
Research Article | DOI: https://doi.org/10.31579/2641-0419/252
1 Department of Internal Medicine, Michigan State University, East Lansing, Michigan, USA.
2 Department of Cardiology, Michigan State University, East Lansing, Michigan, USA.
*Corresponding Author: Rohan Madhu Prasad, Sparrow Clinical Research Institute 1200 E. Michigan Ave, Suite 550 Lansing, MI 48912 517-364-5728.
Citation: Rohan Madhu Prasad, Sandeep Banga, Esosa Ukponmwan, Ahmed Elshafie, Heesoo Yoo. et all (2022). Comparing Polymer-Free and Polymer-Coated Drug-Eluting Stents in Coronary Artery Disease: An Updated Meta-Analysis. J. Clinical Cardiology and Cardiovascular Interventions, 5(3); Doi:10.31579/2641-0419/252
Copyright: © 2022 Rohan Madhu Prasad, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 February 2022 | Accepted: 28 February 2022 | Published: 04 March 2022
Keywords: transfemoral access; multiple co-morbidities; iliofemoral tortuosity or calcification; carotid approach
Transfemoral (TF) access is the safest and the most preferred option for Transcatheter Aortic Valve Implantation (TAVI). However, femoral access is often difficult in a significant number of patients due to inadequate vessel diameter, iliofemoral tortuosity or calcification. Other access routes for TAVI include transapical, transaortic, subclavian, axillary, carotid and transcaval. Choice of vascular access requires both extensive preoperative work-up and adaptive intraprocedural planning by the heart team. Here, we present a challenging case of TAVI in an elderly patient with peripheral artery disease, which required a change in the vascular access site from femoral to carotid artery, midway during procedure, as a strategy to prevent untoward vascular complications. This case also highlights the limitations of current hardware and technologies in negotiating tricky situations.
The field of percutaneous coronary interventions (PCI) for patients with coronary artery disease (CAD) has undergone several advancements over the years, from bare-metal stents to polymer-coated drug-eluting stents (PC-DES) and now polymer-free drug eluting stents (PF-DES). The second type is known to consist of either permanent polymer (PP-DES) or bioresorbable polymer (BP-DES). [1] However, these polymers have been associated with stent-related complications and higher inflammatory and thrombogenic responses. [2,3] PF-DES have been developed for their advantage of drug-release control in the absence of a polymer. [2-4] PF-DES releases its, where the drug was released through micropores instead of a polymer. Intravascular imaging has demonstrated that this method allows for early endothelization and neointimal coverage within one month after implantation. [2-4] The recently published guidelines for coronary artery revascularization from American College of Cardiology (ACC), American Heart Association (AHA), and Society for Cardiovascular Angiography and Interventions (SCAI) indicated that patients undergoing PCI should receive DES as compared to bare metal stents (Class of Recommendation 1, Level of evidence A). [5] However, no mention of PC-DES, PP-DES, BP-DES, or PF-DES was made in the guidelines. Therefore, to delineate the difference between the different DES we conducted an updated meta-analysis to compare PC-DES versus PF-DES in patients with CAD receiving PCI. We also performed new additional analyses to evaluate the effect based on the follow-up period and the specific difference between PF-DES and PP-DES and BP-DES.
