
Research Article | DOI: https://doi.org/10.31579/2578-8965/127
Department of Obstetrics & Gynecology, Faculty of Medicine, Benha University, Benha. Egypt.
*Corresponding Author: Ali A. Bendary. Department of Obstetrics & Gynecology, Faculty of Medicine, Benha University, Benha. Egypt.
Citation: Ali A. Bendary, Waleed M.Tawfik. (2022). Comparative Study between Different Methods of Laparoscopic Hysterectomies, J. Obstetrics Gynecology and Reproductive Sciences. 6(5) DOI: 10.31579/2578-8965/127.
Copyright: © 2022 Ali A. Bendary. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 June 2022 | Accepted: 15 June 2022 | Published: 05 July 2022
Keywords: laparoscopic-assisted vaginal hysterectomy (LAVH); total laparoscopic hysterectomy (TLH); hysterectomy
Background: Hysterectomy is the second most common major surgical procedure performed on women after caesarean section. The incidence of hysterectomy is 4-6% out of which 90% are performed for benign indications.
Aim of the work: The aim of this study was to compare intra- and post-operative morbidity associated with two types of laparoscopic hysterectomy. Laparoscopic-Assisted Vaginal Hysterectomy (LAVH) and Total Laparoscopic Hysterectomy (TLH)
Patients and methods: A total of 80 women scheduled to undergo a hysterectomy for benign disease were subdivided into 2 groups; 40 women for LAVH and 40 women for TLH, Patients were excluded from the study if they had contraindication to laparoscopy. Intra- and post-operative evaluations including the duration of the operation uterine weight, frequency of intraoperative complication, and the difference between hemoglobin level prior to surgery and one day after surgery.
Results: LAVH took the longest operating time. As regard hemoglobin deficit that occurred after 24 hours of surgery, our study showed that TLH had largest Hb deficit (1.6 gm/dl) but still the Hb deficit not significantly different. As regard transfusion of blood, one case took blood in group LAVH and one case in group TLH. As regard other complications, the bladder was injured during plunt dissection of the bladder flap in group TLH and this case was having history of one cesarean section 10 years ago.
Conclusion: laparoscopic assisted vaginal hysterectomy showed lower complication but longer operative time than total laparoscopic hysterectomy group; also (LAVH) showed shorter hospital stay and need fewer analgesics so we considered this method the best when the patient accepted total removal of the uterus. While total laparoscopic hysterectomy showed the more blood loss and complication intraoperatively and postoperatiovely, but this complication is non-significant in cases of removal of the hole uterus.
Hysterectomy is the second most common major surgical procedure performed on women after caesarean section. In India, the incidence of hysterectomy is 4-6% out of which 90% are performed for benign indications [1].
While, the incidence of hysterectomy in the Western countries is 10-20% with the highest rate in the United States and the lowest in Norway and Sweden. There are various possible approaches to hysterectomy for benign disease of uterus; Abdominal Hysterectomy (AH), Vaginal Hysterectomy (VH) and Laparoscopic Hysterectomy (LH). Laparoscopic approach may be used either to facilitate the ease of vaginal delivery of uterus as in Laparoscopy Assisted Vaginal Hysterectomy (LAVH) or it may be carried out completely till final detachment of uterus from pelvic wall i.e. Total Laparoscopic Hysterectomy (TLH). Although Laparoscopic Hysterectomy (LH) takes longer time, its proponents have emphasized several advantages over abdominal hysterectomy in terms of intraoperative blood loss, less postoperative morbidity, rapid recovery time, shorter hospital stay, fewer febrile episodes and early return to normal activities[2].
Traditionally, abdominal hysterectomy has been used for gynaecological malignancy-when other pelvic disease is present, such as endometriosis or adhesions-or if the uterus is enlarged. It remains the "fallback option" if the uterus cannot be removed by another approach [3].
Vaginal hysterectomy was originally used only for prolapse, but it is now also used for menstrual abnormalities when the uterus is of fairly normal size. Vaginal hysterectomy is regarded as less invasive than abdominal hysterectomy [4].
