valve repair OR transcatheter mitral valve repair OR transcatheter edge-to-edge repair) AND (optimal medical therapy OR guideline-directed medical therapy OR guideline-recommended medical therapy OR medical therapy OR medical treatment). Furthermore, we manually searched the current guidelines for heart failure and valvular heart disease published by the European Society of Cardiology and the American College of Cardiology/American Heart Association.
Study selection / Eligibility criteria
For our main analysis we selected all RCT’s comparing TEER and GDMT in HFrEF patients with SMR. Furthermore, we conducted an extended analysis including also non-randomized studies if they fulfilled the following criteria: (i) two-arm (TEER versus GDMT) clinical trial design, (ii) sample size of at least 80 patients, (iii) MR etiology secondary in at least 70% of patients and (iv) all-cause mortality reported at 12 months. An overview of the search strategy is presented in Figure 1. The abstract screening process was conducted by one reviewer (J.S.) and the full text evaluation was carried out by two independent reviewers (O.G. and J.S.). No automation tools were used in the process.
Outcomes
The primary outcomes of interest were all-cause mortality, CV death and HF hospitalizations. Primary outcomes were assessed at the longest available follow-up. COAPT allowed study participants to cross over from the GDMT to the TEER group after two years. Therefore, data from the two-year follow-up was used even though the five-year follow-up has already been published. Secondary outcomes were residual MR severity, quality-of-life (according to the Kansas City Cardiomyopathy Questionnaire (KCCQ) overall score), 6-minute walking distance (6MWD), and New York Heart Association (NYHA) functional class. Secondary outcomes were assessed from baseline to 12 months follow-up. The latter secondary endpoints were only analysed for RCT’s since no data was available for non-RCT-design studies on these endpoints.
Data extraction and quality assessment
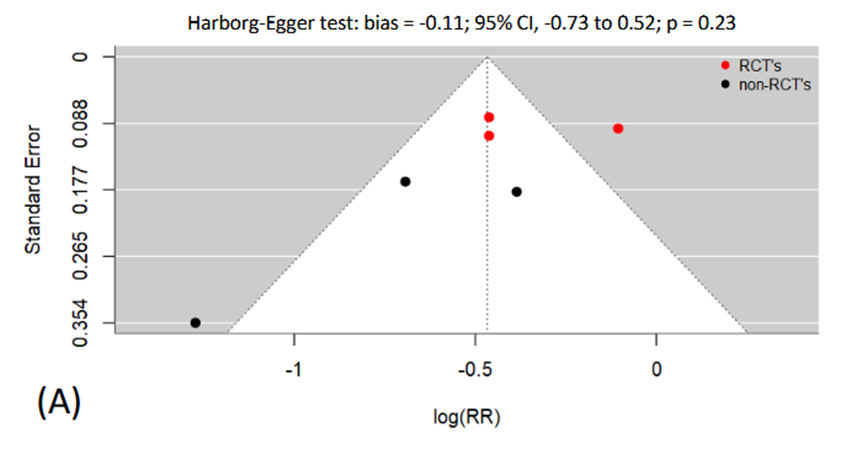
Two reviewers (O.G. and J.S.) independently extracted data with regard to trial characteristics, potential bias and pre-specified outcomes. Any disagreements were solved by consensus. The study quality assessment comprised the risk of study bias, publication bias and the overall strength of evidence. The risk of study bias was assessed at the methodological and outcome level using Cochrane’s risk of bias 2 (RoB2) tool [15]. Publication bias was evaluated using funnel plots [16] and the Harbord-Egger test for asymmetry [17]. Since Harbord-Egger test is unreliable for analysis of publication bias using fewer than ten studies, the Trim-and-Fill-Method was used to detect and, if necessary, impute any missing studies [18]. Finally, the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) method was employed to evaluate overall quality of evidence (for RCT’s only) with regard to study limitations, consistency and directness [19].
Data synthesis and statistical analysis
Meta-analysis was conducted using Cochrane’s Review Manager (RevMan) Version 8.17.0 (The Cochrane Collaboration, London, United Kingdom) (https://revman.cochrane.org/info). Heterogeneity of trial results was assessed with Cochrane’s Q and I2 statistic [20] using the DerSimonian and Laird method. Statistical analysis of publication bias was performed with R version 4.1.2 (The R Foundation for Statistical Computing, http://www.R-project.org). We performed a meta-analysis of relative risks (RR) with 95% confidence intervals (CI) using the Mantel-Haenszel method and a random-effects model for analysis of prespecified outcomes. Numbers needed to treat (NNT) were calculated from absolute risk reductions. All statistical tests were two-sided, and p-values less than 0.05 were considered as statistically significant, except less than 0.10 for heterogeneity analyses, as recommended. For all primary endpoints we sequentially excluded each trial from the meta-analysis to assess its specific effect on the pooled relative risk in sensitivity analyses.
Regulatory aspects
Only outcome data from previously published trials was extracted and no active patient recruitment was performed. Therefore, no formal approval from the local institutional review board was necessary. In addition, all trials involved in the meta-analysis reported approval by their respective ethical regulatory authorities and having obtained written informed consent from each patient. Our analysis complied with the Declaration of Helsinki, and the results were presented according to the PRISMA statement on systematic reviews and meta-analyses [21]. This study did not receive any direct funding.
