
Review Article | DOI: https://doi.org/10.31579/2578-8965/175
1 Department of Obstetrics and Gynecology, Northwestern University, Feinberg School of Medicine, Chicago, IL
2 Department of Obstetrics and Gynecology, Rush University, Chicago, IL
*Corresponding Author: Nisha Garg, Department of Obstetrics and Gynecology, Northwestern University, Feinberg School of Medicine, Chicago, IL.
Citation: Nisha Garg, Kayla Nixon, Susan Tsai, Linda Yang, Angela Chaudhari, (2024), Comparing Complications Between Mini-Laparotomy and Laparoscopy for Benign Hysterectomy – A Systematic Review, J. Obstetrics Gynecology and Reproductive Sciences, 8(2) DOI:10.31579/2578-8965/175
Copyright: © 2024, Nisha Garg. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 July 2023 | Accepted: 17 August 2023 | Published: 15 February 2024
Keywords: IUCD; fragmented IUCD; malpositioned IUCD; misplaced IUCD; uterine perforation
Objective: To perform a comprehensive systematic review comparing complications between mini-laparotomy hysterectomy (MLH) and laparoscopic hysterectomy (LH).
Methods: A systematic review of MEDLINE, Clinicaltrials.gov, Embase, Cochrane Library, and Scopus was conducted. Out of 641 initially identified studies, 8 were ultimately included. The primary outcomes were operative time, time to discharge, need for blood transfusion, superficial and deep wound complications, post-operative fever, reoperation, readmission, and conversion to laparotomy. A meta-analysis was performed for each outcome, including measures of heterogeneity among studies.
Results: There was a significant difference between mean operative time for MLH (121.6 min) and LH (127.51 minutes). There was no significant difference between time to discharge [ MLH (79.21 hours) vs LH (73.21 hours)], need for blood transfusion [MLH (.03) vs. LH (.01)], superficial wound complications [MLH (.01) vs LH (0)], deep wound complications [MLH (0) vs LH (.01)], post-operative fever [MLH (.02) vs LH (.01)] or reoperation [MLH (.01) and LH (0)]. There was not a significant difference in readmission [MLH (.02) vs LH (.01)], or conversion to laparotomy [ MLH (.01) vs LH (.01)]. There was significant heterogeneity among studies in one or both groups for: operative time, time to discharge, need for blood transfusion, and conversion to laparotomy.
Conclusion: In this systematic review comparing complications between MLH and LH, there was significant heterogeneity amongst studies, making it challenging to interpret definitively. Even the definition and technique for performing mini-laparotomy was not well defined. There was an overall trend towards similar rates of complications. Though there was a statistically significant difference in operative time, the mean difference of 6 minutes is clinically unimportant.
Hysterectomy is one of the most frequently performed gynecologic surgeries performed in the U.S. Compared with the traditional abdominal hysterectomy (AH), minimally invasive techniques such as vaginal, laparoscopic, robotic, and mini-laparotomy approaches have been shown to have shorter hospital stays and a quicker recovery [1]. These are important considerations for providers, patients, insurers, and hospitals. Studies have shown that laparoscopic hysterectomy (LH) results in less post-operative pain and shorter hospital stay than AH. However, they also have reportedly longer operative times [2]. Other factors including surgical experience, learning curve, and cost of setup and operating room time may limit the ability to make LH standard of care [3].
Mini-laparotomy has long been in use by general surgeons as a minimally invasive approach. It was first described in gynecologic surgery in 1996 [4]. Mini-laparotomy has since been considered a feasible alternative but with potentially less limitations than laparoscopy, given the ability to use conventional instruments including needle drivers, suture, cell saver, and make use of manual manipulation and dissection [1]. More recently, mini-laparotomy hysterectomy (MLH) has been proposed as an alternative approach that is less invasive than TAH [2]. Previous studies have investigated outcomes after mini-laparotomy myomectomy compared to laparoscopic myomectomy, however the results were variable and with multiple confounding factors [2]. Given the growing interest in determining the optimal route of minimally invasive hysterectomy, there is great interest in evaluating outcomes after MLH.
The objective of this study was to perform a comprehensive systematic review comparing complications and clinical outcomes between mini-laparotomy hysterectomy and laparoscopic hysterectomy.
