
Research Article | DOI: https://doi.org/10.31579/2578-8965/105
1University Witten-Herdecke, Department of Obstetrics and Gynecology, Academic Hospital Cologne Weyertal University of Cologne, Germany
2Department of Obstetrics and Gynecology, University Witten-Herdecke, Marien-Hospital, Witten Marienplatz, 258452, Witten, Germany
3Department of Obstetrics and Gynecology Academic Hospital Cologne Weyertal University of Cologne, Germany
*Corresponding Author: Elvin Piriyev, University Witten-Herdecke, Department of Obstetrics and Gynecology, Academic Hospital Cologne Weyertal University of Cologne, Germany
Citation: Piriyev E., Schiermeier S. , Römer T. (2021) Comparison of pipelle and hysteroscopy with D&C in postmenopausal patients. J. Obstetrics Gynecology and Reproductive Sciences 5(9) DOI:10.31579/2578-8965/105
Copyright: © 2021: Elvin Piriyev, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 November 2021 | Accepted: 11 November 2021 | Published: 16 November 2021
Keywords: pipelle; hysteroscopy; D&C; endometrial carcinoma; postmenopausal bleeding
Objective: The aim of the study is to compare the pipelle method and hysteroscopy with D&C in postmenopausal patients
Methods: In this prospective study, only those postmenopausal patients with postmenopausal bleeding and/or with a sonographically highly developed endometrium who were referred for hysteroscopy with D&C were included. A total of 92 patients were included in this study. Before each procedure, patients were explicitly informed about the study and gave consent. On the condition of anonymity of personal data (surname and first name, date of birth) and after signing a special informed consent form, the patients were allowed to be included in the study. The study was performed as a double-blind study. The obtained histologies (from pipelle and D&C) were sent separately to the same pathologist.
Results: The group with malignant and premalignant findings has a central role in our study. After evaluation of the histologically malignant findings from the pipelle and the D&C, the sensitivity of the pipelle in our study was 82%.
Conclusion: Endometrial biopsy is an important step to exclude endometrial carcinoma in postmenopausal bleeding. The aim is to minimize the burden and invasiveness of the procedure while maintaining a high degree of diagnostic certainty to avoid unnecessary invasive surgery. The pipelle sampling can be used as an outpatient method without anaesthesia during routine examination. Our study shows that this method of sampling is a safe, accurate and cost-effective outpatient procedure with high sensitivity for the detection of endometrial carcinoma.
Abnormal uterine bleeding is a common gynecological problem causing 33% of outpatient presentations. In the pre-menopausal and postmenopausal age groups, it accounts for as many as 69% of the presentations [1].
Investigating of postmenopausal bleeding is crucial in order to determine whether the cause is of a benign nature or due to an endometrial carcinoma [2]. Any postmenopausal bleeding should be assumed to be a carcinoma until proven otherwise [3]. Postmenopausal bleeding is most common in the age group of 55–59-year-olds [4]. In contrast, the highest incidence of endometrial cancer is between the ages of 75 and 79 and endometrial carcinoma is the 7th most common malignancy in women worldwide, with an annual incidence of 142,000 new cases [5, 29]. Postmenopausal bleeding is more common in women who have not taken hormones [6]. Postmenopausal bleeding is special among bleeding cases because this phase of life has the highest incidence of endometrial carcinoma, and postmenopausal bleeding is often the initial symptom for endometrial carcinoma (the most common genital carcinoma in women). Thus, new-onset bleeding at this stage of life requires special clinical attention [7]. Postmenopausal bleeding is associated with an increased risk of endometrial carcinoma even if the endometrium cannot be visualized sonographically [8]. Common causes of bleeding also include endometrial polyps and endometrial hyperplasia; however, submucosal fibroids may also be relevant to bleeding. [7, 9]. The risk of endometrial carcinoma in asymptomatic postmenopausal women with an endometrial thickness of >11mm is approximately equal to that of postmenopausal women with postmenopausal bleeding and an endometrial thickness of 5mm. The relative risk of endometrial carcinoma is 6.7% in both collectives [10]. Histological examination of the removed tissue is an obligatory requirement for a definitive diagnosis. Hysteroscopy and D&C are the gold standard of endometrial diagnostics [11, 12]. However, in recent decades, thanks to newer simplified diagnostic and therapeutic methods, management has changed [3]. In addition, the surgical risk of general anaesthesia, infection, and perforation still exists [11, 12]. This has led to new and simpler methods for endometrial biopsy, including the pipelle instrument [13, 14]. The pipelle is less expensive compared to hysteroscopy with D&C [15]. Although the pipelle is included in many guidelines, it is rarely used in practice in Germany. However, there are still concerns about the informative value of the obtained sample, especially in the case of focal intrauterine changes [14].
