
Case Report | DOI: https://doi.org/10.31579/2641-0419/436
1 Chief Cardiologist.
2 Senior Consultant, Interventional Cardiologist.
3 Academic Executive. SKY Hospital & Research Centre Pvt. Ltd., India.
*Corresponding Author: SKS Lairikyengbam, SKY Hospital & Research Centre Pvt. Ltd., Imphal, India.
Citation: SKS Lairikyengbam, Ramdeo Yadave, Arica Devi Mayanglambam, (2025), Combo Drugs Therapy Improves Restoration of Patency of Culprit Vessel in Acute ST-Elevation Myocardial Infarction – A case report of 3 patients, J Clinical Cardiology and Cardiovascular Interventions, 8(1); DOI: 10.31579/2641-0419/436
Copyright: © 2025, SKS Lairikyengbam. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 December 2024 | Accepted: 27 December 2024 | Published: 06 January 2025
Keywords: door to needle time; culprit vessel; acute myocardial infarction
Acute ST-Elevation Myocardial Infarction (STEMI) usually results from an occlusive coronary thrombus at the site of a ruptured atherosclerotic plaque. Thrombolysis has a role in the management of patient with acute STEMI and restoration of culprit vessel arterial flow as normal as possible. Early thrombolytic therapy in acute STEMI reduced mortality by the time of hospital discharge and better functional outcomes at 6 months. Thrombolytic therapy when given within 10 minutes of arrival at the Emergency Room helped restore the patency of culprit vessel patency to 0-30% in our 3 patients with acute STEMI. This may indicate that thrombolytic therapy augmented with loading anti-platelet drugs and bolus intravenous drug enoxaparin given in ≤ 10 minutes may be a viable alternative to primary percutaneous coronary intervention when the later is not available or not possible within Door-to-Balloon time of 120 minutes.
STEMI- ST Elevation Myocardial Infarction;
LVEF- Left Ventricular Ejection Fraction;
CAG- Coronary Angiogram;
DTE- Door-to-ECG time;
DTD- Door-to-Diagnosis time;
DTB- Door-to-Balloon time;
DNT- Door-to-Needle time;
DAP- Dual Antiplatelet Therapy;
FMC- First Medical Contact;
LAD- Left Anterior Descending,
ER- Emergency Room,
CAD- Coronary Artery Disease
Coronary artery disease (CAD) is a major cause of morbidity and mortality in India. Approximately, 8-10% of Indians in urban areas and 3-4% in rural areas have CAD [1-4]. Dedicated Heart Attack Treatment Centre (HAC) was established at SKY Hospital and Research Centre Pvt. Ltd., Imphal, India in July, 2016 providing 24x7 services, early ECG, loading dose of dual anti-platelet (DAP) drugs, timely administration of thrombolytic therapy for acute STEMI, and early patients transfer to ICCU. Bedside Echocardiogram is performed at the time of admission in ICCU. Our HAC Team consists of Consultant Cardiologist/middle grade Cardiologist on site, other Emergency Medical Officers and well trained nurses. International guidelines are clear in specifying that patients with acute STEMI should receive urgent Coronary reperfusion with either primary percutaneous coronary intervention (pPCI) or thrombolysis [5].
The pPCI is available to less than 10% of STEMI patients in India (CREATE registry) [6]. Consequently, local recommendation on STEMI management exists to promote timely administration of thrombolysis within 30 minutes of patient arrival [7, 8] and then within 10 minutes [9, 10]. Here we present 3 cases in which restoration of complete or near complete patency of the culprit vessel was observed after treatment at HAC of our hospital.
Case 1
A 57 years old man with a history of smoking was admitted to the ER on November 19, 2021, by his family 1 hour 30 minutes after onset of chest pain and breathlessness. On examination, blood pressure was 150/110 mmHg; heart rate of 93 beats per minute. He was resuscitated immediately and intensively. An ECG was obtained on admission which revealed acute extensive antero-lateral STEMI, Figure.1(a). Serum Troponin T was found raised at 2000 ng/L (normal value ˂ 40 ng/L). Loading Double Antiplatelet Drugs, Tab. Ecosprin, 300 mg and Tab. Ticagrelor, 180 mg were administered. Immediate thrombolytic therapy with inj. Reteplase 18 mg in 2 minutes as first dose followed by 18 mg after 30 minutes. Inj. Enoxaparin 30 mg was given intravenously within 10 minutes of the patient’s arrival at ER (Table 1). An Echocardiogram examination revealed akinetic apex involving 25% of left ventricle, dilated left ventricle with reduced LVEF (47.94%), mild mitral regurgitation, mild left ventricular hypertrophy, minimal tricuspid regurgitation, no Pulmonary Arterial Hypertension (PAH), mild pulmonary regurgitation, normal pericardium. Further investigation revealed that he had dyslipidaemia.
