
Review Article | DOI: https://doi.org/DOI: 10.31579/2766-2314/108
1 Department of Biomedical Engineering, School of Engineering and Applied Science, Libyan Academy, Tripoli, Libya.
2 Higher Institute of Science and Technology, Rabta, Libya.
3 Faculty of Medical Technology, University of Zawia, Libya.
4 Bahrain Royal Medical Services.
*Corresponding Author: Altayeb Elazomi, Faculty of Medical Technology, University of Zawia, Libya.
Citation: Abdulbasit Faraj Hadhr, Jamela Boder, Fathi B. Abdalla, Altayeb Elazomi, (2023), Colorectal Cancer: Insight into Incidence, Risk Factors, Diagnosis, and Prognostic Markers, J, Biotechnology and Bioprocessing, 4(5); DOI: 10.31579/2766-2314/108
Copyright: © 2023, Altayeb Elazomi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 July 2023 | Accepted: 14 July 2023 | Published: 24 July 2023
Keywords: colorectal cancer; incidence; risk factors; diagnosis; prognostic markers
Background: Colorectal cancer is one of the most common malignancies and a leading cause of cancer death worldwide.
Objectives: The current review aimed to highlight colon cancer incidence, risk factors, diagnosis, and prognostic markers. Colorectal cancer is the second most common type of cancer, it was responsible for 18.7% and 15.1%, of all cancer in Portugal. The mean age of incidence is about 60 years. The aetiological and pathogenesis of colorectal cancer are usually related to both environmental and genetic factors. Patients with inflammatory bowel disease have a definite predisposition to colorectal carcinoma. Some genetic syndromes transmitted in the family from generation to generation can increase the risk of colon cancer. The most well-defined environmental risk is exposure to ionizing radiation. If the patient has benign glandular tumors before, he is more likely to have colon or rectal cancer. Also, medical history, alcohol consumption, age, diet, physical activity, diabetes, smoking, and geographic differences are from risk factors for colorectal cancer. One of the best methods for detection of colon cancer is a screening program with blood in stool, routine physical and endoscopic examination. The person who is on risks such as personal history of adenomas or CRC, family history of CRC or adenomas in first degree relatives before age 60 years, inflammatory bowel disease, and family history of hereditary syndromes. The usual clinical picture of an early colorectal cancer is a change of bowel habit and painless mild bleeding particularly in the left side tumors. Abdominal lymph nodes (38%) are the second most frequent site of metastasis (38%), just after liver, which is, the organ that most frequently involved (38–60% of cases) and followed by the lung (38%) and the peritoneum (28%). Colon cancers can be graded according the degree of differentiation to well differentiated (grade I). Grading Adenocarcinomas are graded predominantly on the basis of the extent of glandular appearances, and should be divided into well, moderately and poorly differentiated, or into low-grade (encompassing well and moderately differentiated adenocarcinomas) and high-grade (including poorly differentiated adenocarcinomas and undifferentiated carcinomas). the mitotic activity index (MAI) is an independent prognostic factor for recurrence free survival. SMI is a bit more efficient than MAI as a prognosticator. Classical prognostic markers in histopathology are histological grade, mitotic activity, histological type, angiogenesis, and tumor necrosis. Multivariate clinicopathological prognostic indices, molecular prognostic markers in colon cancer, the younger is the patient, the greater is the cellular proliferation and the lower is the degree of differentiation. With increasing malignancy an increased frequency of invasion and metastasis are observed and hence poor prognosis of the tumor Cell proliferation markers. Rational mutations in one allele of the p53 gene associated with congenital or acquired congenital loss of the other leads to continuous cell growth the later can promote carcinogenesis in many organs, including colon, lung, and breast. Ki-67 is a cell proliferation marker. Tumors associated with microsatellite instability tend to be mucinous or poorly differentiated with a prominent host response a circumscribed growth pattern and right-sided location in one study presence of tumor-infiltrating lymphocytes was found to be the best histological predictor of microsatellite instability.