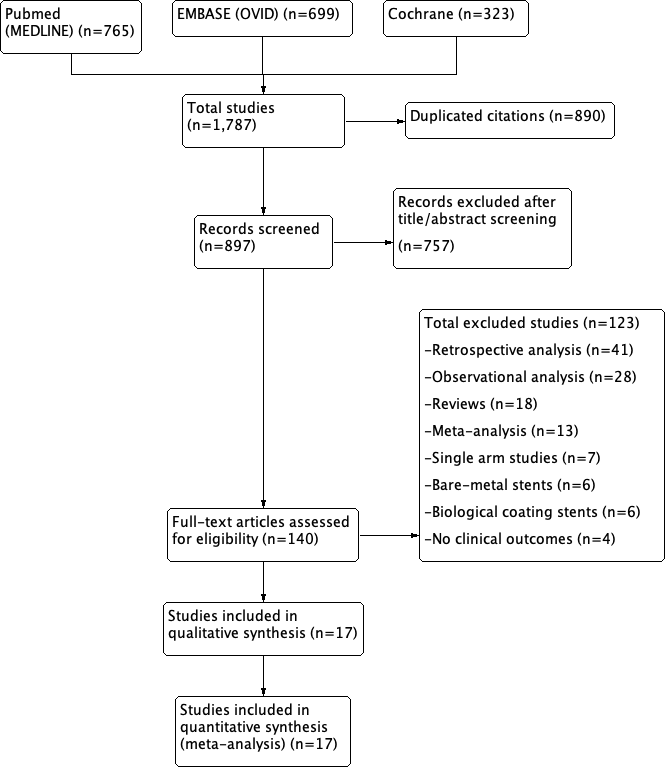
We conducted a comprehensive search of the electronic databases of PUBMED, EMBASE, and COCHRANE from inception to December 2021 for relevant studies. The inclusion criteria consisted of: (1) a prospective double-arm study or arandomized controlled trial (RCT), (2) comparison PF-DES versus a type or both of PC-DES, (3) patients with CAD, (4) reported either efficacy or safety outcomes, and (5) human subjects. Exclusion criteria were the following: (1) ongoing or irretrievable data, (2) single-arm study, (3) retrospective study, (4) use of bare-metal stents or COMBO stents, (5) use of animals, and (6) no clinical outcome endpoint. This meta-analysis was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines and registered on the International Prospective Register of Systematic Reviews (PROSPERO).
The search included the following keywords: “polymer”, “free”, “drug-eluting stent”, ‘“randomized trial”, “meta-analysis”, and “mortality”. Two authors (RMP and SB) independently reviewed the search results, extracted potential articles, and assessed their eligibility. The Cochrane Collaboration risk-of-bias tool was used by two different authors (RMP and SB) to assess the quality of the included studies.
The primary outcome of this meta-analysis was all-cause mortality. Secondary outcomes included cardiac death, recurrent target vessel myocardial infarction (TV-MI), target lesion revascularization (TLR), and stent thrombosis. Stent