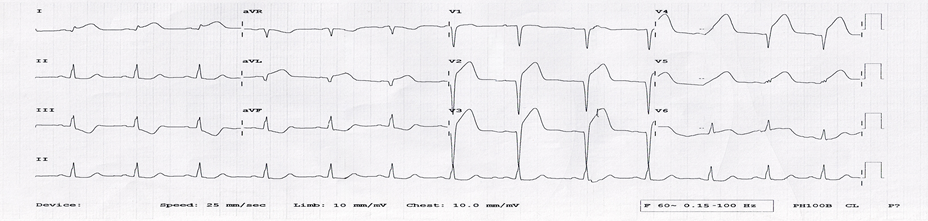
Figure:1(a): ECG on admission
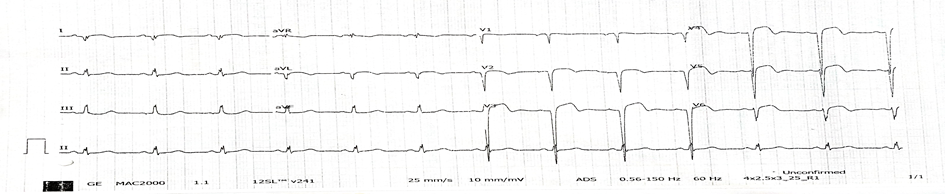
Figure:1(b): ECG post thrombolysis
Post-Thrombolytic therapy coronary angiogram revealed recanalised proximal LAD with only 30% residual stenosis Figure:1(c): Patient’s condition improved and was stable at the time of discharge on November 29, 2021.
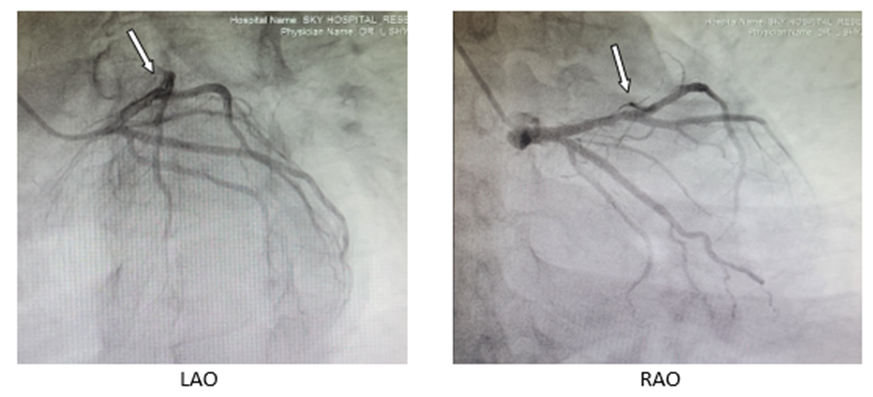
Figure:1(c): Case 1 patient’s CAG photos showing recanalised proximal LAD with 30 % residual stenosis only.