Conclusion: It can be concluded that the colorectal cancer is one of the most common malignancies. The aetiological and pathogenesis of colorectal cancer are usually related to both environmental and genetic factors. The colorectal cancer risk factors are medical history, alcohol consumption, age, diet, physical activity, diabetes, smoking, and geographic differences. the best methods for detection of colon cancer are a screening program with blood in stool, routine physical and endoscopic examination. Classical prognostic markers in histopathology are histological grade, mitotic activity, histological type, angiogenesis, and tumor necrosis. With increasing malignancy an increased frequency of invasion and metastasis are observed. Rational mutations in one allele of the p53 gene associated with congenital leads to continuous cell growth the later can promote carcinogenesis in the colon. Tumor-infiltrating lymphocytes were found to be the best histological predictor of microsatellite instability. Further studies about colorectal cancer are needed to prove strategies for controlling the prevalence of the disease and the more accurate method for diagnosis.
Colorectal cancer (CRC) is one of the most common malignancies and a leading cause of cancer death worldwide [1, 2]. European countries rank the highest in the global statistics in terms of both CRC incidence and mortality [3 , 4], although in recent years, a decline in CRC mortality rates has been observed, mostly due to improvement in earlier diagnosis and treatment [3 , 5]. Among the key risk factors associated with the presence of adenomas is a factor closely linked to the development of malignant neoplasm. The chances of cure and survival of such cancer are high when detected at an early stage. The management of adenomas has an important role in the prevention of colorectal cancer, making it necessary to conduct studies to determine new prognostic factors related to its development and progression. The cell cycle is controlled by several genes, the main function of these genes is the synthesis of proteins that promote perfectly organized cell proliferation, and the other genes that suppress the proliferation.
2. Incidence of colon cancer
Carcinoma of the large intestine is common in Northwest Europe, North America, and other Anglo-Saxon areas and low in Africa, Asia, and some parts of South America [6, 7].
In Portugal for example, CRC is the second most common type of cancer, in both men and women. In 2008, it was responsible for 18.7% and 15.1%, respectively, of all cancer in Portugal [8]. Regarding mortality, unlike European data [9], there was an average increase of 3% from 2000 to 2005 [10], in 2012, incidence and mortality rates are higher than European rates [11].
In the United States, it is by far the most common and most curable carcinoma of the gastrointestinal tract. There is some evidence of a further increase in its occurrence, particularly in young blacks [12]. Males and females are affected equally. The mean age of incidence is about 60 years [13, 14].
3. Risk factors
One specific cause for colon cancer has not been identified. However, the aetiological and pathogenesis of colorectal cancer is usually related to both environmental and genetic factors [15, 16]. The former is largely dietary, particularly in terms of fast animal protein and fatty food they are related to their influence on the intestinal microflora and ultimately on the chemical composition of the intraluminal content [17, 18].
The relationship between epithelial polyps and colorectal carcinoma and the sequence of molecular alterations that have been detected in these lesions have already been recognized. Patients with inflammatory bowel disease (such as ulcerative colitis) have a definite predisposition to colorectal carcinoma, [19, 20] however they consist only a small fraction of the colonic cancer patients in the general population. Polyps of juvenile and/or adenomatous type can also occur at this juncture [21, 22]. Interestingly, these changes are preceded by abnormal colonic mucin secretion [23].
3.1. Family history and genetics:
Although the aetiology of colon cancer is not fully understood, many studies have been done on the effects of family history and inherited mutation. Up to 10% of colon cancers have been found to have genetic predisposition, some genetic syndromes transmitted in the family from generation to generation can increase the risk of colon cancer. They are also responsible for 5% of case. One of these syndromes is called adenomatous polyposis coli, which is rare and characterized by presence of thousands adenomatous polyps within the rectum and on the intestinal walls [24].
3.2. Environmental factors:
The most well-defined environmental risk is exposure to ionizing radiation. Some cases of colorectal carcinomas have been seen as a late complication of pelvic irradiation of cervical carcinoma [19].
