
Research | DOI: https://doi.org/10.31579/2578-8949/081
1 Associate Professor, Dermatology, Ad-din Women’s Medical College Hospital,Dhaka,Bangladesh
2 Associate Professor, Medicine, Ad-din Women’s Medical College Hospital, Dhaka, Bangladesh
3 Associate Professor, Dermatology, Moinamoti Medical College Hospital, Comilla
4 Ex-Professor, Dermatology, Ad-din Women’s Medical College Hospital, Dhaka, Bangladesh
5 Junior Consultant, Burn and Plastic Surgery, Dhaka Medical College Hospital
*Corresponding Author: Richmond Ronald Gomes, Associate Professor, Medicine Ad-din Women’s Medical College Hospital, Dhaka, Bangladesh.
Citation: K Rahman, R R Gomes, D Aktar, SM M Rahman, S M Rahman. (2021) Comparison of Rupatadine monotherapy and Combined Levocetirizine with Ranitidine dual therapy for the treatment of Chronic Idiopathic Urticaria. Dermatology and Dermatitis. 6(2); Doi:10.31579/2578-8949/081
Copyright: ©2021 Richmond Ronald Gomes, This is an open-access article distributed under the terms of The Creative Commons. Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 July 2021 | Accepted: 07 August 2021 | Published: 13 August 2021
Keywords: chronic idiopathic urticarial; antihistamine; itching; relapse
Background: Effective treatment for chronic idiopathic urticaria (CIU) with conventional combined therapy comprising H1 and H2 antihistamine is effective but associated with high relapse rate. Newer H1 blocker rupatadine alone is similarly effective with less relapse rate. Also it is convenient for the patient as similar efficacy is obtained with single dosage compared to 3 times dosing in combined therapy. This study was done to compare the traditional treatment with levocetirizine and ranitidine to a newly introduced antihistamine rupatadine for CIU.
Materials and Methods: The study was a hospital based prospective randomized control trial among 40 patients with CIU in Dermatology and Venereology department of Bangabandhu Sheikh Mujib Medical University(BSMMU), Dhaka from April 2020 to September 2020.Forty patients of CIU were randomly enrolled into two equal groups (group A and B). Patients of group-A were treated with 5 mg of levocetirizine once daily plus 150 mg of ranitidine twice orally daily and group-B were treated with rupatadine 10 mg once daily for one month. The efficacy was assessed 1st and 4th week during treatment and 4 weeks after completion of treatment by observing reduction of itching, regression of the size and shape of lesions and appearance of new lesions. Adverse effects and patient satisfaction were also noted.
Results: 75% patients in group A and 80% patients in group B responded to treatment (p>0.05).80% in group A and 85% in group B showed improvement in itching in the first week (p>0.05). . At the end of 4 weeks 95% showed improvement in each group. Appearance of new lesions in first week was 10% and 5% (p>0.05) and at 4th week, 5% and 0% respectively (p>0.05). 75% in group A and 80% in group B had regression in their lesions at the end of first week (p>0.05). At the end of 4th week, it was 85% and 90% (p>0.05). 40% in group A and 25% in group B had relapse of itching at follow up (p<0.05). Relapse of lesions were 35% and 20% (p<0.05). Overall occurrence of side effects (3 compared to 1) was more in group A.
Conclusion: The result of the present study show that both conventional treatment with levocetirizine and ranitidine combination and newer agent rupatadine alone has similar efficacy in reducing clinical sign and symptoms of CIU. But rupatadine has significantly reduced the relapse rate and so it is a more efficacious and also safer option with less adverse effects for the treatment of CIU in comparison to conventional treatment. Rupatadine is also more convenient option for patients in term of dosage schedule.
CIU is a relatively common skin condition with a 0.5% worldwide lifelong prevalence across different populations, affecting between 0.1% and 3% people in Europe and the ASIA [1]. The etiology is often unknown and a predominant physical urticaria and urticarial vasculitis have been excluded [1,2]. Studies investigating the natural history of CIU in adults have indicated that about 30–55% of patients go into remission within 12 months, although the disease may persist in some patients for several years [3-5].