thrombosis was defined as definite and probable thrombosis as per the Academic Research Consortium-2. [6] For each outcome, subgroup analyses were performed to analyze the data based on follow-up duration. Short-term follow-up was defined as less than 1 year, mid-term was 2-5 years, and long-term was greater than 5 years. An additional analysis was conducted for the primary outcome of all-cause mortality to specifically compare PF-DES vs the different types of PC-DES (PP-DES or BP-DES). We also collected baseline characteristics of the included studies and patients.
Statistical analysis was conducted using Review Manager (RevMan), version 5.4 (The Cochrane Collaboration, Copenhagen, Denmark).
The Mantel-Haenszel random-effects models were used to estimate the odds ratios, 95% confidence intervals, and p-values. Two-sided p values of <0>
Seventeen RCTs were included with a total of 15,098 patients and a median-weighted follow-up of 3.23 years (Figure 1).
(6-23) of the included studies, the exact PF-DES varied per the study, but the common stents were Sirolimus-eluting, Paclitaxel-eluting, Sirolimus- and Probucol-eluting, as well as Amphilimus- and Sirolimus-eluting. (Table 1) As for the control group of PC-DES, the majority of the trials used PP-DES, but two trials used BP-DES [9,23] and two trials used a combination of PP-DES and BP-DES [12,16] The average age of the included patients was 66.3 years, 73.9% were males, 27% were smokers. In regards to