A systematic review of MEDLINE, Clinicaltrials.gov, Embase, Cochrane Library, and Scopus was conducted. A librarian (M.B.) collaboratively developed the search strategies with the other authors (N.G., K.N.) and ran the searches in the following databases: MEDLINE (PubMed), clinicaltrials.gov, Embase (Elsevier), Cochrane Library (Wiley), and Scopus (Elsevier). The search strategies for all databases were adapted from the MEDLINE search strategy. All databases were searched back to inception with no date limits. We included any studies available in English, and we excluded case reports and case series. Searching for eligible studies to include in the review involved the following approaches: controlled vocabulary (MeSH headings and thesauri of relevant databases) and the keywords of gynecologic surgery, benign or non-neoplastic, mini-laparotomy, and laparoscopy. We also attempted to discover additional studies by searching the reference lists of key studies and relevant systematic reviews. The search was completed in December 2020. The search strategy followed all PRISMA guidelines (Figure 1),

Figure 1: PRISMA flow diagram of manuscripts identified
and the study was registered with the PROSPERO international database of systematic reviews.
The PubMed Search Strategy included terms ("gynecologic surgical procedures"[MeSH Terms] OR ("gynecologic" AND "surgical" AND "procedures") OR "gynecologic surgical procedures" OR "gynecologic surgery" OR "gynecologic surgeries" OR "gynecological surgery" OR "gynecological surgeries" OR oophorectom* OR "Salpingectomy"[Mesh] OR salpingectom* OR salpingo-oophorectom* OR Salpingo-oophorectomy[Mesh] OR ovariectom* OR Ovariectomy[Mesh] OR "Uterine Myomectomy"[Mesh] OR myomectomy OR myomectomies OR hysterectomy OR hysterectomies OR fibroidectomy OR fibroidectomies) OR (("adnex" OR "adnexal" OR " adnexes" OR "Adnexal diseases" OR "Adnexal diseases"[Mesh] OR "adnexal disease" OR "fallopian tube diseases" OR "fallopian tube disease" OR "Ovarian diseases" OR "ovarian disease" OR "ovarian cysts" OR "ovarian cyst" OR "adnexal cyst" OR "adnexal cysts" OR "adnexal mass" OR "pelvic mass" OR fibroids OR myoma[MeSH] OR myoma* OR leiomyoma[MeSH] OR leiomyoma* OR endometriosis[MeSH] OR endometriosis OR "adnexal cyst" OR "adnexal cysts" OR "pelvic pain" OR "endometriotic lesions" OR "endometriotic lesion") AND ("surgery"[MeSH Subheading] OR "surgery" OR "surgeries" OR "surgical" OR "surgical procedures, operative"[MeSH Terms] OR "operative surgical procedures" OR "general surgery"[MeSH Terms] OR "general surgery")) AND (mini laparotomy[All Fields] OR "mini laparotomies"[All Fields] OR "mini laparotom*"[All Fields] OR "minilaparotomies"[All Fields] OR minilaparotomy"[All Fields] OR "minilaparotomies"[All Fields] OR "minilaparotomy"[All Fields] OR minilap OR mini-lap) AND (Laparoscopy[Mesh] OR laparoscop* OR "robot assisted" OR "robotic assisted" OR "robotic surgery") N=336
The initial search strategy broadly targeted mini-laparotomy versus laparoscopy for all benign gynecologic surgeries. Six hundred forty-one studies were identified. All reports were screened by two independent reviewers (N.G. and K.N.). After removing all duplicates, 373 abstracts remained for screening. Of these, 103 full texts were retrieved and screened. Authors (N.G. and M.M.) then assessed the reports and narrowed the focus to a single surgical procedure (hysterectomy) to reduce heterogeneity. Ultimately, 8 studies were included in this systematic review1-3, 5-9. Data was then extracted by two independent authors (N.G. and M. M.) and cross-referenced to ensure accuracy. The primary outcomes were operative time, time to discharge, need for blood transfusion, superficial wound infection, deep wound infection, post-operative fever, need for reoperation, and conversion to laparotomy.
For studies that reported means and standard deviations, a mixed effects meta-analysis of the means was used to compute the overall mean effect for each continuous outcome. A mixed effects meta-analysis of proportions was utilized to compute an overall proportion of the binary outcomes. Cochrane’s Q test, τ2, and I2 were the measures of heterogeneity that were computed and reported for each meta-analysis. To compare MLH and LH, two sample t-tests and Fisher’s Exact tests were used for each outcome.
Out of the 8 studies included in the review, 2 were prospective studies, 5 were retrospective studies, and 1 was a randomized control trial. The studies spanned 6 different countries and the data was collected between 2004-2016. All papers included both MLH and LH. One study included Robotic LH and supracervical hysterectomy, which we excluded from the analysis. Four of the studies included laparoscopic-assisted vaginal hysterectomy (LAVH).
