
Case Report | DOI: https://doi.org/10.31579/2693-4779/097
1 Clinic for Pediatric Surgery, Clinical Center of the University of Sarajevo.
2 Department of Surgical Diseases - Cantonal Hospital Zenica.
3 Surgical Diseases, Tešanj General Hospital.
4 Clinic for Anesthesia and Reanimation, Clinical Center of the University of Sarajevo.
5 Oceania University of Medicine, Melbourne, Australia.
*Corresponding Author: K. Karavdić, Clinic for Pediatric Surgery, Clinical Center of the University of Sarajevo.
Citation: K. Karavdić, A. Firdus, Mulahalilović A, Đogić H, Altunbabić L, Dewan P.A. (2022) Combined Extraction (Cystourethroscopy and Suprapubic Cystotomy) of A Selfinserted Hairpin Located In The Posterior Urethra - A 7-Year-Old Boy. Clinical Research and Clinical Trials. 6(1); DOI: 10.31579/2693-4779/097
Copyright: © 2022 K. Karavdić. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 April 2022 | Accepted: 06 May 2022 | Published: 16 May 2022
Keywords: hairpin; urethra; cystourethroscopy; suprapubic
Self-inserted urethrovesical foreign bodies are rare in children. A 7-year-old boy inserted a hairpin into the urethra seven days before admission, a diagnosis that was made on the basis of the appearance of blood in the urine, palpation of the base of the penis and two directional X-ray imaging. Cystourethroscopy and suprapubic cystotomy were used to remove the foreign body.The presentation of urethrovesical foreign bodies can vary widely, as can the type of object inserted. Definitive treatment is usually the endoscopic removal, however occasionally surgical intervention may be required. Our novel approach enabled less traumatic removal of the hairpin
Self-inserted intra-vesical and intra-urethral foreign bodies are rare emergencies in Pediatric Urology, although there has been an increase in reports in the last few decades [1]. Previous studies have reported several different inserted items which were found in the urethra and/or the urinary bladder including sharp and lacerating, wire-like objects objects [2]. Most of the intravesical foreign bodies are the result of self-introduction, but they can also result from medical procedures, migration from the surrounding organs or penetrating injuries. In self-introduced foreign bodies, most patients feel embarrassed, tend to postpone medical help and present to a tertiary institution after multiple removal attempts, which risk urethral injury and foreign body migration. Here-in we present a case of a foreign body in the urethra, and we discuss the clinical presentation, diagnosis and management of patient.
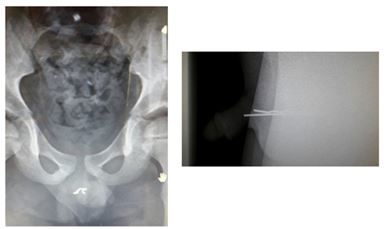
A seven-year-old boy was admitted to the emergency department in a regional hospital. The patient denied symptoms, but his mother noticed blood in his underwear. The mother said that the boy complained of dysuric problems, the appearance of blood when urinating, as well as the appearance of purulent contents on urethral meatus. The dysuria was reported to have been present for seven days. The boy had not reported inserting an object into his urethra; never-the-less he was intellectually, psychologically and neurologically a normal child, and his mother denied previous similar incidents. The examining pediatrician noted haematuria and prescribed antibiotics, despite which the symptoms worsened, and the patient reported to the pediatric surgery unit in the regional hospital. Posterio-anterior and lateral X-rays of his pelvis showed a radio-opaque foreign body consistent with a hairpin-shaped structure, located in the regions of the penis.(figure 1,2).
An attempt to remove the hairpin in the regional centre failed, and he was transferred to our clinic, where he was noted to have blood at the urethral meatus.
At the base of the penis was a firm smooth-edged painful mass At urethroscopy a hairpin was observed in his bulbar urethra, which was swollen and hyperaemic. The sharp end of the hairpin, located in the penile urethra, faced distally and was firmly driven into the inflamed mucosa of the urethra. Thus, was unable to extrated throught the meatus. Therefore, the hairpin was pushed into the bladder, facilitated by the blunt end facing toward the bladder. (figure 3,4,5).


After the hairpin was pushed retrogradely into the bladder, transurethral mobilization from the hairpin into the urinary bladder, the bladder was filled with saline, and a 5 mm suprapubic extraperitoneal laparoscopic trocar inserted into overfilled bladder, under transurethral cystoscopic vision. Thus transvesical extraction was achieved through the suprapubic trocar with a 5 mm grasper.(figure 6) A catheter was inserted, and remained for 8 days, after which he made a good recovery.(figure 7).


Foreign body insertion into the Paediatric lower urinary tract occurs infrequently, with a male to female ratio of two to one. (3) However, females are at an increased risk for foreign body migration into the bladder, due to short urethral length, and straight trajectory of the female urethra. Self-introduction of the foreign bodies is rarely seen in young children [4], generally occurring early in the puberty, as for our case.
The explanation for self-insertion of foreign bodies often reflects psychiatric disorders, accidental insertions, seeking sexual stimulation, attention seeking behaviour, or simple curiosity; most common in patients with psychiatric illness [5].