In 1989, Reich et al. first reported a new procedure called laparoscopically assisted vaginal hysterectomy. Since then, laparoscopic hysterectomy has gained widespread popularity and subtotal and total laparoscopic hysterectomy became a standard of care for treating benign uterine pathology in many centers worldwide [2].
Laparoscopic hysterectomy requires greater surgical experience than abdominal and vaginal methods, the proportion of hysterectomies performed laparoscopically has gradually increased in the last decades. As experience is gained during the learning curve, the operation time, complication rate and hospital stay are decreased [5].
Laparoscopic-assisted vaginal hysterectomy provide minimally invasive way to accomplish a hysterectomy with decreasing length of accomplish a hysterectomy with decreasing length of hospital stay and time of return to normal activity [6].
To compare 2 types of laparoscopic hysterectomies including Laparoscopic-Assisted Vaginal Hysterectomy (LAVH) and Total Laparoscopic Hysterectomy (TLH) as regard demographic data, indications, weight of removed uteri, operative time, intra-operative blood loss, intra- and post-operative complications, need for analgesics and hospital stay.
This was prospective randomized study carried out in Obstetrics and Gynecology Department, between March 2021 to May 2022, all patients are recruited from Gynecological Outpatient Clinic.
In this study, 80 patients were divided into 2 groups:
Group A: 40 patients underwent laparoscopically assisted vaginal hysterectomy (L.A.V.H.).
Group B: 40 patients underwent total laparoscopic hysterectomy (T.L.H.).
Patient selection:
All patients scheduled to undergo a hysterectomy for benign uterine lesion such as:
*Leiomyoma.
*Endometrial hyperplasia.
*Dysfunctional uterine bleeding un-responding to medical treatment.
*Suspected adenomyosis.
The uterine size by examination and investigation was not more than sixteen weeks like gestation size.
Excluded patients from our study:
*Any suspected or confirmed malignancy in the uterus.
*Presence of any contraindication to laparoscopy.
*Any patients with uterine size > 16 weeks like gestation uterus.
All patients were subjected to:
* Full history taking.
* Complete examination
* Ultrasonographic evaluation.
* Laboratory investigation.
* Fractional curettage and histopathological assessment.
Preoperative preparation:
It is recommended that all patients eat lightly for 24 hours and be NPO at least 12 hours prior to surgery. A Fleet enema is helpful the night before laparoscopic surgery and an oral preparation using metronidazole and neomycin 3 days before surgery an empty bowel permits better visualization during surgery, and in the event of a bowel injury, decreases the possibility of complications. It should be carefully worded to explain expected postoperative discomfort and to differentiate it from severe pain that requires her to contact the surgeon with a telephone number that is answered 24 hours a day. Patients should be discharged with all the appropriate instructions and medication or a prescription for pain relief.24 hour after the surgery hemoglobin concentration is done to all patients and the hemoglobin deficit was calculated. Also, the operation time from skin incision to last suture is calculated accurately, the uterine weight, intraoperative and postoperative complications, need to analgesia and hospital stay.
Surgical technique: routine laparoscopic equipment that is essential for performing a successful laparoscopic hysterectomy includes:
* Standard laparoscopic tower containing a high-flow CO2 insufflator, camera and a light source.
* An operating table with leg stirrups and capability of placing the patient in steep Trendelenburg position is essential
* Some kind of bleeding control instrument such as, bipolar and unipolar electricity generator Ligasure vessel sealing instrument.
* A sturdy uterine mobilizer, capable of extreme anteversion and movement of the uterus in an arc of 45° to the right and left is important.
* We prefer the disposable scissors because reusable scissors are often not sharpened adequately for the extensive cutting involved in laparoscopic hysterectomy.
* Two good laparoscopic graspers with long jaws for grasping and manipulating the uterus, adnexal structures and bowel.
* Suction irrigator is essential to clear out the smoke if unipolar or bipolar energy is used and to remove the blood and blood clots.
