
Research Article | DOI: https://doi.org/10.31579/2639-4162/146
1Department of Pharmacy, College of Pharmaceutical Sciences, National Yang Ming Chiao Tung University(Yang Ming Campus),Taipei, Taiwan.
2Department of Pharmacy, Chia Nan University of Pharmacy& Science, Tainan, Taiwan.
3Department of Pharmacy, Koo Foundation Sun Yat-Sen Cancer Center, Taipei, Taiwan.
*Corresponding Author: Shao-Chin Chiang, Mailing Address: No. 155, Sec. 2, Linong St., Beitou Dist., Taipei City 112304, Taiwan.
Citation: Yi-Y. Chen, Winnie Khor, Pei-L. Cheng, Shao-C. Chiang, (2024), Comparing Drug Handling Efficiencies and Expenses for Short-Acting Granulocyte-Colony Stimulating Factor Injection Originators and Biosimilars from the Perspective of Hospital Resource Management in Formulary Decision-Making, J. General Medicine and Clinical Practice, 7(2); DOI:10.31579/2639-4162/146
Copyright: © 2024, Shao-Chin Chiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 February 2024 | Accepted: 16 February 2024 | Published: 23 February 2024
Keywords: filgrastim; filgrastim biosimilar; granulocyte-colony stimulating factor; hospital resource management;
Background/Aim: With the availability of biosimilars, hospital formulary drug selection among biologics extends beyond clinical and safety considerations when comes to hospital resource management, to factors like human resource allocation and financial sustainability. However, research assessing the time and cost of labor, supplies, and waste disposal of biologics from the standpoint of hospitals remains limited. This study focuses on short-acting granulocyte-colony stimulating factor originators (Granocyte® and Neupogen®) and biosimilar (Nivestim®), comparing them based on mean total handling times per dose and total annual expenses.
Materials and Methods: Ten nursesfrom a Taiwanese cancer centerwere recruited; they each prepared three doses of each drug.
Results: Findings showedthat the mean total handlingtimes per dose of Granocyte® and Neupogen® were significantly higherthan that of Nivestim®. Handling Nivestim® required the lowest total annual expense.
Conclusion: Nivestim® is an advantageous alternative to Granocyte® and Neupogen®, benefiting hospital resource management.
When comes to drug selection in the contextof resource management within healthcare organizations, factors beyond clinical efficacyand safety should be taken into consideration, as decision-making. for formularies impacts theallocation of human resources, use of pharmaceuticals, and overall financial sustainability of the healthcare facility [1]. When chemical or biologic originators were initially the exclusively available products on the market, health providers were constrained to procure them owing to their patented market [2, 3]. However, the market competition has since evolved with the introduction of generics and biosimilars [4]. Notably, biologicsare delivereas injections or infusions [5], thus requiring special handling, specificstorage conditions, ancillary supplies, and careful waste management strategies. In response to these needs, manufacturers of biosimilar drugsadd other values to their products, like offering greater consumer convenience by packaging with prefilledsyringes and providingformulations with extendedbeyond- use dates [6, 7]. In light of this, healthcare providers are now faced with a choice not previously available – selecting among originators and biosimilars – in their pursuit for sustainable
One such example is granulocyte-colony stimulating factors (G-CSFs),a biologic that stimulates neutrophil production in the bone marrow to intervene chemotherapy induced myelosuppression[8-10].In Taiwan,several originators and biosimilar G-CSFshave been developed and approved for clinicalapplication (Table 1)[11-17]. Theycan be categorized into short-and long-acting types; the former includes Granocyte® (lenograstim),Neupogen®, also known as 惠爾血添® in Taiwan (filgrastim),and Nivestim® (filgrastim biosimilar),while the latter includes Neulasta® (pegfilgrastim), Ziextenzo® (pegfilgrastim biosimilar), Fulphila® (pegfilgrastim biosimilar),and Lonquex® (lipegfilgrastim)[18].Short-and long-acting G-CSFs serve different therapeutic roles[19].Short-acting G- CSFis administered for the treatmentand prophylaxis of neutropenia or febrile neutropenia. By contrast, long-acting G-CSF is administered once per chemotherapy cycle for prophylaxis [20].