3.3. Medical history:
If the patient has colon cancer or benign glandular tumors before, he is more likely to have colon or rectal cancer.
3.4. Alcohol consumption:
The excessive use of alcohol is an important factor in the increased risk of colon cancer
3.5. Age:
The majority of people with colon cancer are 60 years old. Young people can also develop colorectal cancer, but their incidence is very low in these cases.
3.6. Inflammatory bowel diseases:
Ulcerative colitis and Crohn's disease; are example of inflammatory bowel diseases their presence increases the risk of colon cancer.
3.7. Diet:
High-fat diets, calories, or low fibres foods may be a cause of colon or rectal cancer.
3.8. Physical Activity:
Physical activity plays an important role in maintaining the body's organs. It also helps maintain muscle activity and bone health. It helps the body to get rid of harmful substances and stimulates it to resist diseases such as cancer or internal infections. It also protects the body from obesity, which is another cause of colon cancer.
3.9. Growth hormone disorders:
an imbalance in the growth hormone produced by the pituitary gland. This imbalance may be due to a defect in the work of the gland, which adversely affects the growth of the body organs properly, and thus increase the risk of various diseases, including colon cancer.
3.10. Diabetes:
People with diabetes are more likely to develop colon cancer.
3.11. Smoking:
People who smoke in large quantities are more likely to develop colon cancer, because the accumulation of nicotine in the body turns over days to cancers, including to colon cancer.
3.12. Geographic differences:
There is a big variation in age adjusted incidence rate for colon cancer seen among countries. Carcinoma of the large intestine is common in Northwest Europe, North America, and other Anglo-Saxon areas and low in Africa, Asia, and some parts of South America [6, 7]. In the United States, it is by far the most common and most curable carcinoma of the gastrointestinal trac
4. Diagnosis of colon cancer
One of the best methods for detection of colon cancer is a screening program with blood in stool, routine physical and endoscopic examination [25].
4.1. Screening for colon cancer by endoscopy
Screening means the use of investigations on asymptomatic persons, to detect the disease at an early stage in order to lower the risk of death, or complications of therapy [26].
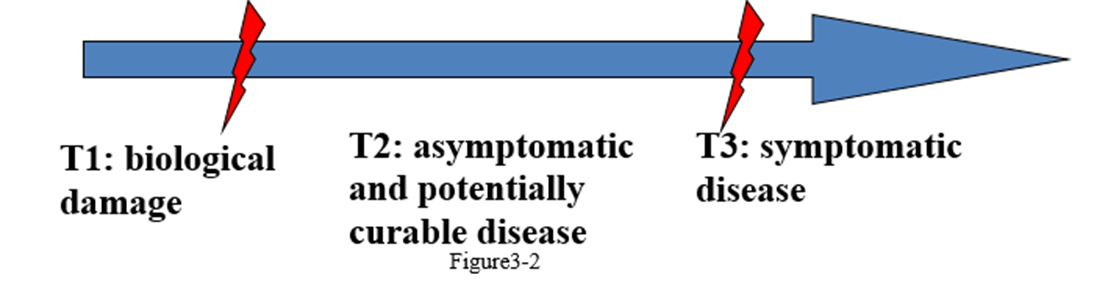
Figure 1: Hutchinson Diagram
Screening program should begin by classifying the individual patient level of risk based on personal, family, and medical history, which will determine the appropriate approach to screening in that person [27]. For example the person who is on risks such as following:
Personal history of adenomas or CRC, family history of CRC or adenomas in first degree relative (s) before age 60 years, inflammatory bowel disease (IBD), and family history of hereditary syndromes [24].
In addition to average risky person such as: healthy people with no known risk factors other than age, In general, practical guidelines recommend starting screening at age 50 years [28,29]. Because only 38% of patients are diagnosed when the cancers are localized to the bowel wall, it is likely that widespread implementation of screening could significantly improve the outcome. Colorectal cancer screening is cost effective, irrespective of the methods used. In addition to currently available methods (fecal occult blood, flexible sigmoidoscopy, colonoscopy, and double contrast barium enema). There are further experimental methods for screening are Fecal DNA test and computed topographic colonography (virtual colonoscopy) [30,31].