Literature search
The literature search covered five online databases and four current guidelines were searched manually. After removing duplicates, 1,332 records were screened for eligibility and out of these, 23 studies were considered for full-text evaluation. Fourteen articles were then excluded because (i) the article was a substudy (n = 4), (ii) the article was a conference record (n = 3), (iii) all-cause mortality was not reported (n = 2), (iv) the article did not compare TEER and GDMT (n = 2), (v) the etiology of MR was primary in more than 30% of cases (n = 1), (vi) the article considered the outcomes after repeat MitraClip intervention (n = 1), (vii) there was a population overlap with another included study (n = 1). Out of the remaining nine full-text articles, three RCT’s [11, 12, 13] were included in the main meta-analysis. Additionally, six non-randomized studies [22, 23, 24, 25, 26, 27] were included for the extended meta-analysis. Figure 1 shows the study flow diagram.
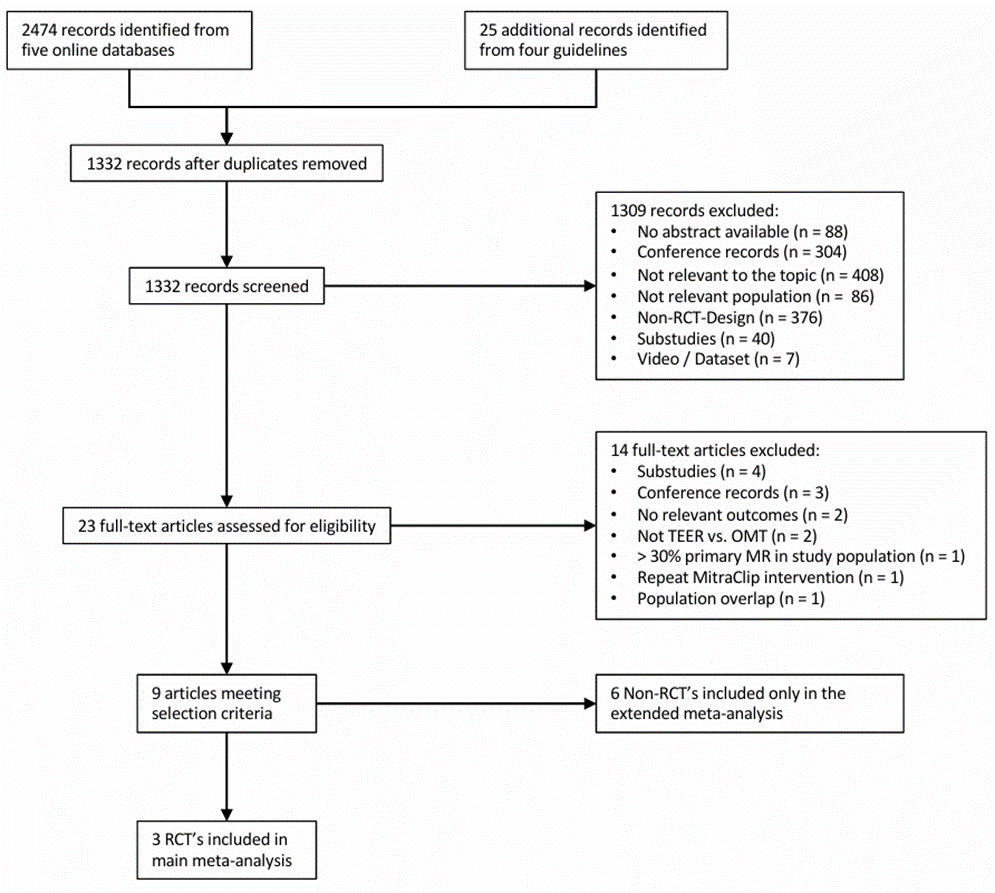
Figure 1: Study flow diagram.
Study characteristics
Table 1 and 2 provide an overview of important characteristics of included studies. The three RCT’s included a total of 1,423 patients. A total of 704 patients were assigned to the TEER group and 719 patients were assigned to the GDMT group. In the TEER group all patients were treated with the MitraClipTM device on top of GDMT. In the control group, all patients were treated with GDMT in accordance with the current European or American practice guidelines at the time of the trial. All RCT’s were multicentric and patients were followed for at least 24 months for the primary endpoints (weighted mean 20 ± 9 months). The inclusion criteria were comparable between the three trials. There were minor differences with regard to MR severity, and LVEDV among the three RCT’s (Table 1) [28].
The six non-RCT’s included a total of 1,382 patients of which 778 were assigned to TEER and 604 to GDMT. Four of them used propensity score matching to reduce inherent selection bias. Mean age and follow-up duration were comparable between RCT's and non-RCT’s.