In this prospective study, only those postmenopausal patients with postmenopausal bleeding and/or with a sonographically highly developed endometrium who were referred for hysteroscopy with D&C were included.
Post-menopause was defined (according to WHO) as the period beginning 12 months after the last menstrual period. Any bleeding during this period was defined as a postmenopausal bleeding [6, 7].
A total of 92 patients were included in this study. Before each procedure, patients were explicitly informed about the study and gave consent. On the condition of anonymity of personal data (surname and first name, date of birth) and after signing a special informed consent form, the patients were allowed to be included in the study.
Preoperative transvaginal sonography for endometrial assessment and hysteroscopy were mandatory requirements of this study.
Pipelle sampling was performed as part of the usual planned procedure under general anaesthesia. After disinfection of the external and internal genital organs and speculum insertion without fixation and dilatation of the cervix as well as probing the uterus (exceptions only in individual cases), the pipelle was inserted through the cervical canal into the fundus of the uterus. It was then possible to determine the probe length using the printed scale. Then the plunger of the pipelle was pulled out as far as possible to achieve an optimal vacuum. The suction curette was pushed back and forth in the uterus several times with simultaneous rotations in order to obtain examination material from all around the cavity. The pipelle was then completely withdrawn from the uterus. This was followed by planned hysteroscopy and D&C.
The study was performed as a double-blind study. The obtained histologies (from pipelle and D&C) were sent separately to the same pathologist. The pipelle material was labelled with a specific number without patient data. Unblinding of the materials was performed if carcinomas, atypical hyperplasia, or other suspicious findings (of unclear cause) were found in the biopsies. In these cases, the findings were assigned to the patients and compared with the histology of the D&C.
Since complex hyperplasia has a higher risk of coexisting with atypical hyperplasia and/or endometrial carcinoma than simple hyperplasia without atypia, it was evaluated separately.
Pipelle sensitivity was calculated:
Sensitivity = (true positive/ true positive + false negative) X 100.
The age of the patients was between 44 and 97, with the largest group being age group between 50 and 55 years (Figure 1).
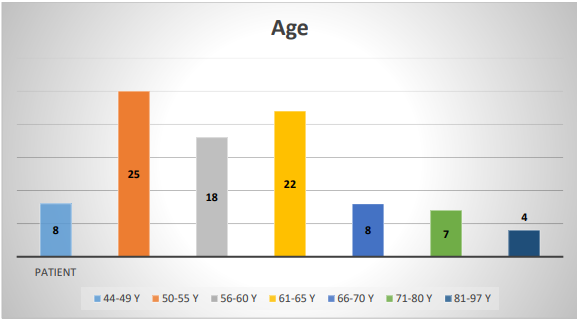
Fig. 1 Age groups of female patients
11 patients (12%) had a double endometrial thickness of <5>10 mm.
The indication for hysteroscopy with D&C was postmenopausal bleeding in 74 cases (80.4%) and a sonographically high endometrium in 18 cases (19.6%), with an average double endometrial thickness of 12 mm in asymptomatic patients.
Figure 2 shows the histologic findings obtained by hysteroscopy with D&C.
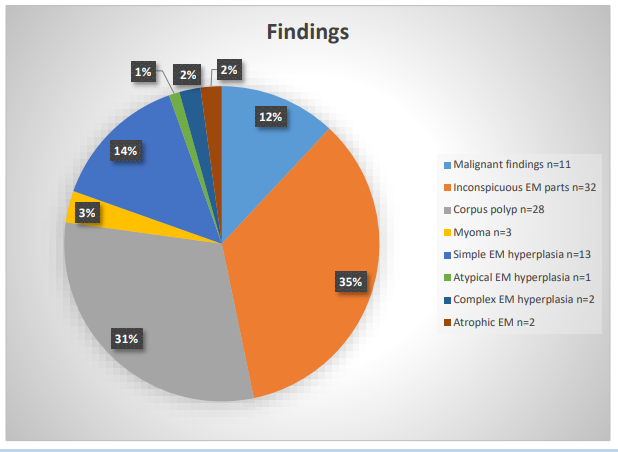
Fig.2 Histological findings obtained by hysteroscopy with D&C
13 patients had malignant findings. Of these hysteroscopy with D&C was able to detect the findings in 11 cases and using the pipelle method 9 cases were detected (Table 1).