the patient’s medical history, 39.5% had diabetes mellitus, 70.2% had hypertension, 58.1% had dyslipidemia, 20.6% had a previous myocardial infarction, and 18.8% had a previous percutaneous coronary intervention. (Table 2)
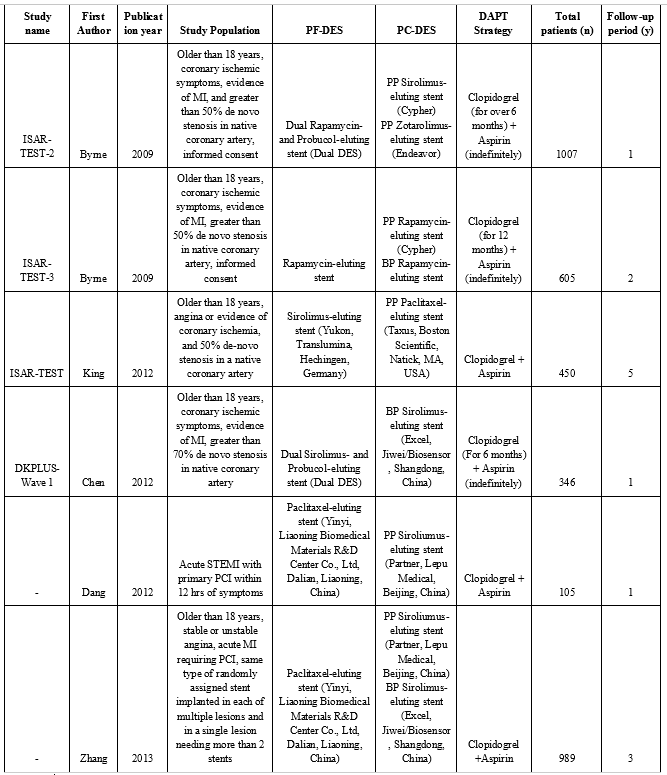
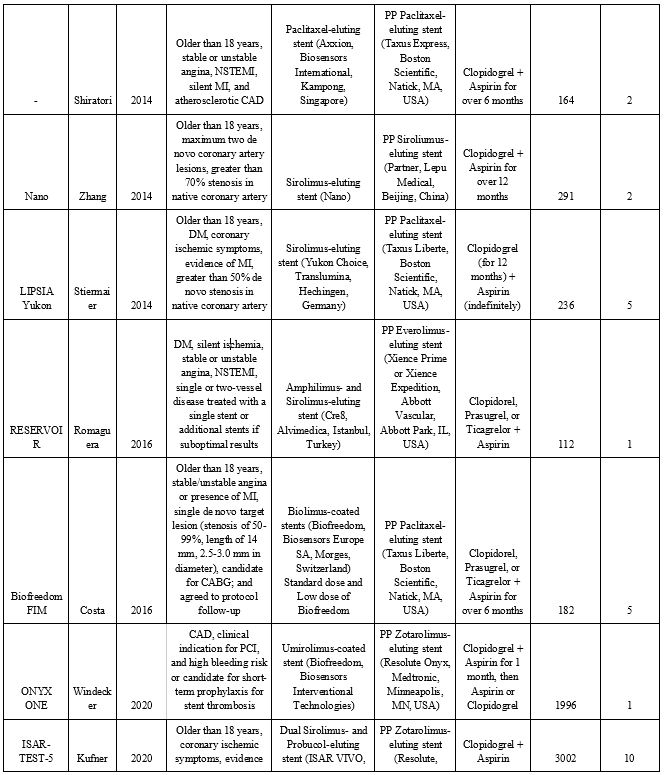
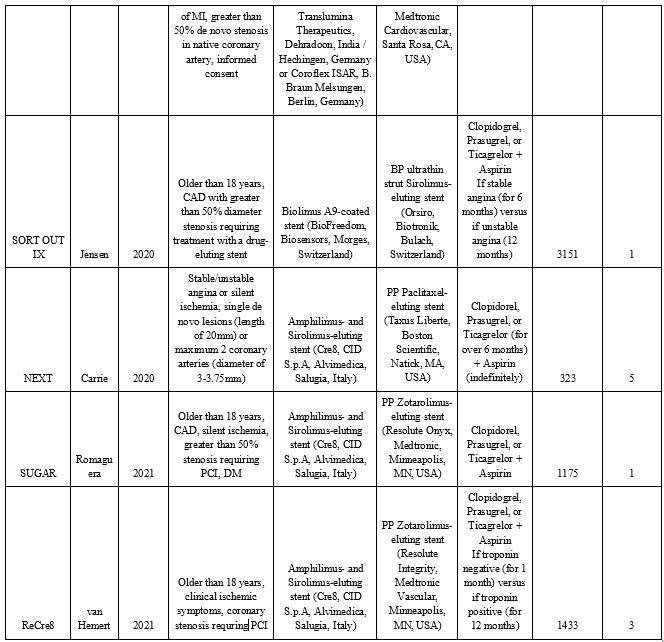
Table 1: Characteristics of included studies
| Study | Patients in PF-DES arm (n) | Patients in PC-DES arm (n) | Age (y) | Males | Smokers | Diabetes mellitus | Hypertension | Dyslipidemia | Previous Stroke | Previous MI | Previous PCI |
| ISAR-TEST-2 2009 | 333 | PP Sirolimus 335 PP Zotarolimus 339 | 67.0 ± 11.1 | 772 (76.7) | 185 (18.4) | 276 (27.4) | 672 (66.7) | 662 (65.7) | NR | 134 (13.3) | 89 (8.8) |
| ISAR-TEST-3 2009 | 201 | PP 202 BP 202 | 66.1 ± 10.7 | 480 (79.0) | 99 (16.4) | 166 (27.4) | 410 (67.8) | 416 (68.8) | NR | 199 (32.9) | 69 (11.4) |
| ISAR-TEST 2012 | 225 | 225 | 66.7 ± 10.4 | 346 (76.9) | 82 (18.2) | 131 (29.1) | 297 (66.0) | 335 (74.4) | NR | 143 (31.8) | 50 (11.1) |
| DKPLUS-Wave 1 2012 | 173 | 173 | 63.8 ± 10.9 | 271 (78.3) | 96 (27.8) | 96 (27.8) | 237 (68.5) | 106 (30.6) | NR | 52 (15.3) | 67 (19.4) |
| Dang 2012 | 50 | 55 | 66.2 ± 13.2 | 73 (69.5) | 67 (63.8) | 27 (25.7) | 46 (43.8) | 23 (21.9) | 8 (7.6) | 6 (5.7) | 2 (1.9) |
| Zhang 2013 | 327 | PP 321 BP 341 | 66.2 ± 10.5 | 670 (67.7) | 410 (41.5) | 282 (28.5) | 652 (65.9) | 425 (42.9) | NR | 51 (5.0) | 94 (9.5) |
