
Research Article | DOI: https://doi.org/10.31579/2578-8965/170
Department of Obstetrics and Gynaecology, Jawaharlal Nehru Medical College, A.M.U., Aligarh 202002 (U.P.)
*Corresponding Author: Nasreen Noor, Department of Obstetrics and Gynaecology, Jawaharlal Nehru Medical College, A.M.U., Aligarh 202002 (U.P.)
Citation: Nasreen Noor, Heena Samreen, Nishat Akhtar, Shazia Parveen, (2023), Comparison of Causes of Maternal Near Miss and Maternal Mortality in a Tertiary Care Hospital: A Prospective Study, J. Obstetrics Gynecology and Reproductive Sciences, 7(3) DOI:10.31579/2578-8965/170
Copyright: © 2023, Nasreen Noor. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 May 2023 | Accepted: 29 May 2023 | Published: 05 June 2023
Keywords: maternal near miss; maternal death; who quality care; severe life-threatening complications
The Maternal Near miss (MNM) concept has led to a more comprehensive and better assessment of the effect of care on maternal health. Investigating severe life-threatening pregnancy complications that women encounter and maternal morbidities (near misses) may help evaluate the quality of care in health facilities and recommend ways to improve maternal survival, especially in poor resource settings.
Aim
This study aimed to identify causes, classify, and determine the nature of complications in maternal near misses and in maternal death.
Material and Methods
The hospital-based prospective cohort study was conducted in the Department of Obstetrics and Gynecology, Jawaharlal Nehru Medical College, Aligarh Muslim University of Aligarh from 2020 to 2022. The study was approved by the Institutional Ethics Committee and informed written consent was obtained from the study participants. The outcome measures included causes, organ dysfunction, complications, maternal morbidities, and neonatal outcome.
Results: Higher rate of unbooked referrals was observed in our study. Hemorrhage was 42.9%, followed by 39.1% hypertensive disorders, 8.6% sepsis in the maternal near miss group while in the maternal mortality group, 26.1% had hypertensive disorders followed by 23.8% women had hemorrhagic disorders, and 20.4% had sepsis. There was a significant difference in HDU, ICU Hospital stay and IUDs in the maternal mortality group compared to the maternal near-miss group.
Conclusion
The WHO near-miss approach was found to represent a feasible strategy in low-resource settings each Near Miss should be evaluated in detail to diagnose underlying pathology, correct and timely detection of complications, prompt referral and early institution of essential and comprehensive obstetrics care are important for maternal and infant survival.
According to estimates from the World Health Organization (WHO), 287.000 maternal fatalities occurred in 2010 with developing regions bearing 85% of the global burden [1,2]. One of the eight Millennium Development Goals (MDGs) and a significant challenge for the healthcare system is reducing maternal mortality (MM).The goal is to reduce the maternal mortality ratio (MMR) by 75
The hospital-based prospective cohort study of pregnancy-related complications in the facility in line with the WHO definition of maternal near miss and mortality criteria was conducted in the Department of Obstetrics and Gynecology, Jawaharlal Nehru Medical College, Aligarh Muslim University of Aligarh during 2020 to 2022. The study was approved by the Institutional Ethics Committee, Faculty of Medicine, written informed consent was obtained from the woman and her attendant, in case she was not fit to give consent and data was collected according to the structured performa developed for the purpose of the study. After detailed history and examination the demographic profiles like age, parity, booking status, gestational age, life threatening condition at arrival or became so later on, h/o previous LSCS, adverse events, disorders, organ system dysfunction were noted. Any underlying medical disorder in these patients such as anemia, diabetes, hypertension was included to study their possible contributory role in the near miss situation. Those who fulfill the WHO criteria for maternal near miss were included in our study groups Those who survived were included in this study as maternal near miss. Those who did not survive were also included for comparision with the MNMM and MD because the disorders and adverse events are the same in both categories.