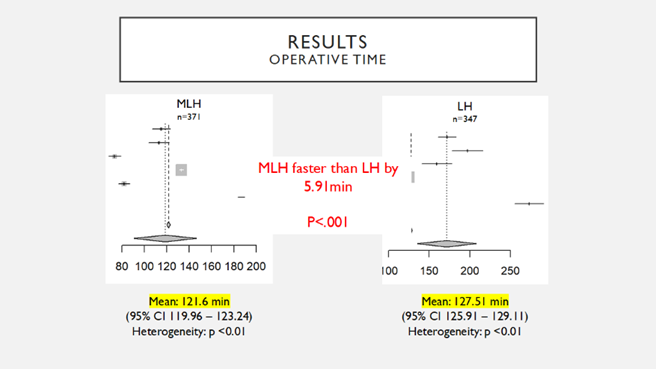
Six studies reported operative times between MLH and LH. The mean operative time for MLH was 121.6 minutes (95% CI 119.96 – 123.24), however there was statistically significant heterogeneity in reported operative times between studies (p less than 0.01, I2 = 99%). The mean operative time for LH was 127.51 minutes (95% CI 125.91 – 129.11), however, again, this was statistically significant between studies (p less than0.01, I2 = 99%). Comparing operative times, MLH was found to be statistically faster compared to LH (Figure 2).
(a)
(b)
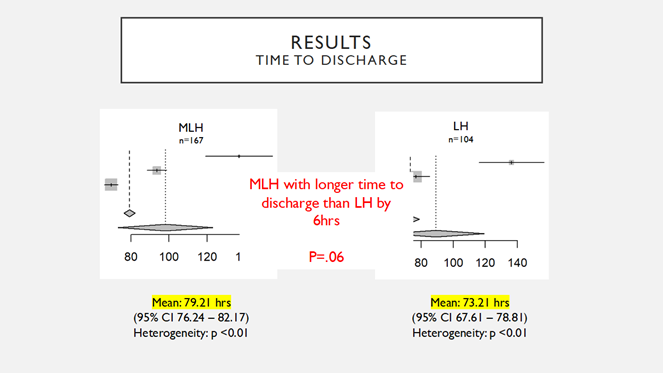
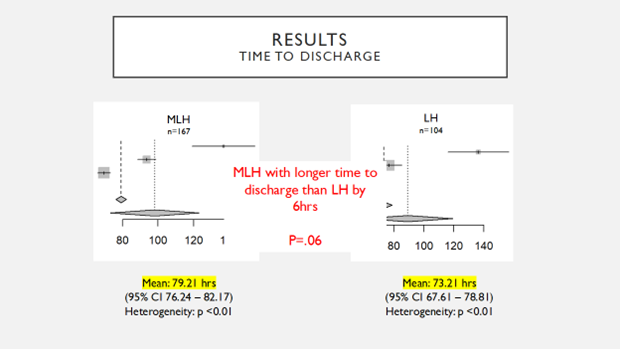
Figure 2: Results comparing operative time (a) and time to discharge (b) of Mini-laparotomy (MLH) and Laparoscopic hysterectomy (LH)
Three studies reported time to discharge between MLH and LH. The mean time to discharge for MLH was 79.21 hours (95% CI 76.24 – 82.17), however there was statistically significant heterogeneity in reported time to discharge between studies (p less than0.01, I2 = 98%). The mean time to discharge for LH was 73.21 hours (95% CI 67.61 – 78.81), however again there was statistically significant heterogeneity between studies (p less than0.01, I2 = 96%). Comparing time to discharge, MLH was found to be equivalent to LH (Figure 2).
Five studies reported on the need for blood transfusion between MLH and LH. The proportion of patients who required blood transfusion for MLH was .03 (95% CI .01 - .05), however there was statistically significant heterogeneity between studies (p less than0.01, I2 = 76%). The proportion of patients who required blood transfusion for LH was .01 (95% CI 0 – .03), and there was no statistically significant heterogeneity between studies (p =0.63, I2 = 0%). Comparing need for blood transfusion, MLH was found to be equivalent to LH (Figure 3).
