
Research Article | DOI: https://doi.org/10.31579/2768-2757/140
1Senior Resident, Indira Gandhi medical college1, Shimla, India.
2Senior Resident, Department of Orthopaedics, PGIMER2, Chandigarh, India.
*Corresponding Author: Vivek P Ksheerasagar., Senior Resident, Indira Gandhi medical college1, Shimla, India.
Citation: Bhushan B., Sharma A., Vivek P. Ksheerasagar., Teja T., Akash K. Ghosh, et al, (2024), Comparison of short segment posterior spinal fixation with or without index screw in thoracolumbar spinal injuries – mid-term results, Journal of Clinical Surgery and Research, 5(7); DOI:10.31579/2768-2757/140
Copyright: © 2024, Vivek P Ksheerasagar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 August 2024 | Accepted: 16 September 2024 | Published: 16 October 2024
Keywords: thoracolumbar spinal injuries; posterior fixation; index screw fixation
Introduction: Short-segment spinal instrumentation has been advantageous in the treatment of thoracolumbar spinal fractures for better correction of kyphotic deformity. Many authors considered that together with the rods with lordotic contour, pedicle screw fixation at the fractured vertebra can cause a forward driving force to augment the reduction, and help to directly elevate the end plate to assist in the restoration of the compressed vertebral height. So it is worthwhile to study the functional and radiological outcome of short-segment fixation of thoracolumbar spine fracture with or without an index screw.
Material and methods: A total of 108 patients (44 retrospective and 64 prospective) underwent posterior stabilisation with pedicle screws and rod construct under radiographic guidance. The only difference in the two groups is the insertion of an index screw in the fractured vertebra. Neurological and functional outcomes of all patients were analysed with the ASIA scale, Denis pain score and Denis work scale preoperatively, postoperatively and at 9 months. Radiographic assessment was done with a preoperative radiograph and CT scan measuring regional kyphotic angle at preoperative, postoperative and final follow-up.
Results: Of the total 108 patients with dorsolumbar vertebral fracture- Group-A had 28 patients without index screws, Group-B had 80 patients with index screw in the fractured vertebra. Postoperatively, we found neurological improvement by 1 grade according to the ASIA scale but there was no significant difference between the two groups. We found no significant difference in the neurological and functional outcomes but the change in kyphotic angle between the immediate postoperative period and 9 months follow-up was significantly less in group B.
Conclusion: The addition of an index screw in the thoracolumbar fractures will help in better kyphosis correction, less correction loss in kyphotic angle in the postoperative period with fewer instrument failures, without additional complications.
With increasing roadside accidents, falls and industrialization spine injuries are increasing day by day, usually associated with high-energy trauma. Dorsolumbar spinal injuries account for 30-50% of all spine injuries [1]. Dorsolumbar injuries in trauma are seen at the dorsolumbar junction, with 60% occurring between T11 and L2 vertebral level, and 10-14% involving the lower lumbar spine. Around 20% of patients with fractures at thoracolumbar level have neurological injuries [2]. The susceptibility of the thoracolumbar junction is mainly due to there is transition from more rigid kyphosis of the thoracic region to mobile lordosis lumbar region [3]. This zone of transition is susceptible to substantial biomechanical stress during traumatic incidents, making it more vulnerable to fracture. It is a grave injury that can cause significant morbidity and disability to the patient. The goal of surgery in these fractures includes decompression of the neural components, reduction of fracture, providing a rigid fixation, and rehabilitation of the patient. If surgical treatment of thoracolumbar spine fracture is decided further debate arises on the type of approach [4]. Anterior decompression with stabilization has been suggested for cases with severe spinal canal narrowing, severe comminution or dislocation, and neurological deficit. However, the posterior approach is less extensive, and many surgeons advocate short-segment spinal instrumentation. Recent literature shows that circumferential decompression with stabilization of the fracture can be done through the posterior approach alone with good results thereby reducing the surgical time, blood loss, infection, overall morbidity and complications seen with the anterior and combined approach. Short-segment spinal instrumentation has been advantageous in the treatment of thoracolumbar spinal fractures for better correction of kyphotic deformity with greater initial stability, early painfree mobilisation, and indirect decompression of the spinal canal. Many authors considered that together with the rods with lordotic contour, pedicle screw fixation at the fractured vertebra can cause a forward driving force to augment the reduction and reshaping. Also, the screw put at the fractured vertebra can be used to directly elevate the end plate to assist in the restoration of the compressed vertebral height. A screw inserted at the fractured vertebrae can reduce the stress of screws in the upper and lower normal vertebrae to decrease the incidence of fracture of screws [5]. Surgeons who advocate these implants for dorsolumbar instability after a burst fracture suggest augmentation with anterior column support to avoid excessive cantilever loads on the screws that might lead to bending failure or breakage. So, it is worthwhile to study the functional and radiological outcome of short segment fixation of thoracolumbar spine fracture with or without one screw fixation in fracture vertebrae. Hence this study is designed to evaluate the result after short segment fixation one level above and one level below and one screw in fracture vertebrae (index screw) and to compare to fixation one level above and one below.