Step 1: Trocar placement:
We routinely place a Veress needle in the lower edge of the umbilicus. We then insufflate to 20 mmHg prior to placement of any trocars. A 10- 12 mm trocar is then placed through a vertical intraumbilical incision for insertion of the telescope. tow additional 5 mm trocars are then placed into the peritoneal cavity. this pair were placed lateral to the inferior epigastric vessels approximately two fingerbreadths above the pubis. the third one was 12 mm and put in the suprapubic region. If a patient has had prior abdominal surgery, we will often place the 5 mm trocar first and then inspect the periumbilical area with a 5 mm laparoscope to evaluate adhesion of underlying omentum and bowel to the anterior abdominal wall. Whatever method is used for trocar insertion, it is crucial to use “backstop” measures to prevent rapid, uncontrolled thrusting of the trocar through the layers of the abdominal wall and into underlying structures and adhesions.
Step 2: Identification of the ureters:
The ureters should be identified prior to securing any supporting structures to the uterus. Knowledge of pelvic anatomy and the course of the ureter are crucial. In most cases the ureters are visible through the peritoneum. As long as the ureters are clearly identified through the peritoneum, it is reasonable not to dissect them when performing procedures such as a laparoscopic assisted vaginal hysterectomy.
Ligaments:
The round ligaments can easily be desiccated by using ligasure instrument. The uterus is deviated to the left by an assistant and a grasper is used to place the round ligament on traction. The round ligament is coagulated and cut in the middle of the ligament with the coagulating instrument introduced from the ipsilateral side.
Step 4: Securing infundibulopelvic and uterine-ovarian ligaments:
For women desiring removal of the ovaries, the suspensory ligament of the ovary (infundibulopelvic ligament). For women who want to preserve their ovaries, the uterine-ovarian ligaments and Fallopian tubes were sealed and cut medial to the ovary using ligasure atlas instrument 10 mm. but if we want to remove the ovaries, we cut the infundibelopelvic ligament itself being care of the course of the ureter.
Step 5: Creation of the bladder flap:
First, identify the vesico-uterine peritoneal fold. To facilitate identification of the vesico-uterine fold, have an assistant retrovert the uterus and push it cephalad. The upper junction of the vesico-uterine peritoneal fold is distinguished as a white line. Identification of the white line is important because, cephalad to the white line, the peritoneum is attached tightly to the uterus. Below this demarcation the peritoneum is loosely attached to the cervix and can be easily dissected away.
Using a grasper, place the vesicouterine fold on traction. Make a transverse incision just below the white line and dissect the bladder away from the lower uterine segment and cervix. In the right tissue plane, the dissection should be relatively bloodless. The middle band of loose connective tissue is the vesico-cervical ligament.
This ligament does not contain blood vessels and can be easily divided. laparoscopic scissors with electroenergy can be used to coagulate any small incidental bleeders during dissection. The lateral bands of connection on both sides of the cervix are bladder pillars. The bladder pillars contain blood vessels and should be desiccated prior to ligation. Dissection of the bladder laterally helps pull the ureters away from the cervix. To achieve this, incise the bladder peritoneum to the level of the round ligament. Continue dissection in the avascular plane and push the bladder caudad over the cervix to its junction with the anterior fornix of the vagina
Step 6: Securing the uterine arteries:
The broad ligaments on both sides are opened downward and towards the cervix, skeletonizing the uterine vessels. Once the uterine vessels are skeletonized they can be sealed laterally using ligasure atlas insteroment 10 mm, if necessary, to help control bleeding and identify the ureter when dealing with a large or cumbersome uterus. With meticulous dissection, the uterine vessels can be identified at the level of the ureteric canal as it crosses above the ureter. Knowledge of the course of the ureter is essential at this point to avoid injury. the uterine vessels can be secured medially as they enter the uterine body. The suction irrigator is used to push the body of the uterus to the opposite side
In cases of group (A)(L.A.VH.) After ligation of uterine artery, the laparoscopic approach is stopped and pneumoperitoneum is reversed, then the patient position is corrected into standard lithotomy position, then the cervix is grasped using vollessulume anteriorly and posteriorly. Using cold scalble or valley lap scalpel, we cut the vaginal mucosa surrounding the cervix, then the Mackenrodit ligment is grasped using 2 force grasspers and cutting is done between the 2 grasspers, then we transligate the attached end to the pelvic wall. This is done on each side. Vagina is closed and suspended to the makenrodet ligament. ligation was done using Vicryl 0 suture. In some cases, vaginal pack is left, then we change the position of the patient and laparoscopic underwater examination is done. The patient is instructed to be followed-up one week later and then after one month.