Group I: Maternal near miss
Group II: Maternal mortality
Information on demographic characteristics, maternal and perinatal information, process indicators, and near-miss screening were abstracted from patient files daily on the maternity wards. The data were entered into an electronic data entry platform every day and shared with the study primary investigators every week. On-site data quality checks were conducted daily and analyzed by SPSS latest version.
A total of 970 maternal near misses were enrolled in this study after fulfilling the inclusion and exclusion criteria. There were 88 maternal deaths registered during the study period. The study groups allocated are as follows
Group I: Maternal near miss (n= 882)
Group II: Maternal Death (n=88)
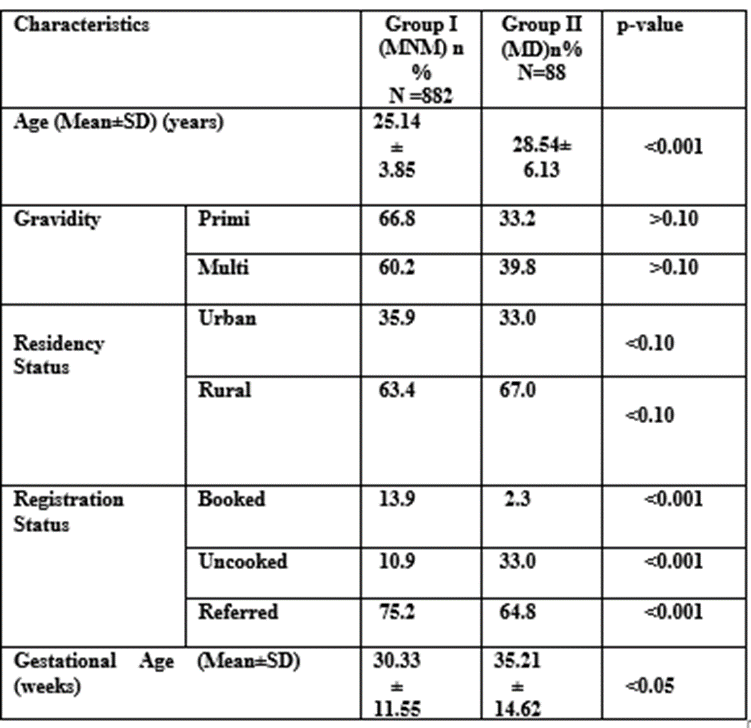
Table 1: Women characteristics of near-miss cases and maternal death.

Table 2: Underlying disorders in Group 1 and Group 2.
(NOTE- A patient can have more than one diagnosis at the time of admission. Percentage is calculated out of 882 cases in group I and 88 cases in group II)
Hemorrhagic disorders (42.9%) were the leading cause of near- miss followed by hypertensive disorders of pregnancy (39.1%), sepsis (8.6%), cardiac illness (1.4%), and Hepatic disorder (1.4%). Hypertensive disorders of preg nancy (26.13%) Hemorrhage (23.8%) and sepsis (20.4%) constituted the leading causes of mortality.

Table 3- Types of hypertensive disorder in Group 1 and Group 2.