| Trial | Year of Publication | Setting | Sample size (n) | Mean age (yrs) | Mean follow-up (months) | Primary effectiveness endpoints | LVEF (%) | LVEDV (mL) | EROA (mm2) | RegV (ml/beat) |
| COAPT [11] | 2018 | 78 sites in the United States and Canada | 614 | 72 | 20 | (i) HF hospitalization | 31 | 193 | 41 | N/A |
| MITRA-FR [13] | 2019 | 37 sites in France | 304 | 70 | 24 | (i) all-cause mortality or unplanned HF hospitalization | 33 | 252 | 31 | 45 |
| RESHAPE-HF2 [12] | 2024 | 30 sites in Europe | 505 | 70 | 19 | (i) first or recurrent HF hospitalization and CV death, (ii) first or recurrent HF hospitalization, (iii) change in KCCQ score | 31 | 205 | 23 | 36 |
Abbreviations: HF denotes heart failure; CV, cardiovascular; KCCQ, Kansas City Cardiomyopathy questionnaire; LVEF, left ventricular ejection fraction; LVEDV, left ventricular end-diastolic volume; MR, mitral regurgitation; EROA, effective regurgitant orifice area; RV, regurgitant volume. LVEF, LVEDV, EROA and RegV are given as mean or median as determined in the original publication. | ||||||||||
Table 1: Study characteristics of included RCT’s
| Trial | Year of Publication | Setting | Sample size (n) | Mean age (yrs) | Follow up (months) | Primary effectiveness endpoints | LVEF (%) |
| Armeni et al. [13] | 2016 | GDMT group: ANMCO registry, TEER group: two institutional databases, propensity score adjusted analysis | 383 | 71 | 12 | (i) life expectancy | 33 |
| Asgar et al. [23] | 2017 | GDMT group: single-centre retrospective cohort, TEER group: single-centre prospective cohort, propensity score adjusted analysis | 92 | 72 | 12 | (i) all-cause mortality | 35 |
| Giannini et al. [24] | 2016 | Single-centre prospective cohort, propensity score adjusted analysis | 120 | 75 | 36 | (i) overall survival, (ii) CV death, (iii) HF hospitalization | 34 |
| Jonik et al. [25] | 2024 | Single-centre retrospective cohort | 185 | 71 | 29 | (i) CV death | 30 |
| Swaans et al. [26] | 2014 | GDMT group: retrospective cohort, TEER group: prospective cohort | 251 | 73 | 36 | (i) overall survival | 36 |
| Velazquez et al. [27] | 2015 | GDMT group: Duke high-risk cohort, TEER group: EVEREST II HRR and REALISM registries, propensity score adjusted analysis | 478 | 70 | 12 | (i) overall survival | 42 |
| Abbreviations: GDMT denotes guideline-directed medical therapy; TEER, transcatheter edge-to-edge repair; HF, heart failure; CV, cardiovascular; LVEF, left ventricular ejection fraction; LVEDV, left ventricular end-diastolic volume; MR, mitral regurgitation; EROA, effective regurgitant orifice area; RV, residual volume. | |||||||
Table 2: Study characteristics of included non-RCT’s
Study quality and risk of bias
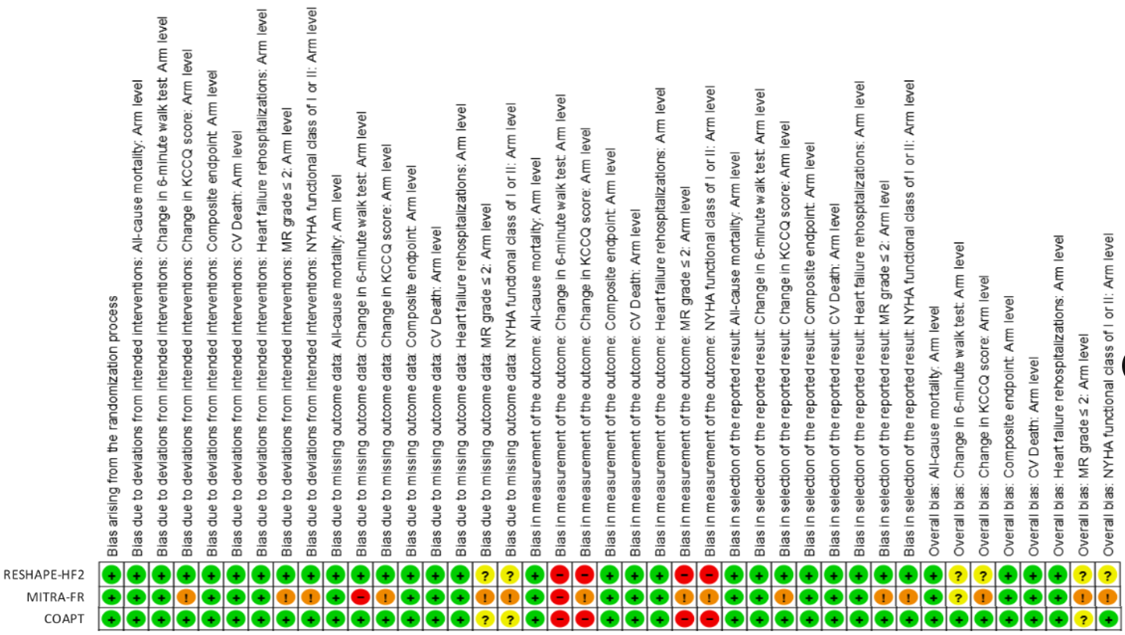
Globally, the three RCT’s had low risk of bias when assessed with Cochrane’s Risk of Bias 2 (RoB2) tool (Table 3) [15]. A more extensive risk of bias assessment based on individual endpoints (including secondary endpoints) is given in Supplementary Figure 1. Global assessment indicated some concerns regarding measurement of outcomes, which was mainly due to the lack of blinding of study participants and personnel. However, it is unlikely that the primary efficacy and safety outcomes were influenced by this bias. Some secondary outcomes (i.e. KCCQ score, NYHA functional class and 6MWT) may have been influenced through knowledge of treatment assignment. Only the COAPT trial blinded study personnel for assessment of these outcomes [11]. Attrition rates were inconsistent throughout all RCT’s but handled well in the statistical analysis. Visual inspection of funnel plots (Supplementary Figure 2) did not indicate any significant publication bias, and Harborg-Egger tests did not show any statistical asymmetry. Trim-and-Fill-Method estimated no missing studies for the outcome HF hospitalizations. For all-cause mortality, the Trim-and-Fill-Method estimated two missing studies and for the outcome CV death one missing study was estimated. Overall, this results in a low to moderate risk of publication bias. Supplementary Table 1 provides an overview of the quality of evidence evaluation using the GRADE method. All included outcomes can be considered direct. Consistency of results with regard to direction and magnitude of effect was limited for most outcomes. This was mainly driven by heterogeneity of the results, which was at least moderate for most outcomes (except change in KCCQ score and NYHA class). The individual trials lacked precision, due to broad confidence intervals, but performing a meta-analysis produced more precise results. Thus, we rated the strength of evidence as moderate at least, according to the updated GRADE method.