To compare the radiological and clinical outcome of short segment posterior spine stabilisation for thoracolumbar injuries with or without index screw.
A total of 108 patients (44 retrospective and 64 prospective) operated at the Department of Orthopaedics at Indira Gandhi Medical College, Shimla were included in the study. Clearance from the ethics committe was taken from the institutional ethical review committee and informed consent was taken from the patients.
Inclusion criteria
Exclusion criteria
The patients included in the study were thoroughly evaluated on admission and were taken up for posterior stabilisation of the thoracolumbar injury in a prone position using a midline open approach with pedicle screws and rod construct under radiographic guidance. The only difference in the two groups is the insertion of an index screw in the fractured vertebra. Laminectomy is done in cases where canal diameter is decreased by more than one-third and the patient has a neural deficit. Sometimes dural tear was found due to the bony fragment injuries. The dural tear was repaired with 3-0 silk with continuous stitches. Thorough toileting of the wound is followed by meticulous closure in layers over a suction drain. All patients were mobilised as soon as possible based on their neurological condition. Neurological and functional outcomes of all patients were analysed with the ASIA scale (American Spine Injury Association impairment scale), Denis pain score and Denis work scale at the time of admission (preoperatively), postoperatively and at 9 months. Radiographic assessment for all patients with a preoperative radiograph and CT scan in the supine position measuring- Regional kyphotic angle at preoperative, postoperative and final follow-up. Figure 1 and 2 show postoperative xrays of patients with and without index screw.
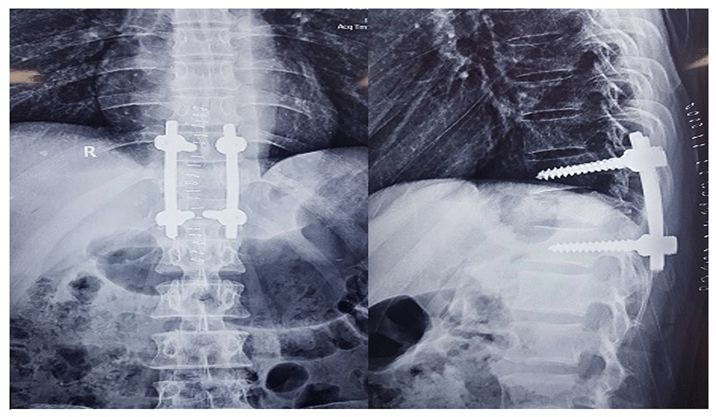
Figure 1: Postoperative X-ray showing screws in AP and lateral view shows without screw at fracture vertebrae.