| Case | Double EM Thick-ness | Pipelle | Curettage | Uterus |
| 1 | 6 mm | Endometrial carcinoma | Endometrial carcinoma | Endometrial carcinoma |
| 2 | 6 mm | Endometrial carcinoma | Endometrial carcinoma | Endometrial carcinoma |
| 3 | 8 mm | Endometrial carcinoma | Endometrial carcinoma | Endometrial carcinoma |
| 4 | 10 mm | Endometrial carcinoma | Endometrial carcinoma | Endometrial carcinoma |
| 5 | 11 mm | No atypia | Focal atypicalendometrial hyperplasia | Focal endometrial hyperplasia without atypia (complex hyperplasia) |
| 6 | 13 mm | Complex hyperplasia (without atypia) | Complex hyperplasia (without atypia) | Endometrial carcinoma |
| 7 | 13 mm | No atypia | Endometrial carcinoma | Endometrial carcinoma |
| 8 | 14 mm | No atypia | Focal complex hyperplasia (without atypia) | Focal endometrial carcinoma |
| 9 | 16 mm | Endometrial carcinoma | Endometrial carcinoma | Endometrial carcinoma |
| 10 | 16 mm | Endometrial hyperplasia without atypia (complex EM hyperplasia) | Endometrial carcinoma | Endometrial carcinoma |
| 11 | 19 mm | Suspicious finding. Cause cannot be clearly assessed. | Endometrial carcinoma | Endometrial carcinoma |
| 12 | 23 mm | Endometrial carcinoma | Endometrial carcinoma | The patient has refused further therapy |
| 13 | 23 mm | Endometrial carcinoma | Endometrial carcinoma | Endometrial carcinoma |
| 14 | 28 mm | Sparse EM-portions with focal strong decidual stromalreaction. Suspicious findings | Cx: necrotic tissue parts. Suspicious findings | Intramurally developed endometrial stromal sarcoma. |
Table 1 Overview of malignant and premalignant findings
The accordance of the pipelle method with the D&C was calculated for individual findings in the total group as well as in the subgroups, depending on the endometrial double thickness (Table 2).
| Total | <5mm> | 5-10 mm | >10mm | |||||||||
| Findings | Curettage | Pipelle | Accordance | C | P | A | C | P | A | C | P | A |
| Inconspicuous endometrium parts | 32 | 31 | 97% | 7 | 7 | 100% | 21 | 20 | 95% | 4 | 4 | 100% |
| Corpus polyp | 28 | 2 | 7% | 2 | 0 | 0% | 13 | 1 | 7,7% | 13 | 1 | 7,7% |
| Myoma | 3 | 0 | 0% | - | - | - | 2 | 0 | 0% | 1 | 0 | 0% |
| Atrophic endometrium | 2 | 1 | 50% | 1 | 0 | 0% | 1 | 1 | 100% | - | - | - |
| Simple endometrial hyperplasia | 13 | 5 | 38,5% | 1 | 0 | 0% | 5 | 3 | 60% | 7 | 2 | 28,6% |
Complexe endometrial hyperplasia without atypia | 2 | 1 | 50% | - | - | - | - | - | - | 2 | 1 | 50% |
Atypical endometrial hyperplasia | 1 | 0 | 0% | - | - | - | - | - | - | 1 | 0 | 0% |
| Malignant | 11 | 9 | 82% | - | - | - | 4 | 4 | 100% | 7 | 5 | 71,4% |
Table. 2 Accordance of the pipelle with theD&C
The aim of this study is to investigate the sensitivity of the pipelle in the group with postmenopausal patients. A correlation between endometrial thickness and pipelle sensitivity could not be investigated due to the small number of patients with endometrial thickness <5mm>10mm (Table 2). Our previous study showed that although the probability of obtaining an adequate sample is largely independent of endometrial thickness in the overall population regardless of menopausal status, it increases for individual findings at an endometrial thickness greater than 5mm [16]. The study by Elsandabesee and Greenwood [17], who examined 97 patients with postmenopausal bleeding, showed that in a group of women with an endometrial thickness of <5mm>
The sensitivity of the pipelle depends on the type of findings (Tab. 2). In the case of an unremarkable endometrium, the pipelle showed a 97
The pipelle biopsy was carried out under anaesthesia.
Endometrial biopsy is an important step to exclude endometrial carcinoma in postmenopausal bleeding. The aim is to minimize the burden and invasiveness of the procedure while maintaining a high degree of diagnostic certainty to avoid unnecessary invasive surgery. In practice, various methods of endometrial sampling and endometrial assessment are used. Hysteroscopy combined with a D&C is a minimally invasive procedure usually performed under general anaesthesia. By contrast, the pipelle sampling can be used as an outpatient method without anaesthesia during routine examination. Our study shows that this method of sampling is a safe, accurate and cost-effective outpatient procedure with high sensitivity for the detection of endometrial carcinoma.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