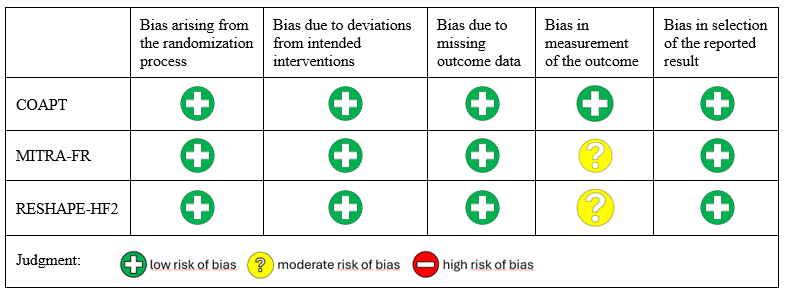
Table 3: Risk of bias summary for the three RCT’s based on the Cochrane’s Risk of Bias 2 (RoB2) tool [15]
Primary endpoints
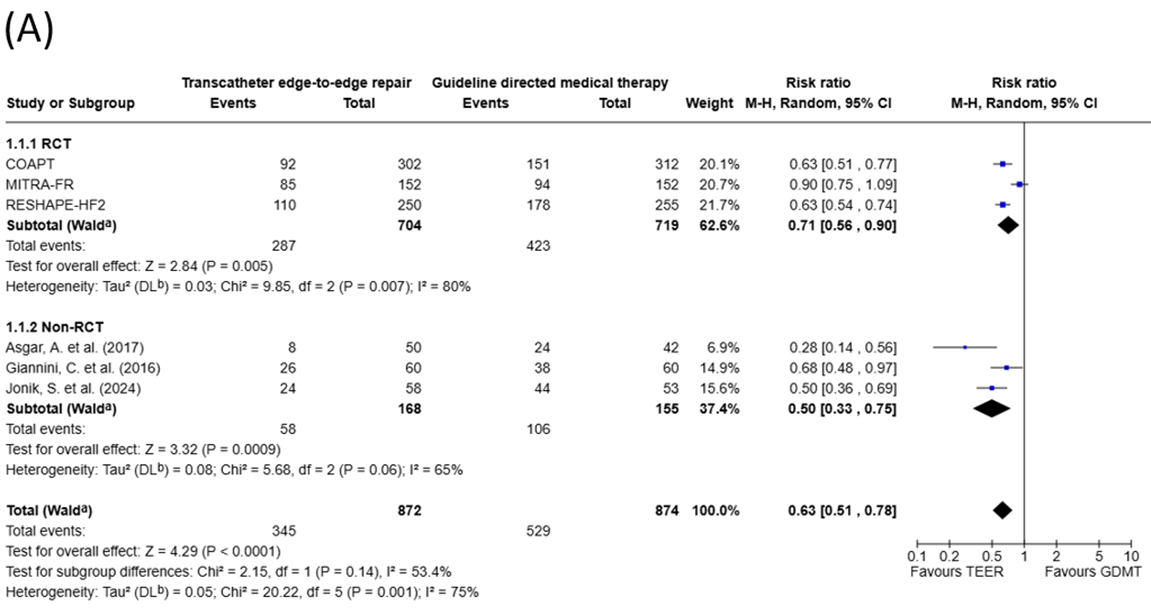
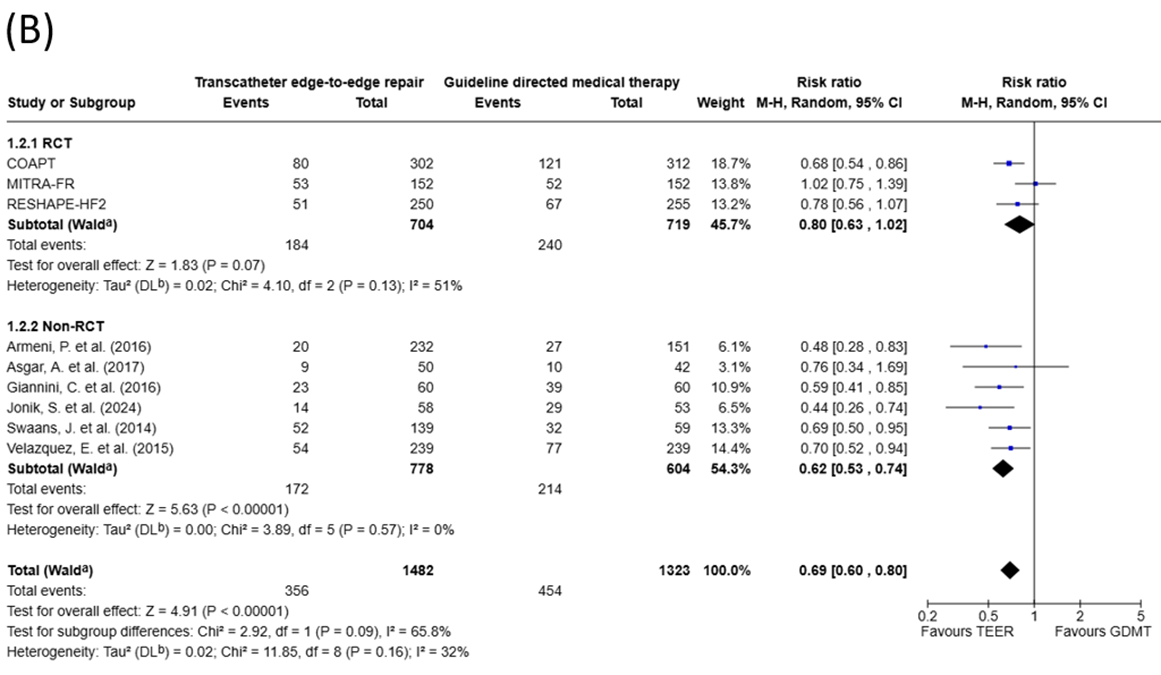
Primary endpoints (HF hospitalizations, all-cause mortality and CV death) could be extracted from all three RCT’s including a total of 1,423 patients (Figure 2). Meta-analysis revealed a 29% relative risk reduction for new or recurrent HF hospitalizations (RR 0.71; 95% CI, 0.56 to 0.90; p = 0.005; NNT = 6) for TEER compared to GDMT. Moreover, there were nonsignificant trends towards reduced all-cause death (RR 0.80; 95% CI, 0.63 to 1.02, p = 0.07; NNT = 14) and CV death (RR 0.81; 95% CI, 0.62 to 1.06; p = 0.12; NNT = 19). Heterogeneity across RCT’s was substantial for the endpoint HF hospitalizations (Q = 9.85; p = 0.007; I2 = 80%), and moderate for all-cause and CV death (Q = 4.10; p = 0.13; I2 = 51%, and Q = 3.86; p = 0.15; I2 = 48%, respectively). In the non-RCT’s, two of the endpoints (HF hospitalizations and