Among hypertensive disorders in near miss women, 234 women (26.5%) had severe pre-eclampsia followed by antepartum eclampsia 119 (13.5%), postpartum eclampsia, HELLP syndrome 31 (3.5%), chronic hypertension 21(2.4%) and 8 women (0.9%) were diagnosed with PRES syndrome whereas among women who had a maternal death 31 women (35.2%) had post-partum pre-eclampsia followed by antepartum eclampsia 29 (33%), severe pre-eclampsia, 22(25%), HELLP syndrome and PRES syndrome 2 (2.3.%). So both groups statistically significant differences (p-value less than 0.001)
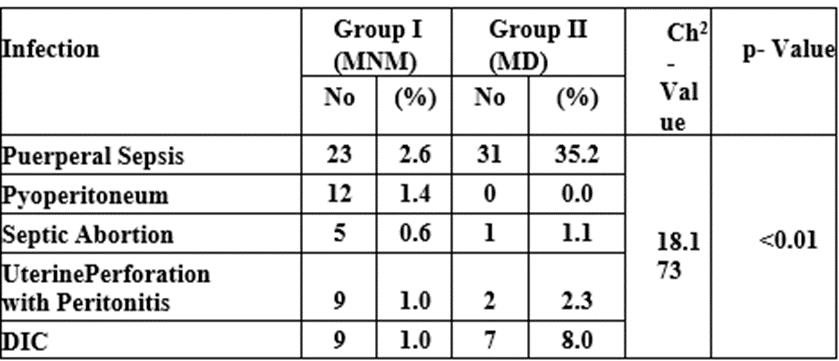
Table 4: Distributon of infection in Group 1 and Group 2
Among 58 women with near-miss with infection, 23 (2.6%) had puerperal sepsis, 12 (1.4%) had pyoperitoneum, 5 (0.6%) had and 9 (1%) had both uterine perforations with peritonitis and DIC due to puerperal sepsis, whereas among 41 women who had a maternal death, 31 women (35.2%) had sepsis followed by 7 (8%) with septic DIC, 2(2.3%) uterine perforation with peritonitis and 1 (1.1%). So both groups had statistically significant differences (p-value greater than 0.001).
The introduction of the maternal near miss (MNM) concept has resulted in a more thorough and accurate assessment of the impact of care on maternal health than was previously possible.
Comparability difficulties should be taken into account, especially in low-income countries, when adopting the standard WHO criterion [10].
There should therefore be MNM criteria that are appropriate and can be applied consistently.
[11The focus has now shifted from the investigation of maternal mortality conditions in retrospect to the early detection and prompt care of pregnancy-related problems that can put a woman at risk for serious maternal outcomes.
[12] There were 882 identified maternal near-miss mothers in all.
The number of maternal deaths during the study period was 88. The high prevalence of MNM in our study was also reported in studies from other low-income countries, which used similar near-miss criteria [13,14,15]
The mean age of nearmiss cases in the current study was 25.10 3.85 years, and the mean age of maternal deaths was 28.54 6.13 years. These results are similar to those of Kalra et al. [16] and Vinita Singh et al. [17]. According to our findings, there were 10.9% vs. 29.3% vs. 33.3% unbooked ladies in each group. In the referenced categories, there were the most women. The same outcomes were noted by Chandrakanta P[18]. Because this hospital has a NICU, ICU, and 24hour blood bank facility, many cases are being directed there. In the current study, 13.9% of women were scheduled in MNM, compared to 2.3% in the MD group in this institution, which is less than Almeria et al. [19]'s figure of 36.4%. They manifest as high-risk cases and are being supervised with better facilities in the hospital to provide better antenatal care and regular follow-up as it is a tertiary care hospital.
Our study population contributed more from the rural area as compared to urban settings with was comparable with the study of Hana et al [20]
The proportion of primigravidas was more in our study which is comparable with the results of Gupta D et al [21] who also found primipara women more in both near misses (60.8 %) and maternal death groups (60.0 %) Our results were not comparable with the study of Chandrakanta Prasad et al[18] Waterstone et al. [22] and Morse et al. [23] to the present study regarding the period of gestation >36 weeks (35.80%) near miss.
In most of the Indian studies, hemorrhage (42.9%) accounted for the leading cause of maternal morbidity followed by hypertensive disorders (39.1.%) disorders. Similar to the majority of studies conducted in India, haemorrhage (42.9%) was the top cause of maternal morbidity, followed by hypertension disorders (39.1%), but in our study, haemorrhage (23.8%) and hypertensive disorders (26.13%) were the two largest causes of maternal death. Twenty-four percent of the causes were due to sepsis. Pregnancy-related eclampsia and hypertension were the leading causes of maternal fatalities. If antihypertensive medications, injection of MgSO4, diligent blood pressure monitoring, and an early pregnancy termination choice are made, these women may be saved. Haemorrhage, or PPH, was the second leading cause of maternal death (postpartum haemorrhage). APH brought on by abruptio placentae, placenta previa, placenta accrete, and percreta was actively controlled by the use of LSCS. When intra-operative blood loss could not be stopped with the use of platelet, PRBC, and FFP transfusions and other precautionary measures, a caesarean hysterectomy was ultimately necessary.
