
Research Article | DOI: https://doi.org/10.31579/2637-8892/248
*Corresponding Author: Delaram Dehnashi, Ramírez Hinojosa Ma, Lucina Family Therapy Institute CENCALLI Mexico City.
Citation: Ramírez Hinojosa Ma, (2024), Comparison of Family Functioning Between Women with and Without Motor Disabilities, Psychology and Mental Health Care, 8(3): DOI:10.31579/2637-8892/248
Copyright: © 2024, Ramírez Hinojosa Ma. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 December 2023 | Accepted: 04 March 2024 | Published: 14 March 2024
Keywords: mbsr; emotion; quality of life; multiple sclerosis
Multiple Sclerosis, an autoimmune disease, can significantly impact a person's daily functioning and overall well-being. Patients often experience emotional disorders and find it challenging to regulate their cognitive-emotional responses during the course of their illness. The objective of this current study was to evaluate the impact of MBSR training on quality of life of patients with Multiple Sclerosis (MS). The study consisted of 40 participants with multiple sclerosis, all of whom were enrolled in the MS Society of Shiraz in Fars Province, Iran. The participants were evenly divided into two groups: an experimental group of 20 individuals and a control group of 20 individuals. The experimental group underwent a series of eight MBSR training sessions, held once a week for 60 minutes over a period of 60 days. The control group did not receive any interventions. The findings of the present study demonstrate a notable disparity between the experimental and control groups in terms of quality of life, specifically in areas such as physical function, pain management, mental well-being, energy levels, health perception, and cognitive function in relation to health changes (P<0.05). However, while these differences were statistically significant, no significant differences were noted among the dimensions of role limitation caused by physical problems, mental challenges, and social functioning (P>0.05). The results of the present study showed that MBSR training improves some dimensions of the quality of life in patients with Multiple Sclerosis and reduced negative emotion regulation strategies.
For the World Health Organization (WHO), the family is understood as a group of people who make up the household and have some degree of kinship by blood, adoption or marriage1.
The Structural Systemic School defines the family as a natural group that over time has developed patterns of interaction; these constitute the family structure, which in turn governs the functioning of its members, defines their range of behaviors and facilitates their interaction with each other2 ; It is also known as a powerful primary system, to which a person belongs; it is a living system, in constant transformation that is modified over time in order to ensure continuity and psychosocial growth of its members and also involves multiple factors that modify its conformation, structure and family dynamics3.
The family structure functions as an interactive and interdependent unit; and when an event or experience occurs that affects one member of the group in particular, it affects the rest of the members, i.e. all members are affected and involved in the disability process, this impact may be at different levels and dimensions of their daily life4.
At this point, a reorganization within the family is necessary, which on the one hand leads to the individuation of each of its members and on the other hand provides a feeling of belonging, security and warmth3. For this reason, the family plays an important role in the process of assimilation and acceptance of disability and its different challenges. Parents tend to react in different ways to the disability of one of their members, which may depend on their degree of severity, vulnerability, their strengths, the stage of the life cycle they are going through, the medical, economic, social, educational aspects and the social support network they have 5,6.
It has been documented that illness, disability and death are universal experiences that place families before one of life's greatest challenges and involve different reactions in each member of the family Interacting with a member with a disability involves adapting to its different phases and demands 5,6.
The family impact of disability is reflected in the appearance of various reactions and affects such as: feelings of helplessness, aggressiveness, guilt, anger, ambivalence and fear of the future, and even emotional discomfort (anxiety, depression) physical discomfort (illness) or even abandonment, neglect and violence for the person with disability, which are characteristics of unresolved grief 7,8.
In this way, the presence of a member with a disability generates the need to modify family roles in order to adapt, which will become more complex as they demand high levels of availability and tolerance for the care and attention of the person, so that flexibility and adjustment to new demands will allow the construction of opportunities and alternatives for the entire close family nucleus 6,7.