In cases of group (B)(T.L.H.) After dealing with the uterine artery, the manipulator is used to push the uterus to the left side during grasping and cutting the Machenrodit ligament on the right and vise verse this is don using ligasure instruments.
After that, we use the Vally laparoscopic hook or unipolar hook to open the vagina, we open the vagina anteriorly against the hard "ceramic" part in the manipulator and we move the ceramic part carefully to open the cuff laterally, then posteriorly. For fear of loss of pneumoperitoneum, we use a big sponge in plastic cover to pack the vagina tightly and surround the mobilizer. Then, we remove the uterus vaginally from the opening os.
We remove all the trocar under vision. CO2 was allowed to escape gradually, then remove the last trocar under vision. Also, lastly, we close the skin using non-absorbable silk suture which removed after 7 days.
After all methods the patients were followed up carefully for 24 hours and discharged if they were will to be examined after one week then after one month. Prior to discharge, each patient was evaluated and examined for vital signs and presence of any complications.
In the postoperative period we gave all patients analgesics in the form of diclofenac sodium 100 mg which is (NSAID) but if the patients are still complaining from pain, we gave here narcotic in the form of 100 mg pethidine single dose.
After 12 hour 1 gm cefotriaxon was given and before discharge we gave here instructions to take only semisolid food in the first day, diclofenac sodium tablet 50 mg if needed.
Statistical analysis: Data were entered checked and analyzed using EpiInfo version 6 and SPP for Windows version 8.
The mean age of group (A) was 44.7 years old with standard deviation of (SD) 2.4.The mean age of group (B) was 52 years old with SD 5.4
As regard the parity each group was subdivided into two groups, the first one who delivered less than 3 children and the 2nd group who delivered more than 3 children in group (A) 60% of its patients delivered less than three children and 40 (percentage) delivered more than 3 children. In group (B) 45 (percentage) delivered less than 3 children and 55 (percentage) delivered more than 3 children. As regarding BMI, In group (A) the mean of BMI was 24.7 kg/m2 with S.D. 2.7. In group (B) the mean of BMI was 24 kg/m2 with S.D. 3.2. The P. value in all demographic data was non-significant.
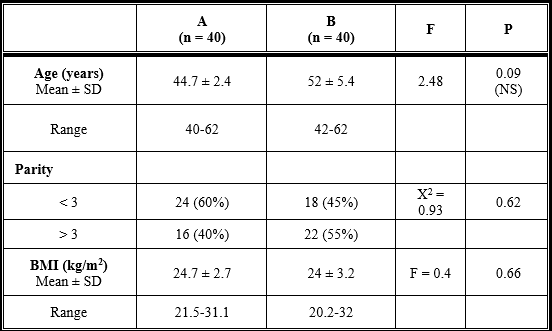
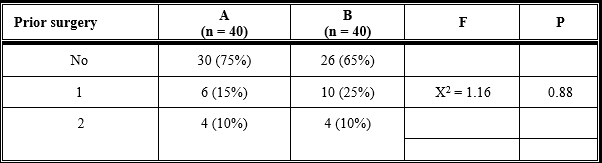
Table (2) shows percentage of previous laparotomy: In group (A) LAVH 15 cases 75% of women had no history of previous surgery, 3 only cases 15% had previous one laparotomy and 2 cases with prior history of 2 or more laparotomies. In group (B) TLH 13 cases 65% of women had no history of prior surgery, 5 (25%) of cases had prior one laparotomy and 2 10% of cases had prior 2 or more laparotomies. The data of prior surgery has no statistically significant.