Besides being severely debilitating and disfiguring, CIU may also be potentially stigmatizing, CIU get worse the Quality of Life, primarily as a result of sleep disruption, energy loss, fatigue, social isolation and emotional/sexual disturbances [6]. This condition follows a chronic course with spontaneous remission and relapses for several years [2]. Chronic urticaria etiology is often unknown [1]. There is increasing evidence for basophil and mast cell-mediated inflammation in urticaria and angio-oedema. Histamine and other mast cell mediators [including eicosanoids, cytokines, proteases, kinins and platelet activating factor (PAF) are involved in wheal development [1,2]. Because the symptoms of CIU, including oedema, erythema and pruritus, are primarily associated with histamine release from dermal mast cells, oral H1- receptor inverse agonists (H1 antihistamines) are the treatment of choice [2,7]. There is evidence that PAF and histamine have mutually complementary activities in vivo. Each mediator is able to promote the release of the other by different tissues and cells [8,9]. Dual blockades of these mediators is likely to be a more effective treatment strategy for CIU.
In chronic urticaria there are clinical trials and isolated observations with multiple treatments either as monotherapy or in combination, involving first and second-generation antihistamines, H2blockers, corticosteroids and many other drugs. Rupatadine is a novel selective long-acting histamine H1-receptor inverse agonist (H1 antihistamine), which is currently approved as a once daily dose of 10 mg. Rupatadine has recently been shown to have a higher affinity for the H1-receptor than fexofenadine and levocetirizine [10]. Rupatadine has shown both antihistamine and anti-PAF effects through its interaction with specific receptors and not due to physiological antagonism [11]. A previous dose-ranging study demonstrated that rupatadine 10 mg once daily for 4 weeks significantly decreased the severity of pruritus, the number of wheals and the total symptom score in patients with CIU, compared with placebo [12]. The aim of the present study was to compare efficacy and safety on CIU symptoms, treatment and patients’ satisfaction improvement with rupatadine monotherapy and combined levocetirizine and ranitidine dual therapy.
The study was conducted complying the declaration of Helsinki 1964.This prospective, randomized controlled trial was carried out in the outpatient department of dermatology and venereology, Bangabandhu Sheikh Mujib Medical University, Dhaka from April, 2020 to September 2020. Total 40 cases of CIU were selected. Patients were randomly allocated into two groups in a single blind fashion, group A and group B. Group A received conventional combination therapy (levocetirizine 5mg once daily plus ranitidine 150 mg twice daily for 4 weeks) while group B received oral rupatadine (10 mg once daily for 4 weeks.). The participants were evaluated one, and four weeks after commencement of the study. They were evaluated for improvement in symptoms (mainly pruritus), appearance of new lesions or resolution of previous ones. Count of lesions on the body was documented on every visit, for further evaluation of response to treatment. Data were collected anonymously. Confidentiality of data was ensured adequately and any unauthorized access to data was not possible. Collected data was analyzed statistically by using SPSS-12 (Chicago, Illinois).
Inclusion criteria: Patients with CIU (i.e. episodes of hives of characteristic wheal and flare appearance, occurring regularly, at least three times a week) for a period of at least 6 weeks during the last 3 months without an identifiable cause whose age was between 18 to 60 and attending OPD of Dermatology and Venereology, BSMMU, were recruited into the study.
Exclusion criteria:
1. Patients with physical urticaria (e.g. solar, heat, cold, aquagenic, cholinergic, contact, pressure, etc.),
2. Drug-induced urticaria, urticarial vasculitis, senile pruritus or hereditary angioedema.
3. Patients with any dermatological or any other clinically significant disease.
4. Patients who had received systemic and topical corticosteroids within last 4 weeks, desloratadine, loratadine, levocetirizine or cetirizine within 10 days, astemizole within 12 weeks, ketotifen within 2 weeks and patients who had received CNS acting agents (including tranquilizers, antidepressants, sedatives, hypnotics or antiepileptic) at any time.