4.2. Clinical examination
The usual clinical picture of an early colorectal cancer is a change of bowel habit and painless mild bleeding particularly in the left side tumors. Other less common clinical features of colorectal cancer are; constipation with penciled like stool and signs of intestinal obstruction, ulceration with signs of intestinal perforation [32].
Systemic complaints like fatigue, cough, anemia, ascites, or musculoskeletal discomfort, may also present During palpation, oddly shaped, hard lump that can be felt might also be sings for cancer [33].
4.3. Colon biopsies (endoscopic biopsy and open biopsy)
A positive biopsy should always be obtained from colorectal carcinoma before performing radical surgery. In large lesions, it is advisable to perform several biopsies from different regions. Those biopsies which are taken from the center may show only granulation tissue, and those which are taken from the very periphery may contain only hyperplastic (so-called-transitional) colonic epithelium. Lesions below the peritoneal reflection should be removed in to wherever possible to facilitate their orientation for section by the pathologist. Although most adenocarcinomas are easily diagnosed, the main problems being presented by the well differentiated tumors and- the highly malignant signet ring carcinomas in which only a few tumor cells may by present [30].
43.1. Endoscopy biopsy
The endoscopic tissue biopsies are usually with size about of 3x1 mm, and the biopsy can be performed under local anesthesia. The endoscopic biopsy allows the diagnosis as well as the distinction between invasive and in situ cancer. However, both false positives and negatives can occur. It is also very helpful in the differential diagnosis of adenomatous polyp, and hyperplastic polyp or from cancer, but examiner experience is highly required to properly performing this task. Increased utilization of endoscopic biopsy for obtaining tissue samples has led to major advances in both detection and diagnosis [30].
4.3.2. Open biopsy
The proper diagnostic procedure for patients with suspected colon cancer is the open excisional biopsy of the mass. Generally, this often applied to benign lesions that the patient wants be removed, and also to removal of doubtful lesions, if a malignancy has not been demonstrated by endoscopic biopsy. When the lesion is still suspected to be cancer, or if a mass is likely to be malignant, and the biological makeup of the tumor seems to be abnormal, the biopsy can be examined as a frozen section by the pathologist for a quick, but preliminary diagnosis. More commonly, the biopsy is processed routinely, and a diagnosis is made. If a malignancy is found within the cancer cases [30].
5. Classical clinicopathological prognostic markers
For CRC, the pathologic clinical stage is currently the single most important prognostic factor [1, 3, 34, 35], correlating with long-term survival [3, 36 ,37], although it does not fully predict individual clinical outcome [3, 37 , 38]. This is particularly true for those tumours with intermediate stage disease (T3-T4N0M0) [38], where one-third of patients with tumor-free lymph nodes have recurrences, and therefore adjuvant chemotherapy may be beneficial [39]. In this group, carcinoma cells are not detected in lymph nodes by conventional staging methods in 24% of patients. Therefore, the lymphatic staging is essential to improve treatment of these patients. Indeed one-third of the patients submitted to curative intent surgery die of local and/or distant tumor recurrence [49 , 3]. Abdominal lymph nodes (38%) are the second most frequent site of metastasis (38%), just after liver, which is, the organ that most frequently involved (38–60% of cases) and followed by the lung (38%) and the peritoneum (28%) [49, 35].
5.1. Tumor size
Although a correlation between size of the tumour and prognosis exists, there are too many exceptions for this to be a reliable prognostic indicator . Along the same lines, there is little relation between the size of the tumor and the incidence of nodal metastases [2].