Case 2
A 46 years old man with a history of hypertension, CVA (ischaemic, 2020 with left Grade 4 hemiparesis), smoking, history of Covid-19 (2020) was admitted to the ER on November 12, 2023, by his family with chief complaints of chest pain and breathlessness. On examination, blood pressure was 180/110 mmHg; heart rate of 90 beats/min. An ECG was obtained on admission which revealed acute extensive antero-lateral STEMI, Fig.2(a). Serum Troponin T was found raised at 668 ng/L (normal value ˂ 40 ng/L). Immediate treatment started to resuscitate the patient. Intravenous Glyceryl trinitrate infusion was started to control the accelerated hypertension which was gradually weaned off. Loading Double Antiplatelet Drugs, Tab. Ecosprin, 300 mg and Tab. Ticagrelor, 180 mg were administered. Immediate thrombolytic therapy with inj. Tenecteplase 35 mg was given over 2 seconds. Inj. Enoxaparin, 30 mg was given intravenously within 10 minutes of the patient’s arrival at ER (Table 1). An Echocardiogram examination revealed apical akinesia involving 25% of left ventricle, dilated left ventricle with moderate left ventricular systolic dysfunction (LVEF=43.5%), mild left ventricular hypertrophy, mild left ventricular diastolic dysfunction, mild mitral regurgitation, minimal tricuspid regurgitation, no PAH (PASP = 17.0 mmHg), intact interatrial septum and interventricular septum and minimal pericardial effusion. On further investigation, he was found to suffer from Type II Diabetes Mellitus.

Figure:2(a): ECG on admission.

Figure:2(b): ECG post thrombolysis
Post-Thrombolytic therapy coronary angiogram revealed recanalised LAD with 30 % residual stenosis Figure:2(c). Patient was stable at the time of discharge on November 24, 2023.
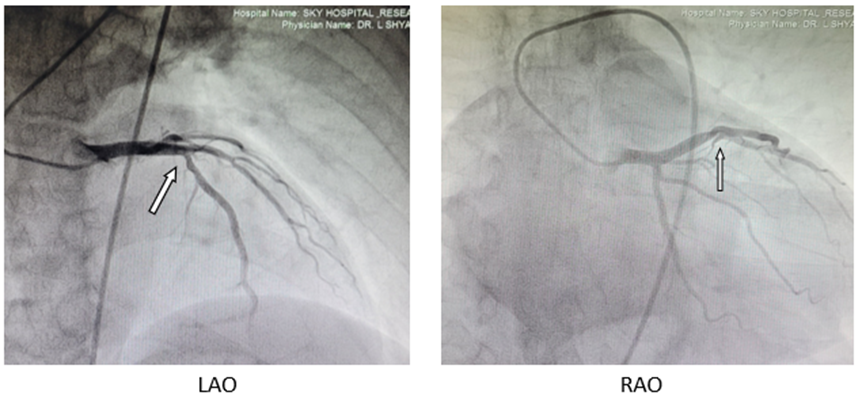
Figure: 2(c): Case 2 patient’s CAG photos showing CAD with recanalised LAD with 30 % residual stenosis only.
Case 3
A 50 years old woman was admitted to the ER on April 6, 2024 transferred from another hospital with acute anterior wall STEMI and hypoxia. On examination, blood pressure was 110/70 mmHg; heart rate of 58 beats/min. She was resuscitated immediately. On admission, ECG revealed Acute extensive antero-lateral STEMI, Figure.3(a). Serum
Troponin T was found raised at 264 ng/L (normal value ˂ 40 ng/L). Loading Double Antiplatelet Drugs, Tab. Ecosprin, 300 mg and Tab.
Ticagrelor, 180 mg were administered. Immediate thrombolytic therapy with inj. Tenecteplase 35 mg was administered over 2 sec. Inj. Enoxaparin, 30 mg was given intravenously within 10 minutes of the patients arrival at ER (Table 1). An Echocardiogram examination revealed akinetic left ventricular apex involving 1/3rd of left ventricle, dilated left ventricle with reduced LVEF (51.6%), mild mitral regurgitation, moderate tricuspid regurgitation and mild PAH (PASP=38.2 mmHg).

Figure:3(a): ECG on admission.
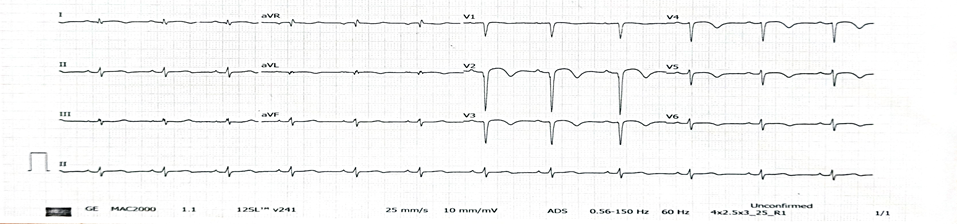
Figure:3(b): ECG post thrombolysis.