The indication of laparoscopic hysterectomy in our study was only benign condition: Fibroid uterus, Endometrial hyperplasia, dysfunction uterine bleeding not responding to medical treatment and suspected adenomyosis all these indications are listed in table (3) which show: Fibroid uterus represented 35% in group (A) LAVH and 35% in group (B) TLH. Also, and hyperplasia represented 55% of cases in group (A) LAVH and 45% of cases in group (B) TLH. Dysfunction uterine bleeding (DUB) represented 10 (percentage) cases of group (B) No cases in group (A) LAVH. Suspected adenomyosis represented 10,ases in group (A) LAVH and 10,ases in group (B) TLH.
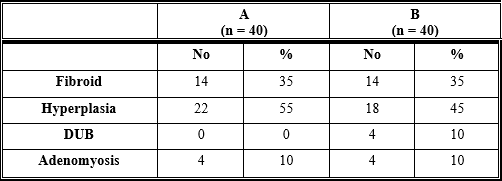
Table (4) compares the outcome measures evaluated during surgery. There was significant difference in the operating time among the 2 groups with shorter time observed in group A and longer time in group B. group (A) group (A) LAVH 104.1min S.D. 10.4. while group (B) TLH took 91.7 S.D.21.6 min. Also, this table show that the mean uterine weight in group A was 316.5 gm & S.D. 64.4. The mean uterine weight in group B was 286.79 SD 75.5. There was no statistical difference among the 2 groups.
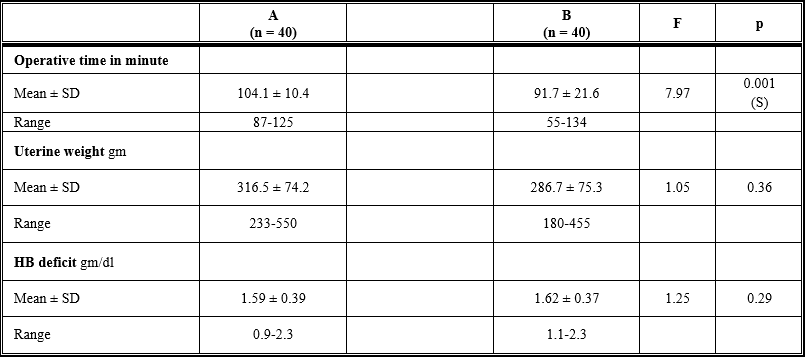
As regard hemoglobin (Hb) deficit gm/ dl.in group A and its mean was 1.59 g/dl with S.D. 0.39. In group (B) the mean of hemoglobin deficit was 1.62g/dl with SD 0.37, But not statistically difference appear between the 2 groups
Table (5) shows that blood transfusion occurs to suspected major blood loss. Conversion to laparotomy either due to uncontrolled bleeding or difficulty to manage complication. Bladder injury occurs during surgery.
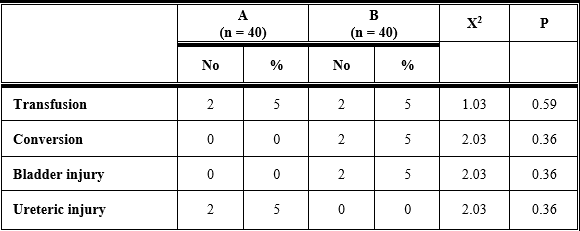
Only 4 out of 80 patients required whole blood transfusion. One patient in LAVH (group A) experienced intraoperative blood loss and one patient in the TLH (group B) for the same reason. Nevertheless, the difference among the groups were not significant. There is only 2 case of intraoperative complication which is bladder injury which occurred in group (B) (TLH) in patient which was a case of DUB and previous laparotomy was done as "cesarean section". During pushing the bladder flap downwards, the injury occurred, and immediate laparotomy was done and repairing of the bladder injury and completing hysterectomy. We asked urological surgeon to repair the bladder to avoid any injury to the ureteric orifices, this case remain in the hospital for 1 week and the catheter removed after 2 weeks. Ureteric injury noticed in the 5th day postoperatively when the patient complaint from watery discharge which is urinefarous in odor. IVP was done which discover very small ureteric fistula near the bladder wall. Consultation of urological surgeon was done and cystoureteroscopy was done to the patient with introduction of double J stent which is removed after 4 weeks, and the patient is good now this was occurred in group (A).