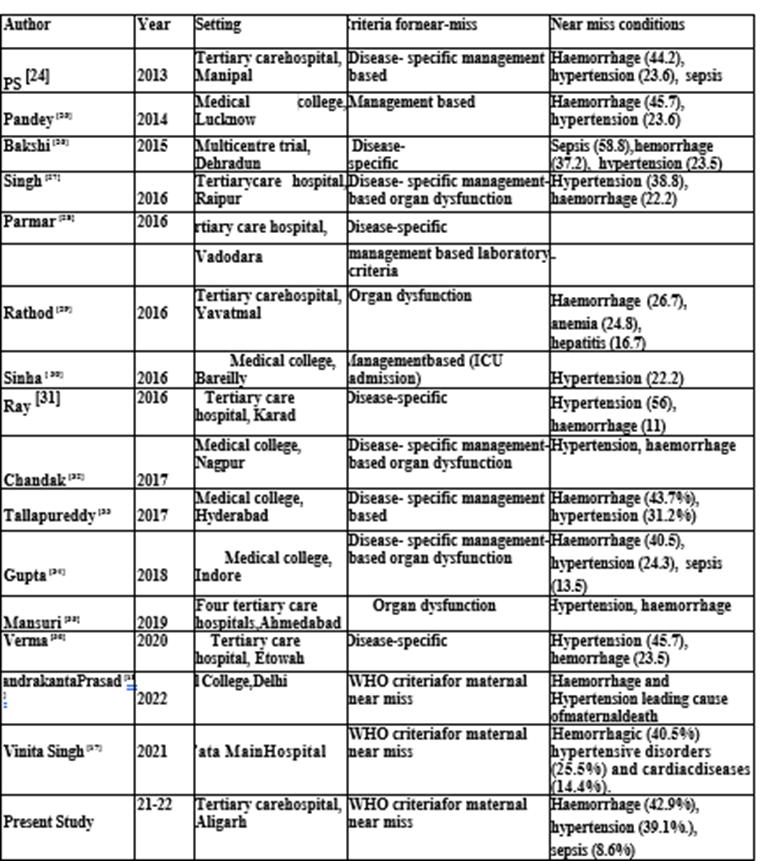
Table 5: List of studies on maternal near-miss done in different parts of India for comparison with our study
Several initiatives have been undertaken in our hospital to improve our response to obstetric emergencies over the last few years. An obstetric high dependency unit (HDU/ICU) has been established. Fast-tracking of blood and blood components available from the blood bank has been streamlined. Monthly audit of mortality women to identify preventable factors and implement protocols adhering to National Guidelines and current evidence-based practices. However, the impact of these quality initiatives on obstetric care needs to be quantitatively assessed by a future study.
At our tertiary centre, maternal near misses (MNM) are frequent.
In low-resource situations. The WHO near-miss approach was found to represent a feasible workable strategy in low resource settings. Maternal near miss (MNM) is common at our tertiary center. Haemorrhage was a leading cause of maternal near misses while hypertensive disorders are the main cause of maternal death in our study.
The main limitation of the current study was its duration and sample size. More data collection over a few years with a large sample size will provide better and more comprehensive information about maternal health status.
All procedures performed in studies involving human participants were following the ethical standards of the institution.
Informed consent was obtained from all the individual participants included in the study.
Nil
None
Data collection and data analyzed by Hina Samreen. the manuscript was written by Nasreen Noor. Proofreading and editing are done by Nishat Akhtar and Shazia Parveen.
We would like to acknowledge all the faculty members, paramedical staff, and women who participated in carrying out this research work at Jawaharlal Nehru Medical College, AMU, Aligarh.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