Post-Thrombolytic therapy coronary angiogram revealed fully recanalised the LAD Figure:3(c). Patient’s condition improved. She was mobilized and stable at the time of discharge on April 18, 2024.
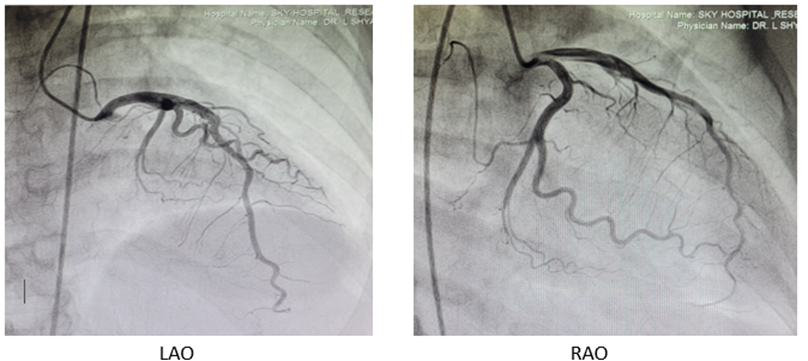
Figure:3(c): Case 3 patient’s CAG photos showing fully recanalised LAD.
| Characteristics | Case 1 | Case 2 | Case 3 | ||
| Demographic characteristics | |||||
| Age (years) | 57 | 46 | 50 | ||
| Sex | Male | Male | Female | ||
| Medical history | Dyslipidaemia |
|
| ||
| Clinical Characteristics | |||||
| Chief Complaints | Chest pain Shortness of Breath on exertion | Chest pain Breathlessness | Chest pain | ||
| DTE | 2 minutes | 1 minute | 2 minutes | ||
| DTD | 3 minutes | 3 minutes | 3 minutes | ||
| Loading dose of DAP | 5 minutes | 4 minutes | 4 minutes | ||
| DNT | 10 minutes | 10 minutes | 5 minutes | ||
| Post-Thrombolysis CAG | Recanalised proximal LAD with 30% residual stenosis | Recanalised proximal LAD with 30% residual stenosis | Fully recanalised the LAD | ||
| LVEF at the time of admission | 47.9% | 43.5% | 51.6% | ||
| LVEF at 7days post discharge | 49.2% | 44.4% | 52.5% | ||
| Days of hospital stay | 10 | 12 | 12 | ||
| Activities- Walk independently without symptoms (Telephone follow up post-thrombolysis on 13-11-2024) | 1 kilometer
| 500 meters | 400 meters | ||
| Health status post-thrombolysis | Asymptomatic | Asymptomatic | Asymptomatic | ||
Table 1: Demographic, clinical characteristics and laboratory findings at the time of the thrombotic event.
Of the 3 patients, 2 were males and 1 was female. The age groups range from 46 years to 57 years. All patients received intravenous thrombolysis between the 10 minutes of presentation at ER. CAG shows that revascularization was successful in 100% of cases and good clinical outcomes were achieved. Early administration of thrombolytic therapy in acute STEMI reduced mortality by the time of hospital discharge and better functional outcomes at 6 months.
Any model of acute STEMI care in India should have the principal objectives of improving the speed of reperfusion, and reducing the time from symptom onset to treatment [11]. These can be achieved by ensuring a quick response time (QRT) to perform an ECG at the point of FMC, a prompt initiation of bolus DAP drugs, thrombolytic therapy and intravenous Enoxaparin or other approved anticoagulants. Reperfusion therapy is also recommended in acute STEMI patients with evidence of ongoing ischemia within 12–24 hrs of symptom onset [12].
For our case, all received loading DAP drugs, bolus intravenous anticoagulants and third generation thrombolytic agent within 10 minutes of diagnosis of acute STEMI. Post lysis CAG for all patients showed normal or near normal restoration of patency of culprit arteries.
Thrombolytic therapy along with loading dose of DAP and bolus Enoxaparin, all given within 10 minutes of diagnosis of acute STEMI may be a viable alternative to primary percutaneous coronary intervention when the later is not available or not possible within DTB of 120 minutes [10, 13]. Larger randomized controlled trials will be necessary to substantiate our finding.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