5. Pregnant or breast feeding women.
This prospective, randomized controlled trial was conducted in the department of Dermatology and Venereology, BSMMU, Dhaka to compare the safety and efficacy and adverse effect between oral levocetirizine plus ranitidine combination and oral rupatadine alone therapy in CIU.A total of forty patients were included, twenty of them were given oral levocetirizine 5 mg once daily and oral ranitidine 150 mg twice daily. This group was designated as Group-A. .Twenty of them was given oral rupatadine 10 mg once daily .This group was designated as Group-B. In this study, 26 patients were male and 14 patients were female, male- female ratio was 1.86:1.Both groups were treated for one month. After collection of data, the data were assessed and analyzed with SPSS 12. The comparison between means was done by Independent sample‘t’ test for continuous variable. The result was considered significant if p value was ≤0.05.
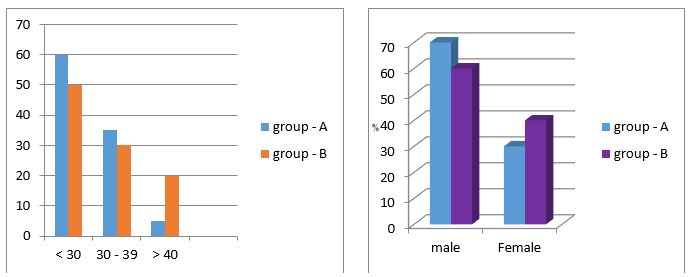
A total of forty patients were included, twenty of them were given oral levocetirizine 5 mg once daily and oral ranitidine 150 mg twice daily(Group-A.) Other twenty were given oral rupatadine 10 mg once daily. (Group-B). Both groups were treated for one month. Among the respondents, most of the patients (60%) in group A and (50%) in group B) were in the < 30> 40 years age group (Table 1). The mean age of the patients was 28.5 years and 30.85 years for group A and group B respectively. Lowest and highest ages were 18 and 55 years respectively. It appears from the study that 70% in group A and 60% in group B were male and 30% in group A and 40 % in group B were female (Table 1).

Current study revealed that 75% patients in group A and 80% patients in group B responded to treatment initially (Figure 2). In the first follow up visit, doctors examined each patient. The enrolled patient who had no itching, whales was considered cured. Patients whose itching was reduced and size and number of the lesions decreased, was considered responding to treatment. The patients who had new or persistent lesions were considered not cured. At first week of intervention uncured patients were prescribed repeat interventions. There was no significant difference in response to treatment between the two groups.

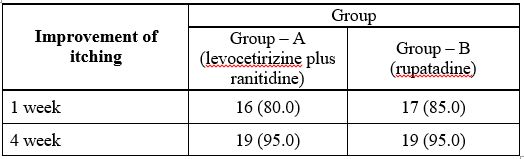
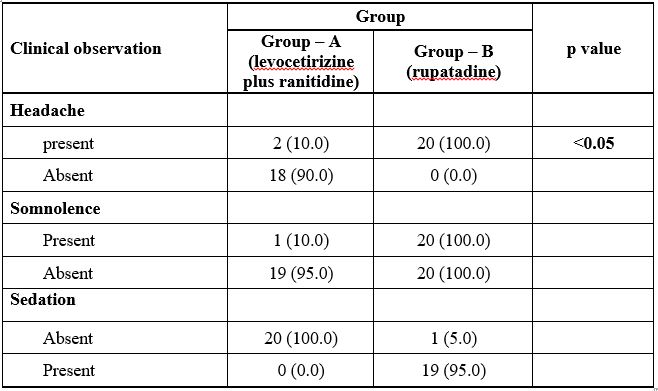
Current study showed 80% patients in group A and 85% patients in group B showed improvement in itching in the first week. At the end of 4 weeks 95% patients showed improvement and it was equal in each group (Table 2).
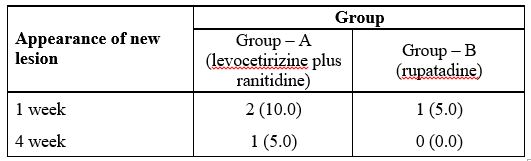
At 1st week, 2 patients in group A and 1 patient in group B had new lesions i.e. lesions at sites different from the primary lesions. After 4 week, 1 patient in group - A still had new lesion whereas, there was no new lesion appearing in the group - B patients (Table 3). Result was slightly better for group B, but not statistically significant.