Table 1: Taiwan Food and Drug Administration- (TFDA-) approved G-CSF (updated as of December 29th, 2023)
Focusing on short-acting G-CSFs,Nivestim® is a biosimilar of Neupogen® that comes in convenient, prefilled syringes [13].This contrasts with the originators,Granocyte® and Neupogen®, which are packaged into vials of dry powderand solution, respectively,making Nivestim® a potentially moreattractive option in termsof expediting the administration process [21]. With ever increasing demands on medical resources, assessing the time and cost of labor, supplies, and waste disposal associated with biologics is critical in deciding between originators and more affordable biosimilars.This study aims to compare these three drugs,namely the two originator(Granocyte® and Neupogen®) and one biosimilar (Nivestim®), based on their mean total handling times per dose and total annual expenses at a local, independent cancer center in Taiwan.
Study design and participants
This study was conducted at the Koo Foundation Sun Yat-Sen Cancer Center in Taipei, Taiwan. Ten nurses from the Department of Nursing were recruited into the study. Each nurse was responsible for handling three doses of each short-acting G-CSF product: Granocyte® (250 μg/vial), Neupogen® (150 μg/0.6 mL/ampoule), and Nivestim® (120 μg/0.2 mL/syringe). The nurses adhered to the standardized drug handling protocol (Appendix A). All the necessary ancillary supplies, namely alcohol swabs, syringes, needles, and artificial skin, were provided (Appendix B).
Drug handling time
The nurses prepared each of the three short-acting G-CSFs three times. They were video-recorded while following the drug handling protocols (Appendix A). Subsequently, one researcher documented the time (in seconds) spent by the nurses on each step of the protocols. The “mean handling time per step” for each nurse was derived from the three separate attempts. Those means were then summed to yield the “mean total handling time per dose” by each nurse, which was tested for statistically significant differences among Granocyte®, Neupogen®, and Nivestim®. Additionally, the “median handling times per step” across the 10 nurses were computed and summed to obtain the “median total handling time per dose”; this value was then utilized in the calculation of the labor cost for each product, as detailed in the next section. The time needed for the refrigerated drug ampoule or syringe to reach room temperature was not considered in our study.
Cost of handling G-CSF in a healthcare setting
The total annual expense for handling a G-CSF product in a healthcare setting was broken down into three components: cost of labor, medical supplies, and waste disposal in New Taiwan Dollars (NT$). Firstly, labor cost was determined based on each medication’s median total handling time per dose, as described in the previous section, and the nurses’ average hourly wage in 2022 (NT$ 271/hour) [22]. Secondly, the cost of medical supplies encompassed alcohol swabs, syringes, and needles, and it was computed using unit prices provided by medical suppliers. Third, waste disposal fees were calculated based on the total weight of the products themselves, vials, alcohol swabs, syringes, and needles, which followed the established pricing method. The sum of labor cost, medical supplies, and waste disposal yielded the total expense per dose. And to compare the expenses on a yearly basis, the total annual expense for each G-CSF product was calculated based on the quantity of 10,000 doses.