5.2. Lymph node status
Lymph node involvement is inversely correlated with tumor survival rate. Once the tumor has spread to the lymph nodes, the 5-year survival rate drops sharply. The location and extent of lymph node involvement are also significant" Cures are very rare when nodes other than those in the immediate vicinity of the tumor are involved [42, 43] Involvement of tie apical node is a particularly ominous feature [44, 45]. The greater the number of lymph nodes involved the worse the prognosis in one study [46]. if more than 6 lymph nodes contained metastatic carcinoma" Less than 10% of the patients survival more than 5 years If more than 16 mesenteric lymph nodes contained carcinoma all patients died within the 5-year period. The former extent of involvement was not observed in carcinomas less than 2cm in greatest diameter and the latter extent of involvement was not observed in carcinomas less than 3cm in diameter, With in these parameters there was correlation between degree of lymph node involvement and size of tumor. it has been claimed that nodal micrometaslases detected only immunohistochemically or molecularly (with a RT – PCR technique for CEA) are also associated with a decreased survival [47,48].
5.3. Clinical staging
The practical clinical decision is dependent on summing the above basic features of a tumor by means of a staging system. American Joint Committee (AJC) on cancer staging has modified the TNM staging system that was proposed by the International Union Against Control of Cancer (IUAC) and based upon the size of tumor (T), degree of spread to lymph nodes (N) and systemic metastasis (M) at the time of diagnosis. The staging system goes from stage I to stage IV. Staging is regarded as the most important prognostic factor. As stage increases the prognosis deteriorates. For example; the 5 years survival in stage I colon cancer is more than 90% while patients with stage IV disease have very poor prognosis and a 5 years survival are less than 30% [49]
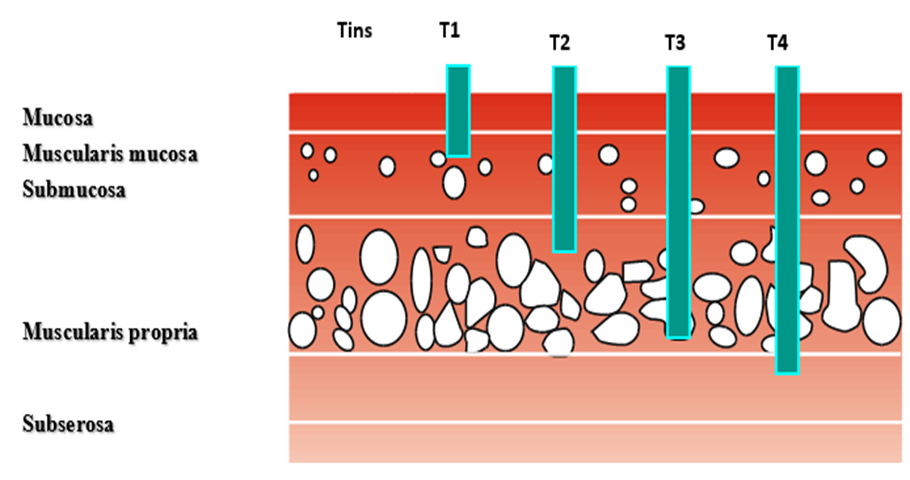
Figure 2: Layers of colon (Taylor, 2012)
6.1 Histological grade
Colon cancers can be graded according the degree of differentiation to well differentiated (grade I), Grading Adenocarcinomas are graded predominantly on the basis of the extent of glandular appearances, and should be divided into well, moderately and poorly differentiated, or into low-grade (encompassing well and moderately differentiated adenocarcinomas) and high-grade (including poorly differentiated adenocarcinomas and undifferentiated carcinomas). Poorly differentiated adenocarcinomas should show at least some gland formation or mucus production; tubules are typically irregularly folded and distorted. When a carcinoma has heterogeneity in differentiation, grading should be based on the least differentiated component, not including the leading front of invasion. Small foci of apparent poor differentiation are common at the advancing edge of tumours, but this feature is insufficient to classify the tumour as poorly differentiated [51]. The percentage of the tumour showing formation of gland-like structures can be used to define the grade. Well differentiated (grade 1) lesions exhibit glandular structures in > 95% of the tumour; moderately differentiated (grade 2) adenocarcinoma has50-95% glands; poorly differentiated (grade 3) adenocarcinoma has 5-50%; and undifferentiated (grade 4) carcinoma has < 5>
6.2 Mitotic activity
Several authors suggested that evaluation of mitotic activity alone can be as prognostic as the grading system or even more powerful [55,56]. There are many available ways to measure cell proliferative activity e.g. by counting the number of mitoses from ten high power fields from the most cellular area of the sample, using a standard light microscope (objective, x40; numeric aperture, 0.75; field diameter, 420µm), or by expressing the count by square millimeter, which produces the standardized mitotic index (SMI), also called volume fraction corrected mitotic index (M/Vv index) [56,57 ,55]. Many studies on different organs demonstrated that the mitotic activity index (MAI) is an independent prognostic factor for recurrence free survival. SMI is a bit more efficient than MAI as a prognosticator [57].