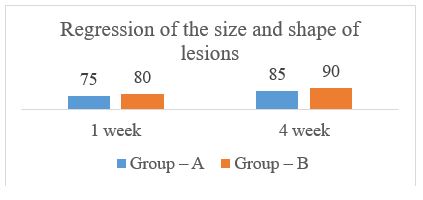
Current study revealed 75% of the patients in group A and 80% patients in group B had regression in their lesions in terms of disappearance, decrease in size, shape and distribution of the lesion at the end of first week. At the end of 4th week, 85% patients in group A and 90% patients in group B showed clinical improvement (Figure 3). The difference is again statistically insignificant.
All the three drugs included in this study were safe and was associated with very few side effects. Only one patient among 40 complained of mild sedation with rupatidine 10 mg after 1 week of treatment. Two patients in group A (levocetirizine plus ranitidine) complained of headache which is known side effect of levocetirizine. Another patient complained of somnolence which was again in the group A and was due to livocetirizine. Other common side effects of drugs like anaemia, jaundice, skin rashes were not seen among any group of patients. Overall occurrence of side effects (3 compared to 1) was more in group A and although clinically mild, difference was statistically significant (Table 4).
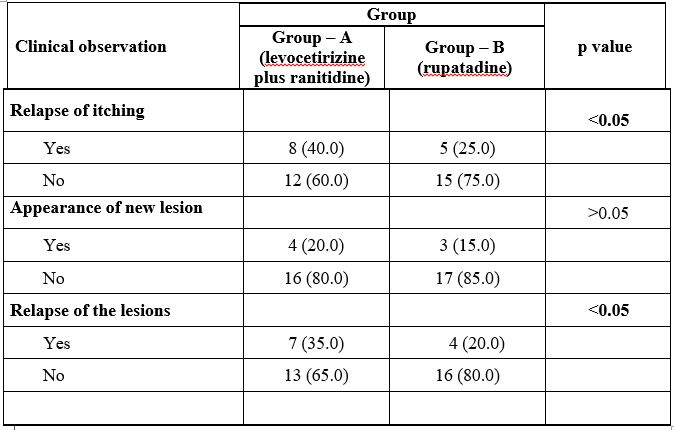
Post treatment follow up of patients was done 4 weeks after completion of treatment. It showed that 40% patients in group A and 25% patients in group B had relapse of itching in the previous site which was statistically significant. 20% patients in group A and 15% patients in group B had new lesions at sites different from the primary lesion. 35% patients in group A and 20% patients in group B had relapse of their previous lesions (Table 5). The differences were statistically significant. Thus, rupatadine showed significant improvement in relapse rate of CIU lesion over conventional treatment which is the main concern of CIU treatment at present.
It was quite evident that patient preferred single daily dosing (rupatadine) then taking 3 drugs daily at two different times. Patient’s satisfaction about treatment regime was randomly categorized as A (excellent), B (moderate) and C (not satisfied). 95% of Group– B patients were highly satisfied regarding treatment regime and described dose schedule as easy and convenient. On the other hand, 65% of the patients in group – A were moderately satisfied (B), 5% not satisfied at all (C) complaining of cumbersome dosing schedule (Table 6). Difference was statistically significant.

CIU is a highly prevalent in the general population which affects the quality of life [7, 14, 15, 16]. It is defined as the presence of wheals on a recurrent basis, more than twice a week, and during over six consecutive weeks [15,16]. Some studies show CIU accounts for nearly 75% of all cases of chronic urticaria [13]. Besides being severely debilitating and disfiguring, CIU may also be potentially stigmatizing. Chronic urticaria etiology is often unknown [1]. There is increasing evidence for basophil and mast cell-mediated inflammation in urticaria and angio-oedema. Histamine and other mast cell mediators [including eicosanoids, cytokines, proteases, kinins and platelet activating factor (PAF) are involved in wheal development [1,2]. There is evidence that PAF and histamine have mutually complementary activities in vivo. Each mediator is able to promote the release of the other by different tissues and cells [8,9]. Dual blockades of these mediators is likely to be a more effective treatment strategy for CIU.