CV death) were not available in all studies (Figure 2). When non-RCT’s were included in the meta-analysis, the treatment effect was increased for all three primary endpoints, and reductions in all-cause and CV death were rendered significant.
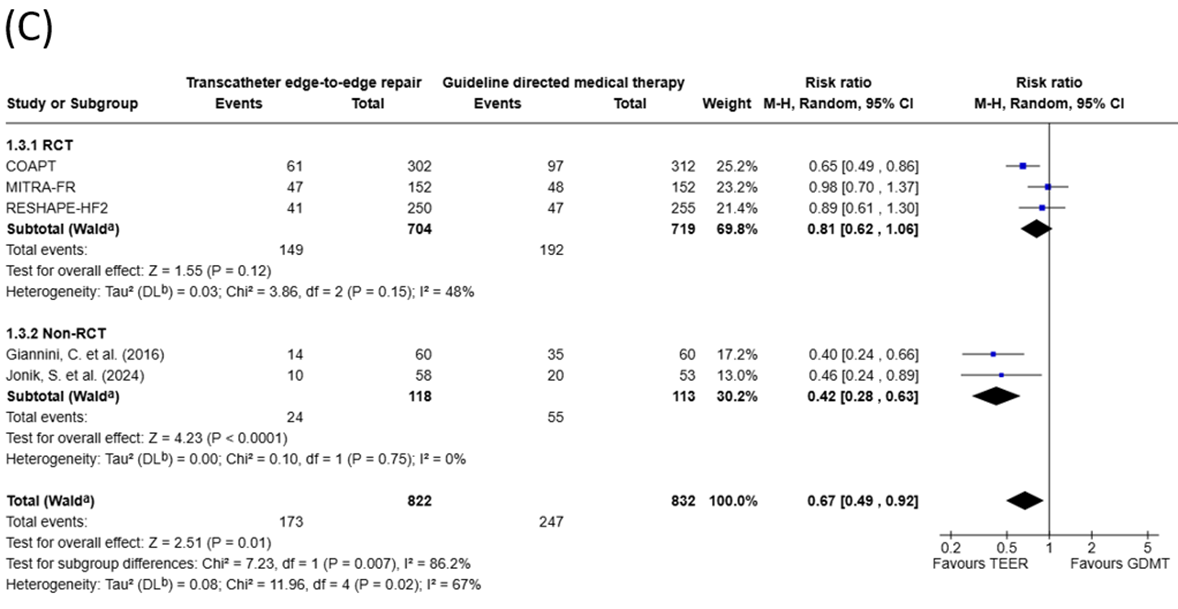
Abbreviations: RCT denotes randomized controlled trial; TEER, transcatheter edge-to-edge repair; GDMT, guideline-directed medical therapy.
Figure 2: Results from meta-analyses presented as Forest plots for the primary endpoints (A) heart failure hospitalizations, (B) all-cause death, and (C) cardiovascular death.
Secondary endpoints
For the analysis of the secondary outcomes only data from RCT’s was available (Figure 3). Changes in 6MWD favoured TEER by 38 m on average compared to GDMT (mean difference 38 m; 95% CI, 14 m to 63 m; p = 0.002). Similarly, quality-of-life as measured by KCCQ score improved significantly more after TEER (mean difference 15 points; 95% CI, 11 to 18; p less than 0.001) and MR grade ≤ 2 at 12 months (RR 2.20; 95% CI, 1.79 to 2.71; p less than 0.001).