6.3 Histological type
Cancer at the site (CIS) consists of sever dysplasia. They are classified as pre-invasive cancers. In theory, it can be curable without any threat to life when surgically removed. Colorectal cancer and invasive adenocarcinomas have a slightly better prognosis than mucinous carcinoma [58].
6.4 Angiogenesis (Microvessel density)
Neo-vascularisation is the formation of new micro vessels in stroma. There is general agreement that angiogenesis has an important role in growth and metastasis of malignant tumors [14,25].
6.5 Tumor necrosis
Tumor necrosis is morphologically characterized by nuclear karyorrhexis, pyknosis and karyolysis, often accompanied by granular eosinophilic cytoplasm. When tumor necrosis has been present for a prolonged time it may be associated with fibrosis. Necrosis is usually related to adenocarcinoma of non-specific type, especially when has high grade [60]. A few studies suggested that tumor necrosis is accompanied with lowered survival and early treatment failure [58]. However, low reproducibility in evaluating necrosis may limit its use as a prognostic factor.
6.6 Multivariate clinicopathological prognostic indices
In last few years many authors combined different independent prognostic factors in multivariate indices in many organs including breast cancer and colon cancer. They found that these models are better prognostic indicators than the traditional grading system alone and can be expected to be more reproducible [61,58].
Typically, mitotic count has an important position in these models. It is important to notice that most multivariate models include lymph node status as a contributing feature and for that reason multivariate models or indices are applicable to both LN+ and LN- patients. One of the most common prognostic indices is Nottingham prognostic index which combines tumor size, lymph node status, and Nottingham histological grade [11].
6.7 Molecular prognostic markers in colon cancer.
A common feature of all cancers is the imbalance that exists between the proliferative activity and cell death; therefore, the evaluation of cell proliferation rate may be interesting in the study and characterization of tumors [63]. Some molecules, such as the Ki-67 protein, permit this assessment and are used as markers of proliferation because Ki67 expression is dependent of cell division rate; thus, over expression of these markers may suggest a disruption in the proliferation mechanism leading to the appearance of tumors [63].
Ki-67 protein, when used to evaluate the percentage of dividing cells, allows us to determine neoplastic growth [63] and has been documented to correlate with neoplastic progression [64] showing different levels of expression between normal mucosa, adenoma, and adenocarcinoma [65], verifying a progressive increasing of positive Ki-67 expression from the first (normal mucosa) to the last part of the tissue (adenocarcinoma) [64, 66 , 67].
Other studies correlate Ki-67 with the degree of malignancy, tumour invasiveness [67, 68], metastatic potential [63], patient survival, and the risk of relapse [69 ,70]. Thus, a high Ki-67 expression in tumour cells is assumed to correlate with a poor tumour differentiation and an increased tumor size [66, 68]. Micev et al. [71] demonstrated that there is an association between Ki-67 expression and a less effective response in patients undergoing chemotherapy.