As mentioned above, the presence of a child with a disability becomes a stressful event within the family and can trigger the breakdown of marital and family relationships. Parents often become directly and exclusively responsible for the education and rehabilitation of their child with a disability. In a study of parents of children with Down's syndrome, it was observed that they use the same parenting skills as parents of children without disabilities, but the differences lie in the high degree of parental stress due to the cognitive disability, which generates strong emotional stress4,8.
Various studies point out that the processes of overprotection, care and exclusion are more evident in women with disabilities in any of their manifestations, as they are the group who live longer with the family of origin, have higher illiteracy rates, have fewer years of schooling, are less employed in companies, and have fewer opportunities for development within the company8.
These differences corroborate what several studies have pointed out: women with disabilities experience double discrimination they are often excluded from different family and social processes because they are women, and not considered competent because they have a disability or physical limitation 9,10,11.
The present study aimed to investigate the impact of motor disability on the family functioning of women with disabilities and to compare them with women without disabilities.
Familyfunctioning instrument
The family functions scale that was applied, is made up of items with factor loadings greater than or equal to .40, was standardized in the Mexican population, is made up of 22 items, divided into 4 factors, and its response style is on a Likert scale12.
| Factor | Positive family environment | Cohesion and rules | Hostility and conflictavoidance | Command Problems in the expression of feelings |
| Items | (7) 12,14,15,17,18,21,22 | (5) 1,6,10,9,19 | (5) 2,3,5,16,20 | (5) 4,7, 8,11,13 |
Note. Overall Cronbach's Alpha of .8533
Table1: Family functions scale factors
Procedure, materials and subjects
A standardized family functions scale was administered in a Mexican population to adult women with and without motor disabilities, all of them of legal age, who agreed to participate in the study.
A sample of 203 women, who agreed to participate in the study on a voluntary basis, was formed, the participants were informed of the objective of the study and their personal data were treated with confidentiality.
The family functions scale was applied in different hospitals in Mexico City12 where they received medical and rehabilitation treatment. A total
sample of 203 women was recruited, interviewed and given a semi-structured interview on socio-demographic aspects.
A group of 100 women with motor disabilities and a second group of 103 people without disabilities were formed. This group was collected in hospitals, schools and recreational centers.
The study was a quantitative, comparative and correlational one-measurement study, with a significance level of p≤ 0,05.
The results obtained from the socio-demographic data are presented in the following table:

Table2: Description data
A comparison of means between the groups of Women with disability (WwD) and Women without disability (WsD) was performed and no significant differences were found with respect to family functioning.
| Scala | WwD | WsD | ||||||
| M | DE | M | DE | gl | t | p | ||
| Family functions | 57.1 | 6.4 | 56.9 | 5.4 | 200 | .294 | .769 |
Note. N=203. WwD n=100 WsD n=103. Difference in average
*p≤.05. **p≤.01.
Table 3: Analysis comparison of total mean
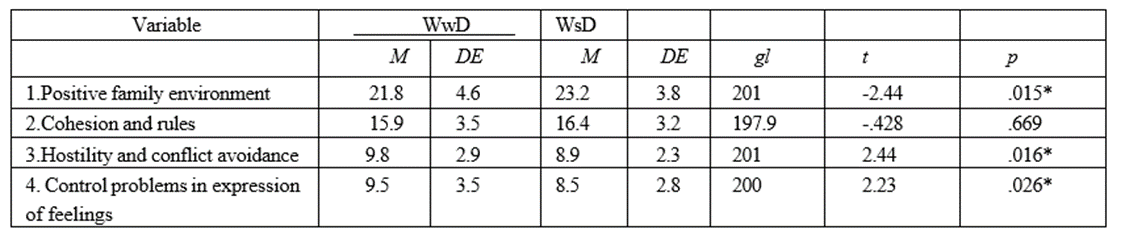
The following table shows the results of the comparison of means between the factors of the scale for both study groups, carried out by means of Studen' t-test, with the following results: differences were observed in the factors positive family environment in WwD (M=21. 8, SD=4.6), in WwD (M=23.2, SD=3.8), cohesion and norms WwD (M=15.9, SD=3.5), in WwD (M=16.4, SD=3.2), hostility and conflict
avoidance WwD (M=9. 8, SD=2.9), in WsD (M=8.9, SD=2.3), and in the factor command problems in expressing feelings WwD (M=9.5, SD=3.5), in WsD (M=8.5, SD=2.8).