(a)
(b)
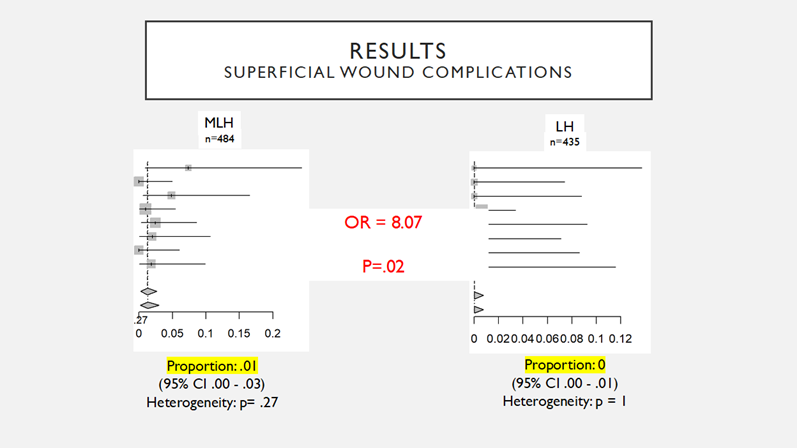
Figure 3: Results comparing blood transfusion (a) and superficial wound complications (b) of Mini-laparotomy (MLH) and Laparoscopic hysterectomy (LH)
All 8 studies reported on the number of superficial wound complications between MLH and LH. The proportion of patients who had a superficial wound complication for MLH was .01 (95% CI 0 - .03), and there was no statistically significant heterogeneity between studies (p =0.27, I2 = 20%). The proportion of patients who had a superficial wound complication for LH was 0 (95% CI 0 – .01), and there was no statistically significant heterogeneity between studies (p =1, I2 = 0%). Comparing the proportion of superficial wound complications, MLH was found to be equivalent to LH (Figure 3).
Four studies reported on the number of deep wound complications between MLH and LH. The proportion of patients who had a deep wound complication for MLH was 0 (95% CI 0 - .02), and there was no statistically significant heterogeneity between studies (p=0.62, I2 = 0%). The proportion of patients who had a deep wound complication for LH was .01 (95% CI 0 – .02), and there was no statistically significant heterogeneity between studies (p =0.25, I2 = 28%). Comparing deep wound complications, MLH was found to be equivalent to LH (figure 4).

(a)
(b)
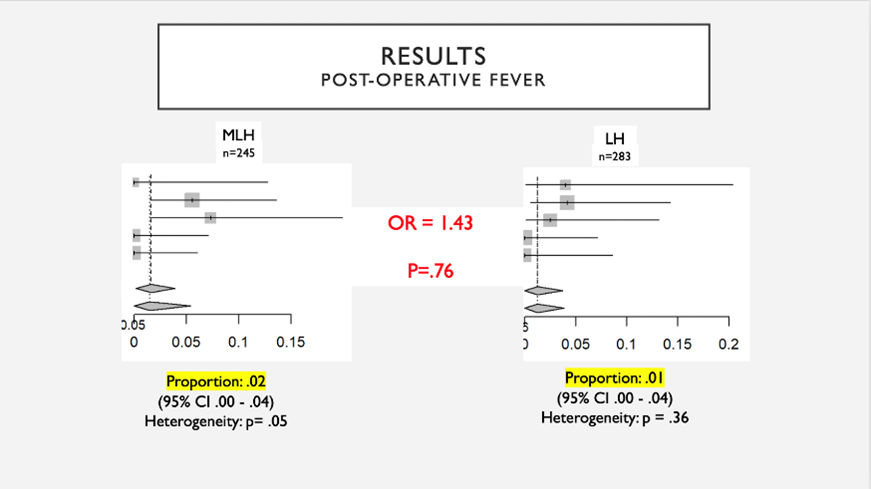
Figure 4: Results comparing deep wound complications (a) and postoperative fever (b) of Mini-laparotomy (MLH) and Laparoscopic Hysterectomy (LH)
Five studies reported on post-operative fever between MLH and LH. The proportion of patients who had a on post-operative fever for MLH was .02 (95% CI .00 - .04), and there was no statistically significant heterogeneity between studies (p=.05, I2 = 58%). The proportion of patients who had a on post-operative fever for LH was .01 (95% CI 0 – .04), and there was no statistically significant heterogeneity between studies (p =.36, I2 = 8%). Comparing postoperative fever, MLH was found to be equivalent to LH (Figure 4).
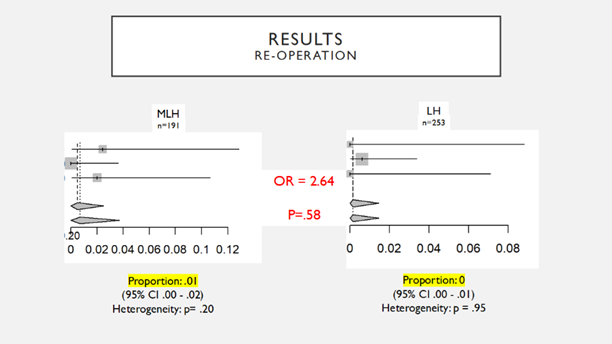
Three studies reported on the need for reoperation between MLH and LH. The proportion of patients who had a need for reoperation for MLH was .01 (95% CI .00 - .02), and there was no statistically significant heterogeneity between studies (p=.2, I2 = 37%). The proportion of patients who had a need for reoperation for LH was 0 (95% CI 0 – .01), and there was no statistically significant heterogeneity between studies (p =.95, I2 = 0%). Comparing reoperation, MLH was found to be equivalent to LH (Figure 5).
