
Case Report | DOI: https://doi.org/10.31579/2768-2757/167
Professor, head of the department of pediatric surgery.
*Corresponding Author: Mirolyubov L.M., Professor, head of the department of pediatric surgery.
Citation: Mirolyubov L.M., (2025), Comparative Characteristics of Methods for Treating Partial Anomalous Pulmonary Venous Drainage (PAPD), Journal of Clinical Surgery and Research, 6(4); DOI:10.31579/2768-2757/167
Copyright: © 2025, Mirolyubov L.M. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 April 2025 | Accepted: 28 April 2025 | Published: 20 May 2025
Keywords: pediatric cardiac surgery; cardiac surgery; cardiovascular surgery
The final situation regarding the treatment of CHADLV with or without ASD remains alarming in terms of the prognosis of postoperative cardiac arrhythmias and remote stenotic complications at the mouth of the SVC. We have developed and tested in the clinic our own original method of correction of CHADLV taking into account the prevention of stenotic complications in the remote period, as well as postoperative cardiac arrhythmias.
It is known that partial Anomalous pulmonary venous drainage (APVD) is one of the most common pathologies of pulmonary venous return [1, 2, 3]. The defect was first described by Winslow (1739). During a pathological examination, he discovered abnormal drainage of the pulmonary vein of the upper lobe of the right lung into the superior vena cava. The anatomy and clinical features of this defect were most fully studied by Brody (1942). R. Darling et al . (1957) systematized the anatomical variants (types) of the defect . In most cases (97.2%), drainage of the right pulmonary veins is observed, and in the rest - the left [4]. The incidence of this defect is at least 1.5% among all congenital heart defects (CHD) [1, 5]. The average life expectancy of patients with CHD without surgical correction does not exceed 37-40 years [1,2]. The first successful operation to correct CADPV using the closed method of "atrioseptopexy" was performed by W. Neptune in 1953. The modern stage of treatment of the defect began with the introduction of open heart surgery into clinical practice. In 1955, under hypothermia conditions, F. Lewis was the first to perform an operation to correct abnormal drainage of the pulmonary veins into the right atrium and superior vena cava. Later, artificial blood circulation began to be used to perform the operation. Partial correction is particularly difficult abnormal drainage of the right upper pulmonary veins into the superior vena cava (AUPV to SVC) with or without an atrial septal defect (ASD). The most common surgical treatment for ASD involves the application of an intra-atrial patch made of autopericardium, which directs blood flow from the pulmonary veins through the ASD into the left atrium (LA). The applied patch, which forms a tunnel, narrows the lumen of the superior vena cava in the area of its mouth by half or more, therefore, in order to preserve the true volume-diameter and prevent venous hypertension in the SVC system, it is necessary to apply a second patch outside the atrium (usually it is made of xenopericardium, since the autopericardium has already been used).
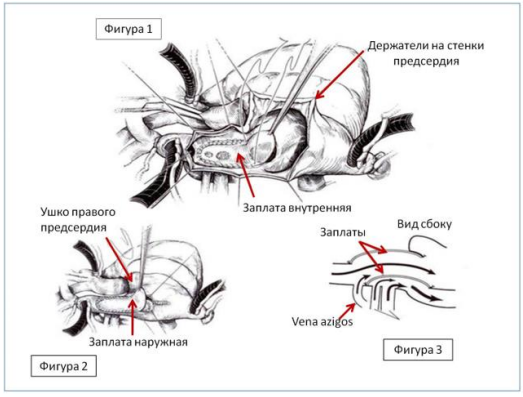
Figure 1: An internal patch is applied, which transfers the pulmonary veins into the left atrium.
Figure 2: External patch of xenopericardium to prevent narrowing in the area of the first patch. Classic version.
Figure 3: Blood flows after plastic surgery. Side view.
The above-described two-patch method of surgical treatment of CHADLV is the "gold standard" in the treatment of this pathology. In the cardiac surgery department of the Republican Children's Clinical Hospital of the Ministry of Health of the Republic of Tatarstan, we have used it for quite a long time. At late stages after the operation, from 1 to 3-5 years, patients operated by us repeatedly returned with phenomena of venous hypertension in the system of the superior vena cava. The cause of complications at late stages of observation in all cases was the fibrous-cicatricial process with phenomena of calcification of the xenopericardial patch, which led to narrowing of the mouth of the superior vena cava. The method proposed by Verdun et al ., which also provides, as in the classical version, the application of a patch on the ASD with the simultaneous transfer of anomalous veins to the left atrium, and then, in order to prevent narrowing in the area of the mouth of the superior vena cava, the implementation of a direct anastomosis of the right atrial appendage with the cut off superior vena cava. It turned out that Verdun's method does not guarantee against stenotic complications in the area of the suture strip and complications from the conduction system of the heart (the sinus node, the master of the cardiac rhythm, is located in the mouth of the superior vena cava). In 2019, Krivoshchekov E.V. and co-authors modified the Verdun method by cutting out a shaped flap from the atrial wall, also trying to reduce the number of complications in the long-term observation period. The final situation regarding the treatment of CHADLV with or without ASD remains alarming in terms of the prognosis of postoperative cardiac arrhythmias and remote stenotic complications at the mouth of the SVC. We have developed and tested in the clinic our own original method of correction of CHADLV taking into account the prevention of stenotic complications in the remote period, as well as postoperative cardiac arrhythmias. The method involves access to the right atrium to the pulmonary veins and ASD by an incision along the upper edge of the superior vena cava with a transition to the lower ridge-rib of the right atrial appendage. The access provides good visualization of the necessary structures, and from it we perform the application of an internal patch with the transfer of the abnormal drainage. Instead of the second patch, we use a dissected auricle, the apex of which easily reaches the upper edge of the dissected superior vena cava. Suture strips along the edges of the auricle and the dissected vein allow us to cover the orifice of the SVC narrowed by the first patch like a hood. Priority reference…. The results were followed for 7 years. 19 patients were operated on, postoperative rhythm disturbances and stenotic disorders were not observed in any case.
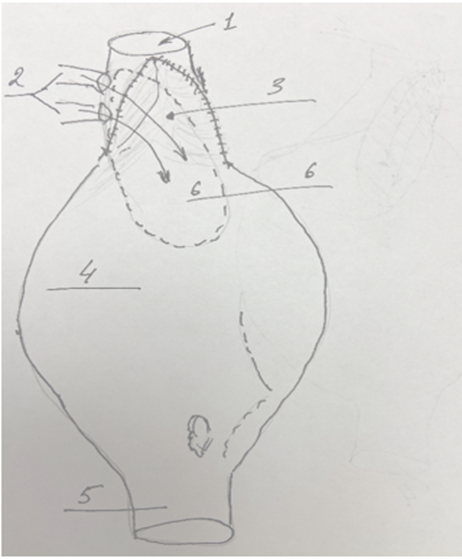
Figure 4: After applying a patch with the transfer of abnormal veins to the left atrium, plastic surgery of the vein mouth was performed with tissue from the atrial appendage: “Covering with a hood”.
1-superior vena cava; 2-anomalous veins; 3-upper part of the auricle with the borders of the suture strip; 4-atrium; 5-inferior vena cava; 6-projection of the internal patch. Priority for invention from January 2025.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