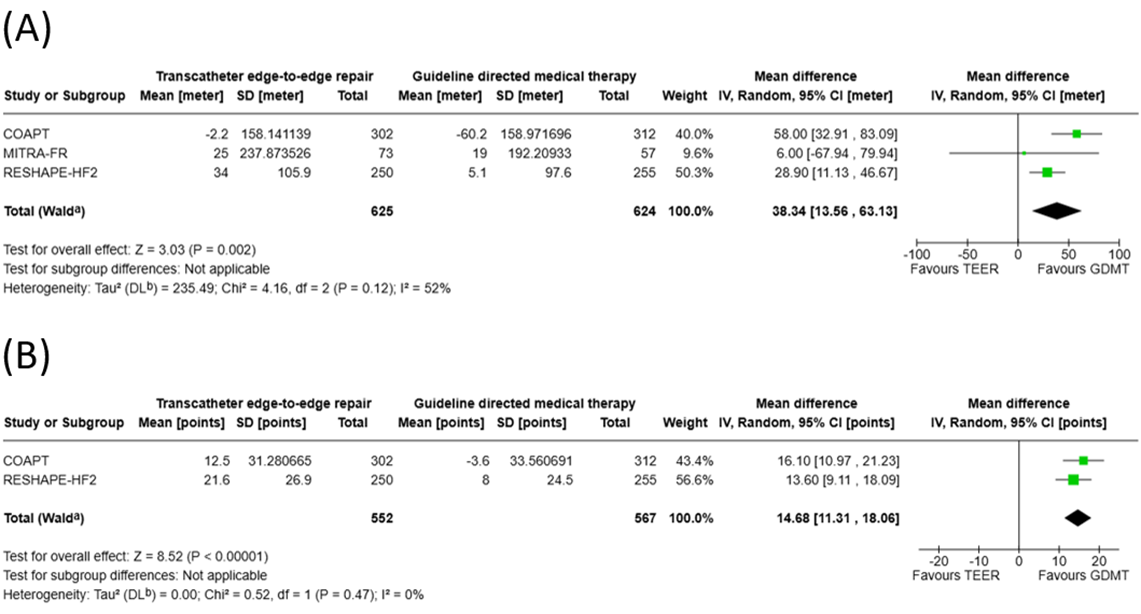
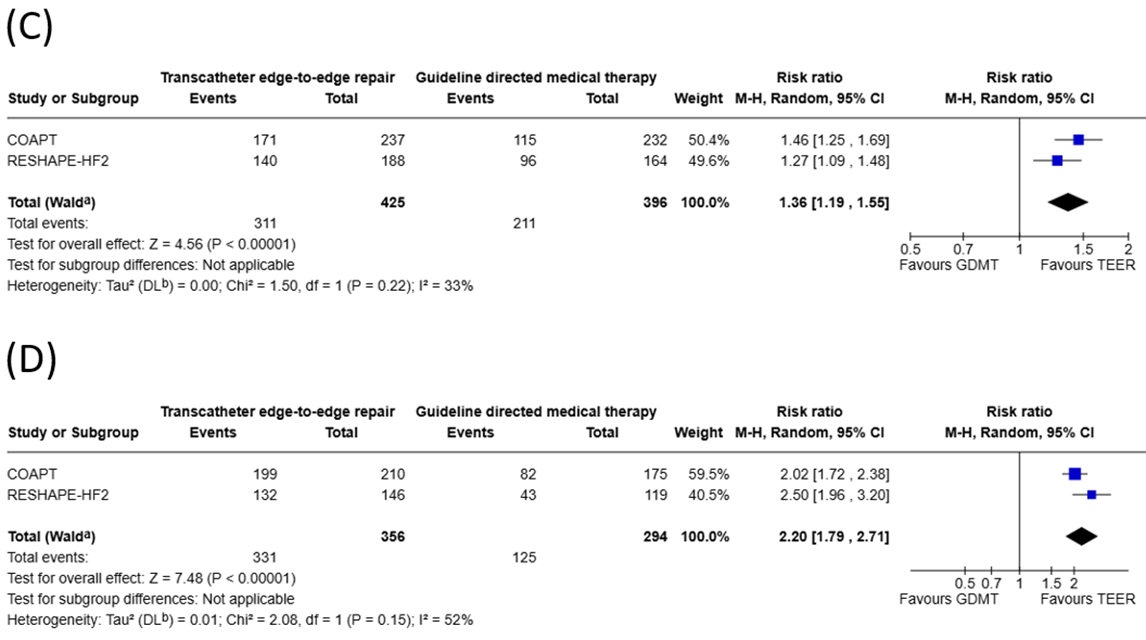
Abbreviations: RCT denotes randomized controlled trial; TEER, transcatheter edge-to-edge repair; GDMT, guideline-directed medical therapy.
Figure 3: Results from meta-analyses presented as Forest plots for the secondary endpoints (A) change in 6-min walking distance, (B) change in Kansas City Cardiomyopathy Questionnaire (KCCQ) overall score, (C) Patients in New York Heart Association (NYHA) class I and II, and (D) Patients with mitral regurgitation (MR) severity 1+ and 2+.
Sensitivity analysis
For the endpoint of HF hospitalizations, excluding either RESHAPE-HF2 [12] or COAPT [11] from the meta-analysis of RCT's rendered the pooled RR statistically non-significant. Exclusion of MITRA-FR [13] led to the result changing in favour of TEER (RR 0.63; 95% CI, 0.55 to 0.72, p less than 0.001). Regarding all-cause death, exclusion of MITRA-FR [13] rendered the pooled RR significant in favour of TEER (RR 0.71; 95% CI, 0.59 to 0.86; p less than 0.001) while exclusion of RESHAPE-HF2 [12] and COAPT [11] did not change the result significantly. Regarding CV death, sequentially excluding each of the three RCT’s did not change the result significantly. In the expanded meta-analysis (including both RCT’s and non-RCT’s) only the exclusion of COAPT [11], Giannini et al. [24] and Jonik et al. [25] led to a change in significance for the endpoint of CV death.