| Shiratori 2014 | 80 | 84 | 65.6 ± 9.3 | 119 (72.6) | 31 (19) | 53 (32.3) | 120 (73.2) | 101 (61.6) | NR | 51 (31.1) | 47 (28.7) |
| Nano 2014 | 143 | 148 | 57.4 ± 10.3 | 223 (76.6) | 150 (51.5) | 49 (16.8) | 156 (53.6) | 90 (30.9) | NR | 88 (30.2) | 40 (13.8) |
| LIPSIA Yukon 2014 | 120 | 116 | 67.2 ± 9.3 | 162 (68.6) | 59 (0.3) | 236 (100) | 230 (97.5) | NR | NR | 52 (22.0) | 71 (30.0) |
| RESERVOIR 2016 | 56 | 56 | 67.0 ± 9.3 | 84 (75.0) | 65 (58.0) | 112 (100) | 95 (85.0) | 92 (82.1) | 14 (12.5) | 30 (27.0) | 41 (36.6) |
| Biofreedom FIM 2016 | 122 | 60 | 67.2 ± 8.8 | 127 (69.7) | 29 (15.9) | 50 (27.5) | 155 (85.0) | 131 (71.9) | NR | 36 (19.7) | 73 (40.1) |
| ONYX ONE 2020 | 1003 | 993 | 74.1 ± 9.7 | 1330 (66.6) | 201 (10.1) | 770 (38.6) | 1603 (80.3) | 1262 (63.2) | 259 (13.0) | 513 (25.7) | 467 (23.4) |
| ISAR-TEST-5 2020 | 2002 | 1000 | 67.9 ± 11.0 | 2295 (76.4) | 523 (17.4) | 870 (29) | 2002 (66.7) | 1907 (63.5) | NR | 885 (29.5) | 284 (9.5) |
| SORT OUT IX 2020 | 1572 | 1579 | 66.3 ± 10.9 | 2440 (77.4) | 880 (27.9) | 607 (19.3) | 1743 (55.3) | 1607 (51.0) | NR | 458 (14.5) | 633 (20.1) |
| NEXT 2020 | 162 | 161 | 64.7 ± 10.3 | 233 (72.1) | 79 (24.5) | 87 (26.9) | 208 (64.4) | 200 (61.9) | NR | 29 (9.0) | 49 (15.0) |
| SUGAR 2021 | 586 | 589 | 67.9 ± 10.2 | 888 (75.6) | 255 (21.7) | 1122 (95.5) | 981 (83.5) | 956 (81.4) | 102 (8.7) | 200 (17.0) | 258 (22.0) |
| ReCre8 2021 | 721 | 712 | NR | 1094 (73.4) | NR | 284 (19.0) | NR | NR | NR | NR | NR |