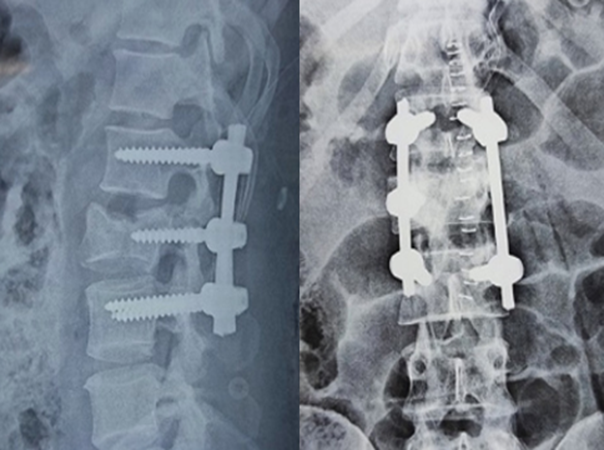
Figure 2: Postoperative X- rays AP and Lateral view with index screw.
Of the total 108 patients- Group-A had 28 patients (10 prospective, 18 retrospective) without index screws in the fractured vertebra, Group-B had 80 patients (54 prospective, 26 retrospective) with index screw in the fractured vertebra. All the demographic details are summarised in Table and no significant difference was found between the 2 groups. Injury characteristics are summarised in Table- our majority of patients had fracture at dorsolumbar junction and no significant difference in the type of fracture or the neurological involvement but Group-B had a significantly low pre-operative kyphotic angle.
| Demographic variable | Group-A (with index screw) | Group-B (without index screw) | P value |
| Age (years)- mean± SD (range) | 48.14±4.35 (26-78) | 44.88±12.89 (18-65) | 0.32 |
| Gender- male/ female (%) | 19/9 (67.8/32.2) | 38/42 (47.5/52.5) | 0.063 |
| Mode of injury- Fall/ Road traffic accident (%) | 27/1 (96.4/3.6) | 66/14 (82.5/17.5) | 0.18 |
| Interval between admission and surgery- <5days>5days | 17/11 (60.7/39.3) | 58/22 (72.5/27.5) | 0.507 |
Table 1: Demographic details of patient population.
| Injury characteristic | Group-A (with index screw) | Group-B (without index screw) | P value |
| Fracture vertebra level- Dorsal(D3-D8) Dorsolumbar(D9-L2), Lumbar(L3-L5) | 11/15/2 (39.3%/53.6%/7.1%) | 7/60/13 (8.8%/75%/16.2%) | <0> |
| AO classification- A/B/C | 28/0/0 (100%/0/0) | 77/2/1 (96.25%/2.5%/1.25%) | 0.77 |
| Kyphotic angle | 29.39±6.84 | 21.8±5.52 | <0> |
| TLICS score* | 5.04±0.51 | 5.26±0.71 | 0.122 |
| ASIA score- A/B/C/D/E | 1/2/5/17/3 | 0/4/11/58/7 | 0.439 |
Table 2: Preoperative injury characteristics of the patient population.
*Thoraco-Lumbar Injury Classification and Severity score.
Postoperatively, we found neurological improvement by 1 grade according to the ASIA scale but there was no significant difference between the two groups and significant improvement in kyphotic angle compared to preoperative value. These findings are summarised in Table 3.
| Postoperative variable | Group-A (with index screw) | Group-B (without index screw) | P value |
| Kyphotic angle | 23.57±6.95 | 16.41±5.21 | <0> |
| Change between preop-post op kyphotic angle | 5.82±1.82 | 5.38±2.39 | 0.23 |
| ASIA score- A/B/C/D/E | 0/2/1/6/19 | 0/2/4/35/39 | 0.518 |
Table 3: Postoperative radiological and neurological outcomes.
Radiological and functional outcomes at 9 months follow-up are summarised in Table-4.
| Variable | Group-A (with index screw) | Group-B (without index screw) | P value |
| Kyphotic angle | 25.39±7.05 | 16.86±5.27 | <0> |
| Change between preop & final follow-up kyphotic angle | 4.0±1.61 | 4.93±2.71 | 0.12 |
| Change between post op & final follow-up kyphotic angle | 1.82±1.70 | 0.45±1.90 | <0> |
| ASIA score- A/B/C/D/E | 0/1/1/4/22 | 0/2/3/8/67 | 0.919 |
| Complications- Yes**/No | 26/2 (92.8/7.2) | 77/3 (96.2/3.8) | 0.345 |
| Pedicle screw – intact/ broken | 25/3 (89.3/10.7%) | 79/1 (98.5/1.5%) | 0.053 |
Table 4: Outcomes evaluated at 9 months follow-up.