The main objective of the present report was to perform a systematic review and meta-analysis of published RCT’s comparing TEER versus GDMT in patients with HFrEF and SMR. The RCT meta-analysis was further expanded by adding published non-randomized studies, while being well aware of the inherent biases and lower quality of the latter. Overall, we included 1,423 patients from three RCT’s and 1,382 patients from six non-RCT’s. The results of the meta-analysis can be summarized as follows: In HFrEF patients with SMR, TEER results in (i) a significant 29% reduction of new or recurrent HF hospitalizations compared to GDMT alone at approximately 2 years (weighted mean = 20 ± 9 months) of follow-up. (ii) All-cause and CV death did not change significantly, although there were numerical trends in favour of TEER (non-significant reductions by 20% and 19%, respectively). (iii) TEER was associated with significant improvements in 6MWD, quality-of-life (as assessed by the KCCQ score), better functional capacity by NYHA class, and significantly less MR burden. The results of the present study are in line with a previous meta-analysis published as a brief communication by Anker and colleagues [29]. Our data not only confirms previous reports, but also expands and strengthens the results by a systematic analysis of study biases and strength/quality of evidence (as recommended by PRISMA [21]), adding patient-reported outcome measures (PROM’s) (e.g. KCCQ score) rather than only clinical endpoints, and including evidence from non-randomized trials.
Recurrent HF hospitalizations are an important concern in HFrEF patients and are associated with CV mortality and health-care costs. Approximately, 60-70% of total health-care expenditures for HF are driven by HF hospitalizations [30]. Hence, the significant 29% reduction with TEER observed in our meta-analysis is clinically relevant, contributes to lower disease burden, and may result in significant cost savings for HFrEF patients. In absolute terms, treating six patients with TEER can prevent one HF hospitalization over the ensuing 2 years. The reduction appears plausible, is in line with previous observations in non-randomized studies [9], and is further substantiated by adding non-RCT’s in the extended meta-analysis (Figure 2). However, a considerable heterogeneity should be highlighted (Q = 9.85; p = 0.007; I2 = 80% for the three RCT’s included), with MITRA-FR appearing as the outlier in the sensitivity analyses. Indeed, there were important differences in baseline characteristics that may explain these findings: Patients included in MITRA-FR had larger LV volumes compared to the two other RCT’s (Table 1). On the other hand, inclusion criteria for MR severity differed between the three RCT’s: MITRA-FR enrolled patients on the basis of the 2012 ESC/EACTS guidelines on the management of valvular heart disease [31], which defined severe SMR at an effective regurgitant orifice area of 20 mm2 (regurgitant volume at 30 mL/beat), while COAPT and RESHAPE-HF2 used more stringent criteria [32, 33]. As a result, MITRA-FR enrolled patients with limited MR severity as opposed to rather dilated LV’s, particularly when compared to COAPT. This apparent disparity between LV dimensions and MR severity and its implications for treatment success after TEER has been addressed by Grayburn and colleagues, and has led to the term of “proportionate” versus “disproportionate” SMR, which may explain some of the heterogeneity observed between RCT’s for the primary endpoints [28].
The numerical reductions observed in all-cause (20%) and CV death (19%) (Figure 2) with TEER fell short of statistical significance in our meta-analysis. However, heterogeneity across trials was less than for the endpoint “HF hospitalizations” (Q = 4.10; p = 0.13; I2 = 51%, and Q = 3.86; p = 0.15; I2 = 48%, respectively), and the margin of the 95% CI overlapping the line of identity was small. When adding the results from non-RCT’s in the expanded meta-analysis, the reductions in all-cause and CV mortality were rendered significant (31% and 33%, respectively; p less than 0.001). Nonetheless, non-RCT’s are inherently biased and degrade the overall quality of the meta-analysis, and therefore our results currently allow no firm conclusion on the effect of TEER over GDMT on all-cause and CV mortality. However, the observed lack of significance may still be attributed to a statistical type II error based on the limited sample size in the RCT’s, and further randomized trials are needed to draw a definitive conclusion. The observed trends for reduced all-cause and CV death were very similar in magnitude indicating that any potential mortality benefit would be driven primarily by CV mortality. Moreover, it documents the high safety profile of the TEER procedure with no signal for increased overall or non-CV mortality.
TEER was associated with improved functional capacity and quality-of-life compared to GDMT alone (Figure 3): Changes in 6MWD favoured TEER, the average increment in 6MWD was 38 m larger with TEER compared to GDMT alone (p = 0.002). Similarly, more patients were in NYHA class I or II after TEER compared to GDMT (RR 1.36; p less than 0.001). Quality of life as measured by KCCQ score improved significantly more after TEER (mean difference 15 points; 95% CI, 11 to 18; p less than 0.001). Although, this result is only based on two RCT’s (COAPT and RESHAPE-HF2), its magnitude should be pointed out (moderate to large increase in quality-of-life) [34]. When put into perspective, a KCCQ increase by 15 points over background therapy exceeds observed benefits of angiotensin receptor-neprilysin inhibitors (+1 point) [35], sodium-glucose cotransporter 2 inhibitors (+6 points) [36], and cardiac resynchronization therapy (+10 points) [37]. The MITRA-FR study employed the European Quality of Life 5-Dimensions (EQ5D) visual analogue scale and results were incomplete. EQ5D increased by 9 points in the TEER group (4 points more than in the GDMT group) [10], a result that can be considered a small to moderate improvement in quality-of-life [34] and is in line with the results of the two other RCT’s.