As shown in table (6), All patients took non-steroidal analgesic drug in the form of diclofenac sodium 100 mg (injection) and if the patient is still complaining from pain, we gave here 100 mg pethidine.
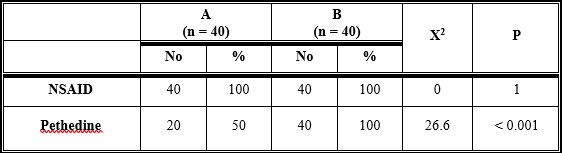
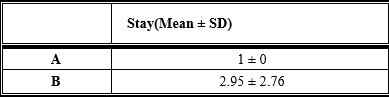
The lower mean consumption of analgesics was observed in the first group (A) and the larger consumption of analgesics observed in group B and this is statistically different. The hospital stay in all patients was only 24 hour postoperatively except in the complicated case of bladder injury where this case require hospitalization for 1 week and if we exclude this case, the time consumed postoperatively will be non-significant as shown in table (7).
Hysterectomy is the most common gynecological surgical procedure performed on women. There are three popular approaches to hysterectomy for benign disease; Abdominal Hysterectomy (AH), Vaginal Hysterectomy (VH) and Laparoscopic Hysterectomy (LH). Laparoscopic hysterectomy has three further subdivisions; Laparoscopic Assisted Vaginal Hysterectomy (LAVH) where a vaginal hysterectomy is assisted by laparoscopic procedures, Laparoscopic assisted Supracervical Hysterectomy (LASH), and Total Laparoscopic Hysterectomy (TLH) where there is no vaginal component, and the vaginal vault is sutured laparoscopically. Recently, robotic hysterectomy has also come in the field but it is not widely practiced yet [7].
Multicenter studies have shown clearly that hysterectomy is usually carried out by laparotomy, accounting for about three-quarters of all hysterectomies [8].
The primary disadvantage of abdominal hysterectomy is the prolonged recovery period mainly contributed by longer period of pain and general malaise. This may be due to the larger abdominal incision and the procedure of laparotomy itself [8].
Vaginal hysterectomy is associated with fewer complications, lower need for blood transfusion and shorter period of postoperative recovery. The progress in laparoscopic surgery made over the past few years has proved that Total Laparoscopic Hysterectomy (TLH) is a feasible technique [9].
Laparoscopic Assisted Vaginal Hysterectomy (LAVH) has been introduced as a surgical alternative to the standard methods of abdominal and non-descent vaginal hysterectomy.
Hysterectomy.
There are very few prospective randomized studies comparing various routes and types of hysterectomies. Most of the data published involves retrospective analysis of surgical technique but the Present study was a randomized prospective clinical analysis. For the operation time, our study showed that there is statistical deference among the 2 groups as the laparoscopic assisted vaginal hysterectomy (group A) showed the longest time (mean ± SD, 104 ± 10.4 minutes) due to time consuming during changing the position of the patient from trendelenburg to lithotomy position to do vaginal part of the surgery followed by reinsufflation and under water examination which took more time but TLH group (B) took about (mean ± SD, 91.7 ± 21.6 minutes).
Drahonovsky et al. (2015) did their study in Department of Gynecology and Obstetrics, 3rd Faculty of Medicine, Charles University, Czech Republic. The study was a prospective randomized study performed to a total of 125 women indicated to undergo hysterectomy for benign uterine disease were randomly assigned to three different groups (40 VH, 44 LAVH and 41 TLH). VH group showed the shortest operative time (66 minutes) and smallest drop in hemoglobin, while (TLH) group showed the longest operative time (111 minutes). (LAVH) group showed the longest amount of blood loss (306 ml) while (TLH) group showed the smallest amount of blood loss (184 ml), 3 cases out of 44 cases converted to laparotomy in (LAVH) group, 6 cases out of 41 cases converted to laparotomy in (TLH) group, one case of bladder injury in (LAVH) group out of 44 cases [10].