Urethral and intravesical foreign bodies are important considerations in the differential diagnosis of lower urinary tract symptoms. Clinical presentation may vary from asymptomatic to swelling of external genitalia, lower abdominal pain, dysuria, urethral discomfort, pollakiuria, nocturia, haematuria, bloody or purulent urethral discharge, painful erection, difficulty in voiding, urinary retention. A high index of suspicion is necessary for diagnosis and management of these challenging cases. A urethral foreign body left untreated can lead to serious complications such as urethral stenosis, periurethral abscess, and/or fistula [6].
A high proporation of patients do not admit to the insertion of a foreign object because of embarrassment or mental illness, resulting in the nonspecific symptoms making the diagnose difficult, until imaging is undertaken, as in our case. The resultant delay in diagnosis makes the resultant extraction procedure more difficult, due to inflammatory changes in the urethral mucosa and the possibility of urethral injury with endoscopic manipulation.
Plain-films of the pelvis are generally enough to evaluate number, location, size or orientation of radio-opaque objects for the purposes of treatment planning; computed tomography or ultrasound may be necessary if the object is radio-lucent [7]. Immediate management of patients with a urethral foreign body should be pain relief, control of voiding symptoms with either anticholinergic medication for irritative symptoms, or bladder catheterization if unable to void.
Rahman et al recommends treatment with broad-spectrum antibiotics prior to foreign body removal [8]. Palmer et al recommends empiric coverage for Gram-negative organisms for a duration of 1 week [9]. In case of positive cultures or sepsis, antibiotic coverage should be broadened or tailored as appropriate. Definitive treatment is removal of the foreign bodies with minimal or no urethral morbidity and without compromising erectile function [10]. Choosing the optimal technique for removal of the foreign body is dependent on the patient’s condition and age, urinary tract injuries and the size, shape and material of foreign body. Various methods including meatotomy, cystoscopy, internal or external urethrotomy, suprapubic cystostomy, Fogarty catheterizations and injection of solvents have been used. In cases where endoscopic techniques are unsuitable or unsuccessful, open surgical removal is necessary. For objects lodged in the penile urethra, external urethrostomy is recommended, while a suprapubic cystostomy is the procedure of choice for intravesical foreign bodies; treatment should be individualized according to the particular patient [11].
The first-line treatment is minimally invasive removal by cystoscopy in which the object is grasped and extracted with forceps, graspers, snares or retrieval baskets. Following removal, cystourethroscopy is important to diagnose urothelial injuries and to ensure complete removal of foreign bodies [12]. When the object is visible through the external urethral meatus or is suspected to be small and distally located, gentle manual traction may be applied to try and deliver the object [9]. External urethrotomy has also been described; however, this approach has some potential complications including dehiscence or periurethral abscess secondary to urethral damage should the object is impacted [13]. An undetermined diameter, length or material of the object has been described as contraindication for endoscopic removal. Whenever a surgeon believes that an attempt of endoscopic removal will no doubt result in a traumatic or unsuccessful procedure, the patient should be directly taken for open surgery [14]. In most cases, the formation of multiple knots may preclude safe transurethral removal and some authors have employed suprapubic cystotomy. In the patient of case the decision was made to perform a suprapubic cystotomy to minimize further urethral trauma and expedite extraction. The sharp part of the hairpin was facing toward the outer meatus of the urethra, and had buried itself into the mucosa over a 7 day period, making extraction via the urethra likely to lead to excessive damage to the urethra.
In the circumstance our case there was less risk to the urethra by pushing the blunt end of the hairpin into the bladder, which would obviously be able to be used for other similarly shaped foreign bodies.
Other therapeutic options have been an especially designed magnetic retriever for magnetic extraction of a small metallic intravesical object, such as a hair pin or clip; and the YAG laser has also been used for paraffin and wax objects are frequently reported as foreign intraurethral and intra-vesical objects [2,11] ... previously solvents (xylol, kerosen, benzene) were used to dissolve these objects however, since their known carcinogenic risk, its use is no longer recommended. Endoscopic removal of wax and paraffin is further complicated as these substances tend to float on water, which can be countered by using carbon dioxide insufflation, then removal [15].
Complications following removal of urethral foreign bodies include urethral false passages, mucosa tears with subsequent haemorrhage, urethritis, fistulae, urethral stricture, diverticulum and incontinence. Urethral strictures are the most common delayed complication with a 5% incidence [16]. Therefore, close follow-up of a long duration is advocated to detect delay obstructive symptomatology.
Also, routine Psychiatric/Psychological evaluation should be offered to all patients with intentional foreign body insertion to avoid missing any underlying psychiatric disorders, and because there is a high incidence of recidivism, noting that educating patients about the long-term sequelae is important to try to avoid repeated foreign body insertion [17].
Diagnosis of the existence of a foreign body in the urethra in the pediatric age is a major challenge. Therefore, the diagnosis should be considered in the presence of dysuria and haematuria, and palpation and radiological examination should be considered. When diagnosed, careful consideration should be given to the techniques of removal to ensure minimal secondary urethra injury, which may include retrograde passage of the foreign body and transvesical extraction, as in our case
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