The significant differences detected between the two groups on the family functioning scale were in the factors: positive family environment, hostility and conflict avoidance and problems in expressing feelings.
Note. N=203. WwD n=100 WsD n=103.
*p≤.05. **p≤.01.
Table 4: Analysis of differences of meansby factor scale family functions
The socio-demographic data show important differences between the two groups: the first group of WwD has a lower educational level, lives longer with the family of origin, lives less in a couple and has fewer years of vocational training, which shows that the group of women with disabilities experiences different levels of exclusion and backwardness compared to the WsD group [10].
To determine whether the differences between the two groups were significant, a comparison of means per factor of the scale applied was carried out, in this analysis it was observed that the WwD group presented significant differences in positive family environment, where they scored low, but not in the factors hostility and conflict avoidance, and problems in the expression of feelings, where the difference was significant, a high mean was obtained in relation to the WsD.
The results indicate that the family environment is perceived by WwD less positive, they have a perception of greater hostility, they determine for conflict avoidance and identify greater problems in the expression of feelings, which implies less expression of their feelings, discomfort or discomfort, disagreements, as well as states of wellbeing 7,9.
It was also observed that the group of women with disabilities perceive their family environment with more negative and excluding aspects compared to the group without disabilities, which may hinder their personal development and their adaptation to the social environment 7,11.
Parents are important figures who must adapt to each of the stages of disability (diagnosis, treatment, rehabilitation, education, employment) and where changes in family functioning will be determinant in achieving family cohesion, building harmonious relationships, facilitating the adjustment of roles and the redistribution of tasks within the family 4,5,6.
Therefore, in the care process, the family must be considered, addressing the various conflict dynamics that can be generated within the family, which can become sources of conflict and stress among its members. Influencing family functioning will facilitate the process of acceptance and adaptation to disability 4,5,7 as several studies have pointed out, the attitude of acceptance of disability is strongly related to the adaptation of the family group[7,8].
Family functioning is important in the construction of strategies and the development of adaptive psychological resources. Some of these structural elements within the family are: the autonomy of each of the members, the existence of clear limits, flexibility in the face of changes, the expression of affection in a clear and direct way, openness to information and the creation of new relationships outside the family group5,6. A positive family environment in which conflict resolution and the expression of emotions, as well as disagreement, are favored are determining factors in the development of problem-solving strategies [2,3].
It is common for parents to focus more on the member with a disability, which can lead to abandoning or neglecting the other members (children, partner), which has an impact on the quality of affective relationships, coming to perceive the member with a disability in a negative way, sick, and promoting hostile and competitive relationships within the family[5,7].
Several studies point out that it is common for parents to focus on the disabled member, which can lead to abandoning or neglecting the other members of the family (children, partner), which has repercussions on the quality of affective and fraternal relationships, leading to a negative perception of the disabled member, or perceiving him or her as ill, which fosters hostile and competitive relationships between family members[5,7].
Knowing the characteristics of families in the face of the challenge that disability implies is of utmost importance, as a series of links and experiences are developed in the family that will be fundamental for the person in the process of adaptation, this will allow them to achieve greater adjustment and adaptation in various spheres of their development [4,5,7].
Disability is an experience that brings families into strong and constant states of tension and involves facing challenges, deconstructing the family system where all members can express their emotions. In the study, WwD rated themselves as having lower family functioning compared to the group of non-disabled women. The differences detected in the study were located in the factors less positive family environment, greater hostility and conflict avoidance and greater problems in the expression of feelings. Clinical work with the family and with the person with disabilities in the different facets of their evolutionary cycle is recommended in order to achieve greater integration of the experience and its intrinsic challenges.
Acknowledgments to women who agreed to participate in the study. Funding None.
Conflicts of Interest Author declare that there is no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