Our results are not in agreement with Drahonovsky et al. (2015) who showed that (LAVH) took shorter operation time than (TLH) [10].
For the hemoglobin deficit, our study stated that TLH showed the largest deficit (mean ± SD, 1.6 ± 0.37 gm/dl) and (LAVH) showed deficit of hemoglobin about (159 ± 0.39 gm/dl) and this is statistically not significant.
Mueller et al. (2019) did a study in the Department of Obstetrics and Gynecology, Erlangen University Hospital, Nuremberg, Germany was to compare Total Laparoscopic Hysterectomy (TLH) with Laparoscopically Assisted Supracervical Hysterectomy (LAVH) in women with uterine leiomyoma, 231 women underwent laparoscopic hysterectomies for the treatment of symptomatic fibroid. A total number of 113 women decided to undergo complete hysterectomy with removal of the cervix (TLH group) and 118 women wished to preserve the cervix (LAVH group). The complications occurred only in (TLH) group in the form of 2 cases of bladder injury, while no complications occurred in LASH group. The mean loss of hemoglobin in (TLH) group was 1.6 gm/dl, while in (LAVH) was 1.4 gm/dl. The hospital stay and use of analgesics were equal in both groups. He stated that (LAVH) group took shorter time than (TLH) group during the operation [11].
Mueller et al. (2019) accepted our results as they showed in their study that (LAVH) has less amount of Hb deficit (1.5 g/dl) than TLH in cases of leiomyoma which was (1.6 g/dl) in the first day post surgery.
In our prospective study, in the first group , no cases was taken blood transfusion but one case in group B was taken one unit of blood and this is due to hemorrhage from the descending cervical artery which took some time to be secured using ligasure instrument. In group B (TLH), there is 2 case was also taking blood transfusion due to bleeding from uterine artery which also was secured using ligasure instrument [11].
This transfusion rate is minimal and Drahonovsky et al. (2015) also gave blood to 2 cases in their study which was case of (LAVH).
Also, Mueller et al. (2019) had one case that was taken blood which was a case of (TLH) and this is in agreement with our study.
In our study, one case from 60 is transformed to laparotomy, this case had history of previous laparotomy which was cesarean section and during pushing bladder flab downwards, the bladder was opened and immediate laparotomy was done, the injured part is identified which was the trigon and consultant urosurgeon came immediately and close the tear after saving the ureteric orifices [10,11].
Drahonovsky et al. (2015) showed that (TLH) showed the largest conversion rate among the 3 groups as 6 cases conversed to laparotomy from 111 cases while in cases of LAVH 3 cases only converted to laparotomy from 85 cases [10].
For the hospital stay, in our study, group A the recovery was rapid, but in group B (TLH), one case took 2 days for recovery and another 4 cases took 7 days as there was urinary complication which necessitate hospital stay. So, if we exclude the 4 cases, there were no significant difference among 2 groups, but due to these 4 cases (TLH) showed the longest hospital stay duration and this is in agreement with the study of Mueller (2019) as the study showed the least hospital stay with group (LAVH) and longest stay in the group of (TLH). While Drahonovsky et al. (2015) study is not in agreement with our study as (LAVH) group showed the longest hospital stay duration and (TLH) group showed least hospital stay duration [10,11].
In our study the need for non-steroidal anti-inflammatory drugs was equal in all groups as all patients in the 2 groups were taken diclophenac sodium 100 mg injection in the early postoperative period but the need for narcotic was not needed in all patients, but the (TLH) group showed the largest number of cases who need narcotic.
Morelli et al. (2017) stated in his study that no statistically difference was found in the complication rate and postoperative recovery period between (TLH) and (LAVH).This study was done on one hundred and forty one patients who complained of symptomatic leiomyoma and abnormal uterine bleeding non-responding to medical treatment [12].