There are a number of limitations of our meta-analysis that should be mentioned. First, we conducted a study-level meta-analysis while a patient-level pooled analysis might have provided better evidence. Additionally, the study-level design precluded assessing specific subgroups for their respective benefits of TEER versus GDMT. Second, the sample size included in the three RCT’s is still limited. A potential type II error for some of the primary endpoints cannot be excluded. Third, the lack of blinding of patients and personnel to the type of treatment may be perceived as a limitation of the RCT’s included in the meta-analysis. However, currently, to our knowledge, no randomized sham-controlled trials of TEER versus GDMT are available. And finally, we expanded our meta-analysis by adding six non-randomized trials. Non-RCT’s are inherently flawed by selection bias, hence the results of the expanded meta-analyses should be considered with caution.
In HFrEF patients with SMR, our meta-analysis showed that TEER results in a significant reduction of future HF hospitalizations, and non-significant trends towards lower all-cause and CV mortality compared to GDMT. Furthermore, we showed that TEER was associated with significant improvement in patient-centered outcomes (6MWD, NYHA functional class, and quality-of-life).
This study did not receive any funding. None of the authors report any potential conflict of interest related to this manuscript.
Supplementary Material
Supplementary Figure 1: Detailed risk of bias assessment for individual endpoints in the three RCT’s based on the Cochrane’s Risk of Bias 2 (RoB2) tool [15].
Supplementary Figure 2: Funnel plots and Harborg-Egger tests for the three primary endpoints of HF hospitalizations (A), all-cause death (B) and cardiovascular death (C)
Supplementary Table 1: Assessment of overall quality of evidence of included RCT’s with the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) method [19].
| Quality assessment | Summary of findings | ||||||||||
| No of patients | Effect | ||||||||||
| Outcome (No of studies) | Design | Quality | Consistency | Directness | Other modifying factors | TEER | GDMT | Relative [95% CI] | Absolute | Quality | Importance |
| HF rehospitalization (3) | RCT’s | No serious limitations in study methods, low risk of bias | No serious differences in PICO; CI not overlapping on visual inspection of forest plot; Q = 9.85; p = 0.007; I2 = 80% | Direct | None | 704 | 719 | RR 0.71 [0.56 to 0.90] | ARR 18.06%, NNT = 6 | Moderate | Critical |
| All-cause mortality (3) | RCT’s | No serious limitations in study methods, low risk of bias | No serious differences in PICO; overlapping CI on visual inspection of forest plot; Q = 4.10; p = 0.13; I2 = 51% | Direct | CI does not rule out the possibility of no effect | 704 | 719 | RR 0.80 [0.63 to 1.02] | ARR 7.24% NNT = 14 | Moderate | Critical |
| CV death (3) | RCT’s | No serious limitations in study methods, low risk of bias | No serious differences in PICO; overlapping CI on visual inspection of forest plot; Q = 3.86; p = 0.15; I2 = 48% | Direct | CI does not rule out the possibility of no effect | 704 | 719 | RR 0.81 [0.62 to 1.06] | ARR 5.54%, NNT = 19 | Moderate | Critical |
| Change in 6MWD (3) | RCT’s | No serious limitations in study methods, concerns about measurement of the outcome | No serious differences in PICO; overlapping CI on visual inspection of forest plot; Q = 4.16; p = 0.12; I2 = 52% | Direct | Imprecise data | 625 | 624 | MD 38.34 [13.56 to 63.13] | N/A | Moderate | Important |
| Change in KCCQ (2) | RCT’s | No serious limitations in study methods, concerns about measurement of the outcome | No important inconsistencies: no serious differences in PICO; overlapping CI on visual inspection of forest plot; Q = 0.52; p = 0.47; I2 = 0% | Direct | None | 552 | 567 | MD 14.68 [11.31 to 18.06] | N/A | Moderate to High | Important |
| NYHA functional class of I or II (2) | RCT’s | No serious limitations in study methods, concerns about measurement of the outcome | No important inconsistencies: no serious differences in PICO; overlapping CI on visual inspection of forest plot; Q = 1.50; p = 0.22; I2 = 33% | Direct | None | 425 | 396 | RR 1.36 [1.19 to 1.55] | ARR -19.89%, NNT = 6 | Moderate to High | Important |
| MR grade ≤ 2 (2) | RCT’s | No serious limitations in study methods, concerns about measurement of the outcome | No serious differences in PICO; overlapping CI on visual inspection of forest plot; Q = 2.08; p = 0.15; I2 = 52% | Direct | Strong association | 356 | 294 | RR 2.20 [1.79 to 2.71] | ARR -50.46%, NNT = 2 | High | Important |
Abbreviations: No denotes number; TEER, transcatheter edge-to-edge repair; GDMT, guideline-directed medical therapy; CI, confidence interval; RCT, randomized controlled trial; PICO, patient/intervention/comparator/outcome; RR, relative risk; ARR, absolute risk reduction; NNT, number needed to treat; HF, heart failure; CV, cardiovascular; 6MWD, 6-minute walk distance; MD, mean difference; KCCQ, Kansas City Cardiomyopathy Questionnaire; NYHA, New York Heart Association; MR, mitral regurgitation.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