We found no significant difference in the neurological and functional outcomes (Denis scale as indicated in Table-5) but the change in kyphotic angle between the immediate postoperative period and 9 months follow-up was significantly less in group-B.
| Denis scale (9months) | Group A (n=28) | Group B (n=80) | p value | ||
| No. | % | No. | % | ||
| Pain | |||||
| P1 | 11 | 39.3 | 22 | 27.5 | 0.24 |
| P2 | 14 | 50.0 | 54 | 67.5 | 0.09 |
| P3 | 3 | 10.7 | 4 | 5.0 | 0.29 |
| Work | |||||
| W1 | 12 | 42.8 | 27 | 33.7 | 0.38 |
| W2 | 11 | 39.2 | 42 | 52.5 | 0.22 |
| W3 | 3 | 10.7 | 9 | 11.2 | 1.0 |
| W4 | 2 | 7.3 | 2 | 2.5 | 0.26 |
Table 5: Denis’s scale assesment of functional outcome at 9 months.
P1- No pain, P2- Occasional, minimal pain without need for medication, P3- Moderate pain with occasional need for medication and no interruption of work or activities of daily living. W1- return to previous employment (heavy labor) or physically demanding activities, W2- Able to return to previous employment (sedentary) or return to heavy labor with lifting restrictions, W3- Unable to return to previous employment but working full time at a new job, W4- unable to return to full time work.
In 1995 Bao Shan MD et al assessed the long-term results of short-segment pedicle instrumentation for burst fractures of thoracolumbar and lumbar spine. They found at least one-grade improvement in the Frenkel neurological grading system in 90.8% of patients with loss of correction of anterior vertebral body height and cobbs’ angle of 1.9% and 12.10 respectively at final follow-up and they recommended more adequate fusion given suboptimal results [6]. Conghui Zhang, Yang Liu did a clinical trial from Jan 1980 to July 2017 and concluded that combined pedicle screw fixation at the fracture vertebrae may be better than traditional fixation across the fracture level alone for thoracolumbar fractures [7]. In 2016 Kunpeng Li, MD et al in their meta-analysis suggested that the Combined screw fixation technique was seen with better reduction of the fractured vertebrae, less loss of correction in the follow-up, and lower rate of implant failure [8] Dick et al and others [9][10][11][12] did in vitro biomechanical comparison evaluating the use of an intermediate screw on the pedicle at the fracture level, it showed that it could improve the stability of the pedicle screw fixation system and reduce the distribution of stress on each pedicle screw. In this study, the authors made an effort to compare the efficiency and safety of short-segment posterior spinal fixation for single-level thoracolumbar injury. We found no difference in the baseline demographic variables and injury characteristics other than significantly less kyphotic angle in group-B similar to the results found by lei wang et al and M.R. Farrokhi et al. [13][1] Postoperatively we found significant improvement in the kyphotic angle and ASIA score similar to available literature Khare S et al[14], Deng Z et al[15] with no significant difference in complication rates or implant failure similar to results of Zhang C et al (7)i.e, 0.63% implant failure in group A ( AFV - Adding fracture vertebrae) & 7.63% group B (CFV –cross fracture vertebrae). In our study we found that group-B patients had significantly less Change between post op & final follow-up kyphotic angle indicating that addition of index screw in the fractured vertebra helped in maintain the correction in the kyphotic angle better similar to results in the literature. (16)(6)(17). The functional outcomes measured by Denis scale were statistically similar in both groups.
For thoracolumbar spine injuries if required operative management with short segment posterior spinal fixation is an acceptable treatment option as it will help in stabilisation and indirect decompression of the spinal cord by correcting the kyphotic collapse and help in early mobilisation of the patient. Addition of index screw in the fractured vertebra will help in better kyphosis correction, less correction loss in kyphotic angle in the follow up, in addition to fewer instrument failures, without additional complications.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