(a)
(b)
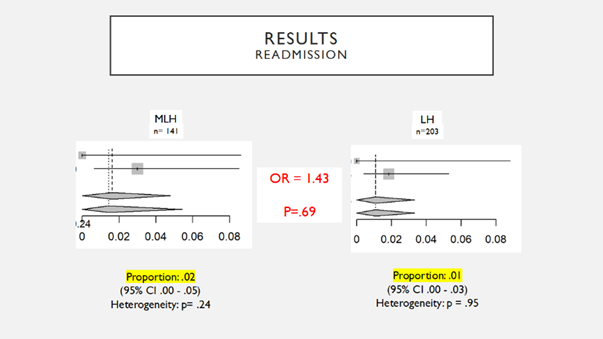
Figure 5: Results comparing reoperation (a) and readmission (b) of Mini-laparotomy (MLH) and Laparoscopic hysterectomy (LH)
Two studies reported on the need for readmission between MLH and LH. The proportion of patients who had a need for readmission for MLH was .02 (95% CI .00 - .05), and there was no statistically significant heterogeneity between studies (p=.24, I2 = 29%). The proportion of patients who had a need for readmission for LH was .01 (95% CI 0 – .03), and there was no statistically significant heterogeneity between studies (p =.4, I2 = 0%). Comparing readmission, MLH was found to be equivalent to LH (Figure 5).
Six studies reported on the need for conversion to laparotomy between MLH and LH. The proportion of patients who had a conversion to laparotomy for MLH was .01 (95% CI .00 - .03), however, there was a statistically significant heterogeneity between studies (pless than.01, I2 = 74%). The proportion of patients who had a conversion to laparotomy for LH was .01 (95% CI 0 – .02), and there was no statistically significant heterogeneity between studies (p =.16, I2 = 37%). Comparing conversion to laparotomy, MLH was found to be equivalent to LH (Figure 6).
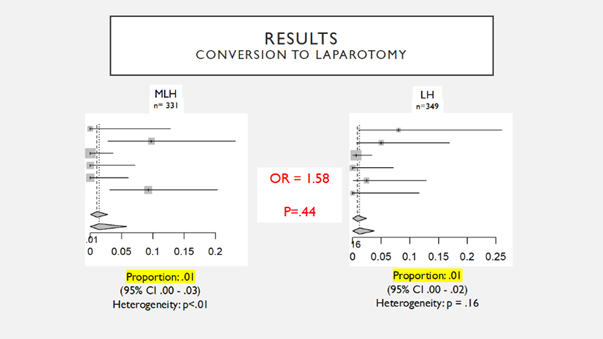
Figure 6: Results comparing conversion to laparotomy between Mini-laparotomy (MLH) and Laparoscopic hysterectomy (LH)
Superficial wound infection occurred more frequently in MLH compared LH (OR = 8.07). Additionally, operative time was 5.91 minutes longer in MLH.
In this systematic review, the existing literature was used to compare complications and clinical outcomes between MLH and LH. Overall, there appears to be a trend towards similar outcomes between MLH and LH, except for an increased odds of superficial wound infection with MLH, and a slight increase in operative time with MLH, though this difference of six minutes is likely clinically unimportant.
There was significant heterogeneity among the studies for many of the outcomes. This makes interpretation of the data challenging and brings into question the consistency of the results. An important confounder is that there was variation in the definition and technique of mini-laparotomy that was used in each study. The skin incision varied from 4-9cm, and the fascial incision lengths went as high as 12 cm. Some studies also included vertical fascial or skin incisions in their MLH groups. These variations can have a potentially significant impact on the results. Another important point is that much of it was collected from patients who underwent surgery prior to the FDA ban on power morcellators. Since then, large specimen tissue extraction in laparoscopic hysterectomy has changed to involve hand morcellation either vaginally or through a “mini-lap” extension of a port site. This change in practice could have important impacts on the true operative times and odds of wound infections. Future studies should consider including further subset analysis based on mini-laparotomy incision length, uterine weights, and data pre- and post- morcellator ban. Additionally, studies performing similar analyses for other gynecologic surgeries such as myomectomy or cystectomy would also be informative.
In summary, complications of mini-laparotomy were comparable to laparoscopic hysterectomy although there was significant heterogeneity amongst studies.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