Other correlations with clinical and pathological data were also investigated and a correlation was detected between a high expression of this protein and the following variables; Patient's age [67], tumor size [72], tumor localization [70], dysplasia degree [72], the presence of lymph node metastasis [63, 67 ,70], and TNM [67] and Dukes [70] classification.
Accordingly, the younger is the patient, the greater is the cellular proliferation and the lower is the degree of differentiation. With increasing malignancy a increased frequency of invasion and metastasis are observed and hence poor prognosis of the tumor [67].
6.7.1 p53.
The p53 gene is located on chromosome 17p13.1, and is encoded for p53 protein. p53 is thought to be the gate keeper in the cell cycle, also called the guardian of the genome. When active, the main function of p53 is to suppress cell proliferation and activate apoptosis. When DNA is damaged, p53 inhibits the evolution of the cell cycle from G1 to stage S and activates DNA repair genes. The cell is directed with irreversible DNA to apoptosis by activating the estrogenic genes [73,74 ,75]. Rational mutations in one allele of the p53 gene associated with congenital or acquired congenital loss of the other leads to continuous cell growth the later can promote carcinogenesis in many organs, including colon, lung, and breast [75]. A p53 mutation increases the half-life of the non-functional p53 protein, accumulated in the cancer cell nucleus.
The accumulated p53 protein can be identified with IHC [76]. p53 hyperplasia has been detected in many human cancers including breast cancer [76], [75].and is often associated with poor prognosis[77]. p53 mutations, which can be detected by DNA sequence, appear to be independent indicators [78] Allred and his group reported in 1993 that p53 predicted a disease-free survival in patients with colon cancer. However, it has been shown that the expression of mutated p53 protein is also associated with more aggressive tumors, including the early recurrence of disease and early death in colon cancer [79].
6.7.2 Bcl-2
Family of membrane proteins that control apoptosis. It has been stated that immunohistochemical expression of bc1-2 is associated with an improved prognosis [80].
6.7.3 Cell proliferation markers
A. MIB-1 (Ki-67)
Ki-67 is a cell proliferation marker. It is a non- histone DNA binding protein that can be detected by immunohistochemistry [81, 82]. It is expressed in all phases of cell cycle except the resting phase [81]. The Ki-67 positive cells are in preparing for the S phase. Ki-67 labeling index (fraction of Ki-67 positive nuclei of all cells nuclei) indicates the fraction of cells in proliferation or near S-phase in the cell cycle. Several authors detected that high Ki-67 labeling index correlate with high histological grade [83], and large tumor size of colon cancer [73]. Therefore, Ki67 when used to evaluate the percentage of dividing cells, allows us to determine neoplastic growth [63] and has been documented to correlate with neoplastic progression [64] showing different levels of expression between normal mucosa, adenoma, and adenocarcinoma [65], verifying a progressive increasing of positive Ki-67 expression from the first (normal mucosa) to the last part of the tissue (adenocarcinoma) [64, 66, 67].
Ki-67 labeling index (determined e.g. by the MIB1; IgG monoclonal antibody used for detection Ki-67 in paraffin embedded material) showed a significant adverse correlation with survival in colon cancer, particularly among patients without LN involvement [58]. However, the independent prognostic significance of MIB-1 is much less than that of mitotic count (as determined with either MAI or SMI [57,84]. The molecular classification of colon cancer based on gene expression profiling, The identification of several types of carcinoma of the large intestine has led to the discovery of some of the genetic alteration associated with (and presumably path-genetically responsible for) these tumors [85,186]. It was subsequently shown that somatic mutations of these genes also occur in sporadic colorectal cancer [87,88 89]. the most important of these genes are APC mismatch repair genes p53, k-ras and DCC [90].
In CRC, the analysis of colon adeno4mas has shown a different pattern for Ki-67 expression between normal tissue, adenomas, and adenocarcinomas. This was limited to the crypts in normal tissue and expressed both in the crypts and in the surface epithelium in adenomatous polyps e.g. (tubular, villous) [67], and distributed homogeneously in adenocarcinoma [92]. Nussrat et al. [72] also observed an increase in Ki-67 rates which was associated with the growth and rise of dysplasia in adenomas.