Abbreviations: BP, bioresorbable polymer; MI, myocardial infarction; n, number; NR, not reported; PC, polymer coated; PCI, percutaneous coronary intervention; PF, polymer free; PP, permanent polymer; y, years
Table 2: Baseline characteristics of included patients
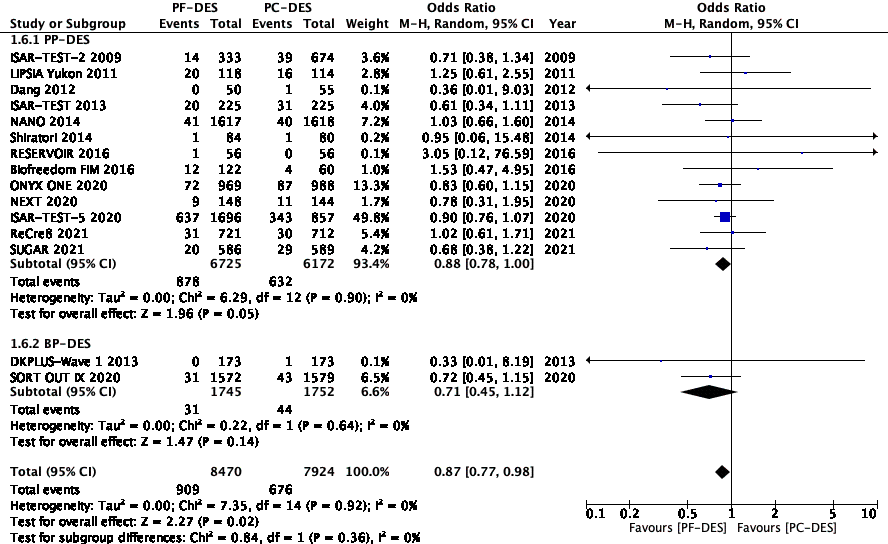
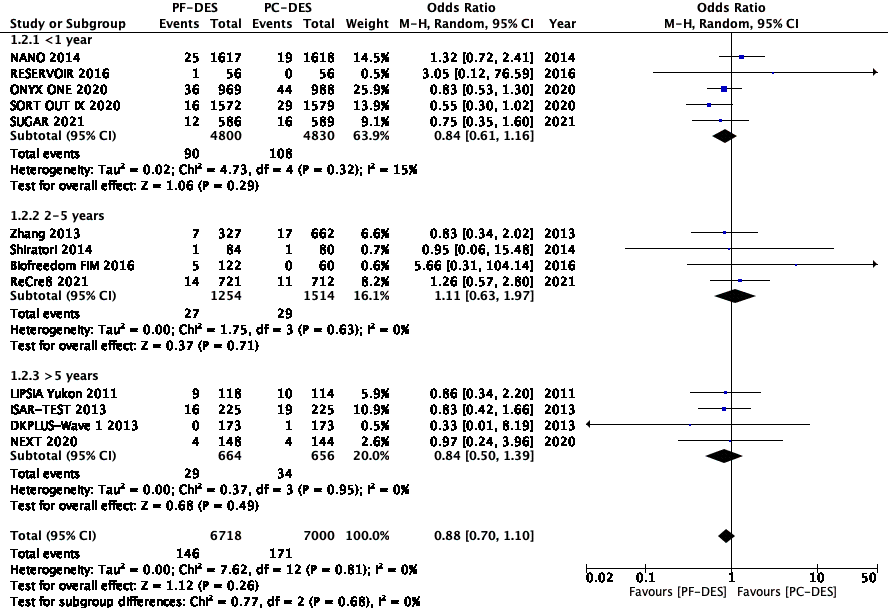
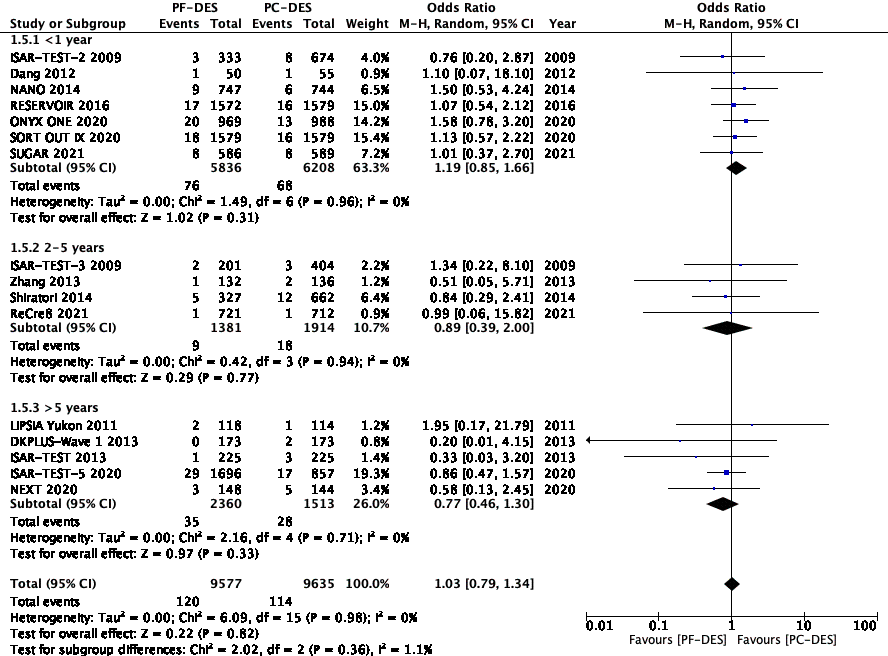
In regards to the primary outcome of all-cause mortality, the statistical analysis showed that it was significantly decreased in the PF-DES group (PF-DES 10.3% vs PC-DES 7.9%, p=0.02, I2=0) (Figure 2). The subgroup analysis based on follow-up duration illustrated that the significance of all-cause mortality was specifically seen in the short-term (PF-DES 3.5% vs PC-DES 4.3%, p=0.04, I2=0) (Figure 2). The results insignificantly favored PF-DES in the mid-term (PF-DES 22.2% vs PC-DES 15.0%, p=0.28, I2=0) and long-term (PF-DES 7.4% vs PC-DES 9.0%, p=0.28, I2=0) setting (Figure 2).

An additional analysis was done to compare all-cause mortality in PF-DES vs PC-DES when separating PC-DES into PP-DES or BP-DES. Interestingly, all-cause mortality favored PF-DES in this analysis –
Significantly when compared to PP-DES (PF-DES 13.1% vs PC-DES 10.2%, p=0.05, I2=0) and insignificantly when compared to BP-DES (PF-DES 1.8% vs 2.5%, p=0.14, I2=0) (Figure 3).
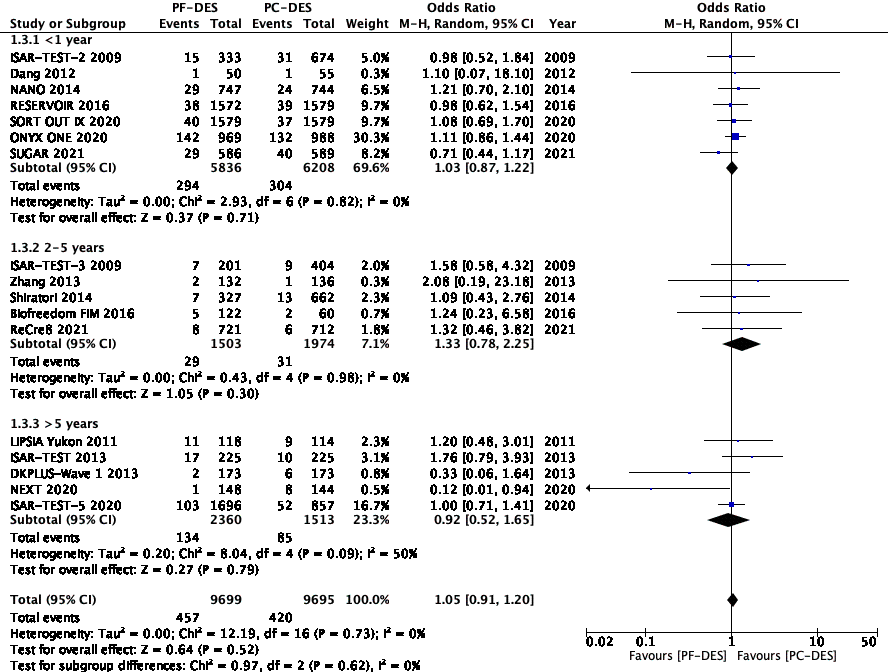
There was no difference in cardiac death between the two groups (PF-DES 2.2% vs PC-DES 2.4%, p=0.26, I2=0) (Figure 4).