Statistical analysis
The Friedman test was used to determine if there were overall significant differences in the average drug handling times among the three drugs: two originators (Granocyte® and Neupogen®) and one biosimilar (Nivestim®). Subsequently, post hoc analysis via Wilcoxon signed-rank tests was performed with a Bonferroni correction applied to identify the pairs of drugs with statistically significant differences in drug handling times. A Bonferroni-adjusted significance level of p < 0>
Ten nurseswere recruited into this studyand were each tasked with handling three doses of three G-CSF products: Granocyte® (lenograstim), Neupogen® (filgrastim), and Nivestim® (filgrastim biosimilar). The “mean handling time per step” by each nurse (denoted by A to J) was measured (Appendix C). Across the threeprotocols, steps such as hand washing, drug inspection, reconstitution, and injection were the most time-consuming. Figure 1 illustrates the mean and median total handling times per dose for Granocyte®, Neupogen®, and Nivestim®. The median total handling time per dose for a single Nivestim® administration was 85 seconds, which was notably shorter than the times required for Granocyte® and Neupogen® administrations, measured at 242.5 and 120.5 seconds, respectively. The Friedman test demonstrated statistically highly significant differences in mean total handling time per dose among the three drugs (Friedman’s χ2 = 20.000, df = 2, p < 0 xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed>

Figure 1: Boxplot of mean total handling times per dose in seconds for Granocyte®, Neupogen®, and Nivestim®.The three boxplots illustrate the distribution of meantotal handling times per dose for Granocyte®(n=10), Neupogen® (n=10), and Nivestim®(n=10). The shaded box represents the interquartile range with the mean indicated by the “x” and the median indicated by the horizontal line within the box. The vertical lines extending from the box show the range from the minimum to the maximum values,excluding outliers.
The total expenses per dose of Granocyte®,Neupogen®,and Nivestim® were NT$ 23.66, NT$ 12.35, and NT$ 7.31, respectively (Table 2). Labor costs made up the largest portion of total expenses per dose for all three drugs,constituting 77%, 73%, and 88% of the cost for Granocyte®, Neupogen®, and Nivestim®, respectively (Figure 2). Nivestim®, the filgrastim biosimilar, incurredthe lowest labor and medicalsupply costs among the three drugs. Meanwhile, the cost for waste disposal was highest for Granocyte®, followed by Nivestim® and Neupogen®. When considering total annual expenses,Granocyte® was the highest (NT$ 236,563), followed by Neupogen® (NT$123,502) and Nivestim® (NT$ 73,128).
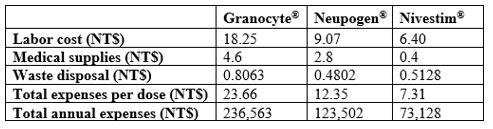
Table 2. Cost breakdownfor handling short-acting G-CSFs in a healthcare setting
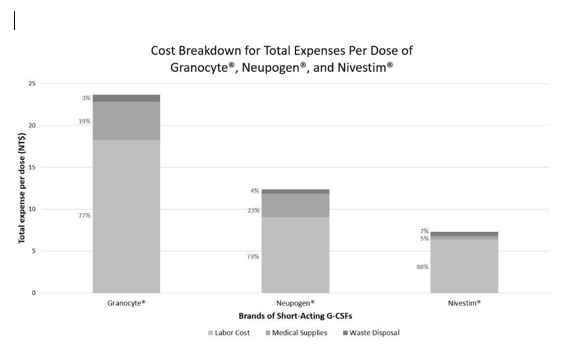
Figure 2: Cost breakdown for total expenses per dose. Stacked bar chart visualizing the total expenses per dose of Granite®, Neupogen®, and Nive stim® in a healthcare setting, broken down into three components: labor cost, medical supplies, and waste disposal. Labor cost was determined based on nurses’ average hourly wage of NT$ 271/hour and the median total handling time for each product. The proportions of each component for the three brands of drugs are expressed as percentages.