The results of Morelli et al. (2017) are not in agreement with the results of our study as we found significant difference in both postoperative stay and intraoperative complication between the (TLH) group and (LAVH) group as (TLH) took longer mean period of hospital stay, but (LAVH) took only 24 hours, but the longer duration in (TLH) group only occurred in 2 cases, one case converted to laparotomy due to bladder injury and the 2nd due to presence of drains which necessitate staying for another day and if we exclude these two cases, our results will be as the results of Morelli. For the complication rate in our study,there was no complication in group A(LAVH) while the complication rate more in (TLH) than (LAVH) but not significant, Morelli (2017) showed also that there was no significant difference between the 2 groups [12].
Long et al. (2012) in a study done on 120 patients to compare the operative and postoperative data between two groups; the first group where (LAVH) (n = 60) was done and 2nd group where (TLH) (n = 60) was done. They found that (LAVH) showed the shorter operation time than (TLH) , but they were using extracorporeal knot in ligation of the pedicles and this might be the cause of elongation of the operative time in (TLH) group. This result was not in agreement with the results of our study as we stated that (LAVH) group took the longest operation time and (TLH) group consumed shorter period during the operation and this happened with us, as we use Ligasure instrument in securing and cutting blood vessels and pedicles. Also, the time consumed during changing the position of the patient from Trendelenburg to lithotomy position during doing the vaginal part of the surgery [13].
Long et al. (2012) also stated that (LAVH) group stay for shorter period in the hospital than (TLH) group and this agreed with our results. Also, the complication rate between both groups was non-significant and this was in agreement with our results.
The study of Roy et al. (2020) showed that (TLH) took significantly longer time (105 ± 23 minutes) than (LAVH) (89 ± 21 minutes), and this results are not in agreement with our study which showed that (LAVH) group took longer operation time than (TLH) group. But if the mean blood loss was 290 ± 124 ml in (TLH) and 302 ± 130 ml in (LAVH), this means that(TLH ) group showed less blood loss than (LAVH) group and this is not in agreement with our study that stated the opposite. He also found that there were no statistically differences between (TLH) and (LAVH) groups in the postoperative stay. While our study showed that there was statistically difference in the postoperative stay where the group of (TLH) showed higher rate in the hospital stay and, in the complication, [1].
In a study done by Mousa et al. (2018) in Royal Vectoria Hospital, Montereal Canada, they stated that there were no statistically differences in the hospital stay between (LAVH) group and (TLH) group. Also, no statistical difference in the Hb deficit between the 2 group after the 1st postoperative day and this is agree with our result concerning Hb deficit only, but our result is not agreed with Mousa result's regarding hospital stay as in our result the length of hospital stay is more in group (TLH) than in (LAVH) group. Also, In the study of Mousa et al. (2018), no statistically difference between (LAVH) and (TLH) regarding major and minor complication. Also in our result, no statistically difference but there was one major complication in (TLH) group which was bladder injury which required conversion to laparotomy [14].
Jin and Jang (2018) in a study including 120 patients; 60 of them were underwent (LAVH) and 60 women underwent (TLH). There were no significant differences in patients' clinical characteristics (age and weight) and the hospital stay and this is in agreement with our result. They also found a longer operation time in (TLH) group (mean, 105 minutes) which is statistically different than (LAVH) group (86 mm), but this result is not matched with our results regarding operation time. Also, they showed that (LAVH) group has the merits of less blood loss than (TLH) group and this agreed with our result as blood loss in (LAVH) group was 1.59 gm/dl while in(TLH) was 1.62 gm/dl.
Laparoscopic assisted vaginal hysterectomy showed lower complication but longer operative time than total laparoscopic hysterectomy group; also (LAVH) showed shorter hospital stay and need fewer analgesics so we considered this method the best when the patient accepted total removal of the uterus. While total laparoscopic hysterectomy showed the more blood loss and complication intraoperatively and postoperatiovely, but this complication is non-significant in cases of removal of the hole uterus.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