Furthermore, there was no difference in the recurrent TV-MI (PF-DES 4.7% vs PC-DES 4.3%, p=0.52, I2=0) and the subgroups based on follow-up duration had similar results (Figure 5).
Overall TLR had similar rates (PF-DES 11.7% vs PC-DES 8.7%, p=0.33, I2=67) (Figure 6). Finally, there was no difference in stent thrombosis overall (PF-DES 1.3% vs PC-DES 1.2%, p=0.82, I2=0) or in any of the subgroups (Figure 7).
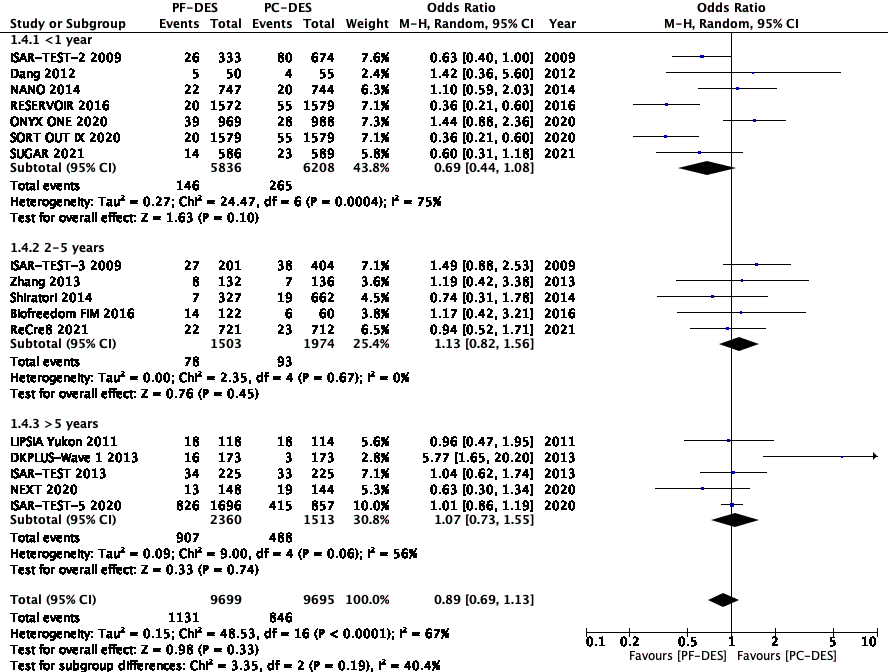
The heterogeneity for these statistics was mainly low, but overall ranged from low to moderate. The two results with elevated I2 values were TV-MI and TLR. A rule-one-out sensitivity analysis was conducted for these outcomes. After excluding the NEXT trial [21], the long-term results of TV-MI showed no difference between the two groups (PF-DES 6.0% vs PC-DES 5.6%, p=0.70, I2=20), which was consistent with the initial findings. For TLR, the DKPLUS-Wave 1 [9] and ONYX ONE [19] trials were excluded, which resulted in the following findings: overall (PF-DES 12.6% vs PC-DES 9.6%, p=0.07, I2=62), short-term (PF-DES 2.2% vs PC-DES 4.5%, p=0.007, I2=60), and long term (PF-DES 40.7% vs PC-DES 36.2%, p=0.92, I2=0). This analysis demonstrated that TLR favors PF-DES - insignificantly overall and significantly in the short-term setting. In this meta-analysis, major adverse cardiovascular events was not analyzed, but all the components were analyzed separately.