This is the first study to compare three short-acting G-CSF products in terms of their handling times and expenses. Nivestim® required a statistically significantly shorter mean total handling time per dose and the lowest total annual expense compared with Granocyte® and Neupogen®. The cost effectiveness of Nivestim® may be attributed to its ready-to-use packaging, eliminating the need for ancillary supplies and lowering the spending on waste disposal. In addition, the pre-filled syringes of Nivestim® streamline its drug handlingprotocol, thereby reducinglabor cost.Notably,air bubbles may become trapped in syringes when products are drawn from vials or ampoules, as is the case with Granocyte® and Neupogen®, and those bubbles need to be expelledto ensure accuratedosing and patientsafety [23].However, small quantity of bubbles can often be disregarded in manufacturer-prefilled syringes, as is the case with Nivestim®, thereby expediting the preparation process[24]. Aside from differences in labor requirements, the three short-acting G-CSFs vary in storage requirements. As with most protein-based therapeutics, optimal storage conditions are vital for maintaining the stability and shelf- life of G-CSFs,as they are susceptible to denaturation and degradation when exposed to environmental stressors like temperature extremes, light, or pH changes [25].Whereas Granocyte® can be storedat room temperature for 30 months [11],Neupogen® and Nivestim® require refrigeration and can be stored for 36 and 30 months, respectively[12,13].Based on manufacturers’ instructions, however,Neupogen® and Nivestim® can remain stableat room temperature for up to 24 hours post-refrigeration [12, 13], a step that would not have impacted the nurses’ drug handling efficiency. Therefore, the present study did not factor the time needed to bring Neupogen® and Nivestim® to room temperature into the analysisof total drug handling time.Beyond lowering expenses and workforce demands within individual medical facilities, the adoption of biosimilars also has significant implications for public health. Recent expert reports from high-income countries highlight that nearly all stakeholders in healthcare can benefit from biosimilars [26], as they provide more treatment options for the growing aging population and foster market competition to make products more affordable [27-29]. According to the United States Food and Drug Administration, developing biosimilars can take from 8 to 10 years,incurring between USD $100 and 200 million, whereasan estimated USD $2.6 billion would be required for the development of a novel drug [30, 31].Having a broader array of treatment options for a particular disease or condition also incentivizes manufacturers to adjust pricingto sustain or expand their market share [32]. Moreover, biosimilars may even introduce competition that pressures reference products to drop in prices, leading to greater reductions in healthcare spendings [33].
This study is subject to certain limitations. One potential concern is the relatively small sample size, which consists ten nurses from a single healthcare center in Taipei, Taiwan who are tasked with handling each product three separate times. The single-center design may also affect the external validity of the findings. Nonetheless, given that the nurses have all undergone proper training and followed the standard operation procedure provided by the Principal Investigator, increasing the numberof participants would likelyhave limited impacton our results. The secondlimitation is that our study focuses on three short-acting G-CSF products currently approved for clinical use in Taiwan. As a result,the findings may not be generalizable across other countries, where variations in dosage forms and healthcare practices can influence drug handling times and expenses. With that considered, caution should be exercised when extrapolating the findings to diverse healthcare settings and healthcare systems outside of Taiwan. Nevertheless, our study contributes novel perspectives on formulary decision-making in the context of hospital resource management.
The present study demonstrates that the short-acting G-CSF biosimilar, Nivestim®, is an advantageous alternative to the short-acting G-CSF originators,Granocyte® and Neupogen®,significantly reducing both time and expenses spent on the drug handling process.Given the growingcancer patient population and finite medical resources,the practical and financial benefits of biosimilars signal an opportunity for local healthcare facilities to re-strategize their formulary decision-making to optimize resource management.
Acknowledgments
The authors would like to acknowledge the Koo Foundation Sun Yat-Sen Cancer Center in Taipei, Taiwan for providing the study site and medical supplies, as well as the Chia Nan University of Pharmacy and Science for their generous contribution.
Author Contributions
Yi-Ying Chen: formal analysis; writing – original draft; writing – review and editing; visualization.
Winnie Khor: formal analysis; writing – original draft.
Pei-Ling Cheng: conceptualization; data curation.
Shao-Chin Chiang: conceptualization; methodology; writing – review and editing; supervision.
Conflicts of Interest
All authors declare no conflicts of interest.
Data Availability Statement
The data supporting the findings of this study are available within the article’s supplementary materials.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