Clinical trials revealed multiple treatment options such as first- and/or second generation antihistamines, H2 antihistamines, leukotriene antagonists, corticoids,cyclosporine and other immunosuppressors, calcineurin inhibitors, sulfasalazine, intravenous immunoglobulins, plasmapheresis or phototherapy [15]. Consequently, non-sedating (or second-generation) H1 antihistamines are considered as the first line symptomatic treatment [15, 16]. Rupatadine is a new potent nonsedative reverse H1 agonist and 10 mg of rupatadine is a fast, long-acting, efficacious and safe treatment option for the management of CIU [21]. There have been fewer studies with head to head comparison of individual antihistamines and combination of multiple options with a single antihistamine [7, 12, 15, 16].
In this study, 75% patients in group A and 80% patients in group B responded to treatment, however, the difference was not statistically significant. The study revealed that, 80% patients in group A and 85% patients in group B showed improvement in itching in the first week. In this study, at 1st week, 2 patients in group A and 1 patient in group B had new lesions and after 4 week, 1 patient in group - A still had new lesion whereas, there was no new lesion appearing in the group - B patients. Again, the difference was not statistically significant. In this study, 75% of the patients in group A and 80% patients in group B had regression in their lesions in terms of disappearance, decrease in size, shape and distribution of the lesion at the end of first week and at the end of 4th week, 85% patients in group A and 90% patients in group B showed clinical improvement. Current study revealed 40% patients in group A and 25% patients in group B had relapse of itching in the previous site; 20% patients in group A and 15% patients in group B had new lesions at sites different from the primary lesion; 35% patients in group A and 20% patients in group B had relapse of their previous lesions. The differences were statistically significant. This finding is also supported by other studies [2, 7, 12, 15, 16]. Thus rupatadine showed significant improvement in relapse rate of CIU lesion over conventional treatment which is the main concern of CIU treatment at present which is supported by other placebo control studies [16]. Though, head to head studies is yet too compared. All the three drugs included in this study were safe and was associated with very few side effects. Only one patient among 40 complained of mild sedation with rupatadine 10 mg after 1 week of treatment. Two patients in group - A (levocetirizine plus ranitidine) complained of headache which is known side effect of levocetirizine. Another patient complained of somnolence which was again in the group A and was due to livocetirizine. Other common side effects of drugs like anaemia, jaundice, skin rashes were not seen among any group of patients. Overall occurrence of side effects (3 compared to 1) was more in group A and although clinically mild, difference was statistically significantIt was quite evident that patient preferred single daily dosing (rupatadine) then taking 3 drugs daily at two different times. Patient’s satisfaction in found more in rupatadine group than the other group and the difference was statistically significant. This finding is supported by other repeated studies [2, 7, 12, 15, 16].
The present study had the following limitations. Factors should be kept in mind while deciding on the implications of the findings of the study such as the small sample size, lack of objective assessment tools, single center-based study. Additional rigorously conducted prospective randomized trials with large sample sizes, full reporting of outcomes and double blinding of assessors are required. Increase transparency is needed if the sample cohort of patients is reported on in different studies and avoidance of multiple publications is strongly recommended.
The result of the present study show that both conventional treatment with levocetirizine and ranitidine combination and newer agent rupatadine alone has similar efficacy in reducing clinical sign and symptoms of CIU. But rupatadine has significantly reduced the relapse rate and so it is more efficacious and also safer option with less adverse effects for the treatment of CIU in comparison to conventional treatment. Rupatadine is also more convenient option for patients in term of dosage schedule.
The present study did not represent the actual scenario in Bangladesh because it was conducted in one tertiary level hospital (BSMMU) in Dhaka city only. Sample size and duration of the study was short. The long term results of the operative procedure could not be assessed. There is also lack of appropriate disease severity assessment tool.
There were no conflicts of interests
Appropriately taken
Self-funded
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