Although the ACC, AHA, and ACSO have recommended DES for coronary artery revascularization, there are no recommendations as to which type of DES is preferred. [5] The PC-DES type, which compromises of PP-DES and BP-DES, has been associated with stent-related complications and higher inflammatory and thrombogenic responses. [2,3] Therefore, PF-DES have been developed in efforts to alleviate these complications. This meta-analysis was conducted with the objective of comparing PF-DES and PC-DES. The statistical analysis showed that all-cause mortality was significantly decreased in the PF-DES group, specifically when compared to PP-DES and only in the short-term follow-up.
The recently published RCT ONYX ONE by Windecker et al evaluated Umirolimus-coated PF-DES and Zotarolimus-eluting PP-DES in patients with high bleeding risk who were receiving a PCI. The study found that PF-DES was non-inferior to PP-DES in terms of a composite of all-cause mortality, TV-MI, or stent thrombosis as well as target lesion failure. [19] Additionally, Romaguera et al conducted the SUGAR trial to compare Amphilius- and sirolimus-eluting PF-DES and Zotarolimus-eluting PP-DES in patients with diabetes mellitus who were undergoing PCI. This study also showed that the rates of TLF between PF-DES and PP-DES were non-inferior. [18]
The physical difference between PP-DES, BP-DES, and PF-DES may be a source of the results seen in this meta-analysis. The polymer in PP-DES was designed to achieve drug adherence on the stent surface and control drug release. [2] However, the struts have been associated with chronic inflammation and delayed endothelization, which leads to delayed vascular healing, hypersensitivity reactions, and neoatherosclerosis. This immune response explains the higher rate of events, such as mortality and thrombosis, with when using PC-DES. [2,3,24,25]
Our results demonstrated that the effects of PF-DES were mainly seen in the short-term follow-up and when compared to PP-DES. We hypothesize this is the case because the PF-DES are endothelialized in about a month; whereas, the PP-DES are present permanently. With this hypothesis, the PF-DES should also have significant benefits in the long-term, but our meta-analysis was not able to accurately depict this outcome. Moreover, the insignificant favoring of PF-DES over BP-DES can be explained as the BP-DES have polymers that are bioresorbable, as their name indicates, and also have been associated with improved outcomes. [24,25] However, there were only two studies that directly compared PF-DES and BP-DES, so further studies are needed to confirm these findings.
In addition to the limitations inherent to a meta-analysis, we found a significant difference between the patient population. Three of the studies only included diabetic patients, [13,14,18] which is significant because diabetic patients have a higher rate of all-cause mortality and TLR [26]. Thus, these studies could’ve skewed our results. Additionally, within the PF-DES and PC-DES there were varying types of stents used, including drugs and PP-DES versus BP-DES. The Biofreedom FIM study had two separate groups that received a PF-DES, standard and low dose of Biolimus. [7] Although benefits were mainly found in all-cause mortality with PF-DES, they were not found with cardiac mortality or stent thrombosis. Thus, the mortality benefit may not actually depend on the type of stent placed. Further RCTs should be conducted to adequately compare different types of PF-DES, compare PF-DES versus BP-DES, and analyse the sub-groups of diabetics and non-diabetics. The findings from this meta-analysis is consistent with the current literature; however, ours is different then the current studies in the literature as it evaluates all-cause mortality based on the type of drug-eluting stent’s polymer-coating [27].
In patients who are receiving PCI with DES, the current data indicates that PF-DES has significantly favorable outcomes in all-cause mortality as compared to PC-DES in the short-term follow-up. This believed to be due to the fact that PF-DES are resorbed but PP-DES are permanently present. Further studies with longer follow-up periods and different types of PF-DES are required to confirm and expand on these results. Trials should also be conducted to compare PF-DES versus BP-DES and to compare the specific drug components of the PF-DES.
None
The authors report no relationships that could be construed as a conflict of interest.
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