Studies on CRC indicated that Ki-67 is a prognostic marker since the survival rate for patients with high expression of Ki-67 is significantly lower compared to those with low expression [67, 93 94] and a predictor of CRC recurrence [95]. Also, significant associations were found between higher index of Ki-67 and increased tumour penetration [94, 96], the presence of lymph node [64, 94] and distant [94], metastasis, advanced TNM stage [92, 94], highest degree of differentiation, and subtypes of adenocarcinoma other than mucinous [97].However, not all studies were in agreement, and no correlations were found between patient age, gender, tumor location [64, 72, 93 98], and the type of adenoma [72] in some cases. Although, Jansson and Sun [98], did not find any associations between index Ki-67 and clinicopathological data or prognosis, Allegra and his group [99], described opposite associations, between a low rate of Ki-67 and high recurrence rate and poor overall survival. Regarding the use of Ki-67 in CRC metastasis, no full information is available, and the only similar study found compares Ki-67 index in primary tumour with peritoneal metastasis and had observed a lower proliferative index in metastasis compared with the primary tumor [100]. However, in other types of cancer, in particular breast cancer, a higher Ki-67 index was found in systemic and lymph node metastasis than in primary tumors [101 ,102], suggesting greater aggressiveness of these [102], it might be using of Ki-67 in lymph node metastasis in selecting the appropriate treatment for certain subgroups of patients [103].
6.7.4 Other molecular prognostic markers.
DNA mismatch repair deficiencies with resulting microsatellite instability MSI has been found to be an important alternate pathway present in approximately 15% of cases it operates in hereditary nonpolypsis colorectal carcinomas [104,105 ,106]. and is possibly a marker for the cancers arising from hyperplastic polyps and serrated adenomas [107].
Tumors associated with microsatellite instability tend to be mucinous or poorly differentiated with a prominent host response a circumscribed growth pattern and right-sided location in one study presence of tumor-infiltrating lymphocytes was found to be the best histological predictor of microsatellite instability [108,109]. it has been further pointed out that differences may exist depending on the specific type of mismatch repair gene involved [110].
Another group of molecules thought to play an important role in the pathogenesis of colorectal carcinomas is that of E-cadherin and catenins [110,111, 112] β-catenin is associated with APC protein and is dysregulated at all stages of the adenoma-carcinoma sequence [113,114] the expression of E-cadherin and α-catenin in colorectal carcinoma correlates with local invasion and metastases [115], mutations of p53 have been detected by molecular techniques in the majority of colorectal carcinomas [116]. E-cadherin and α-catenin have been correlated with an overexpression of the p53 protein that coded by the abnormal gene as detected immunohistochemically [109]. Approximately, half of the tumors showed positive staining of these proteins but do not seem to differ from others in terms of site of differentiation or DNA ploidy [117, 118]. As expected the (transitional) mucosa present between the edge of the carcinoma and the normal mucosa is uniformly negative for this marker [119].
Mutations of the rats oncogene have been found in a minority of colorectal carcinoma particularly those in the metastatic group. [120, 121] expression of this gene which is said to influence the morphogenesis of early cancers [105] can be detected immunohistochemically in histologic and cytogenetic preparations[123, 124] Deletion of the von Hippei-Lindau gene has been detected in a high proportion of colorectal adenocarcinoma cases [125]. An enhanced expression of the c-myc oncogene occurs in approximately 90% of colorectal carcinomas [126] The increased proliferative activity of colorectal carcinoma has been measured by S-phase determination staining for Ki-67 or PCNA.
It can be concluded that the colorectal cancer is one of the most common malignancies. The aetiological and pathogenesis of colorectal cancer are usually related to both environmental and genetic factors. The colorectal cancer risk factors are medical history, alcohol consumption, age, diet, physical activity, diabetes, smoking, and geographic differences. the best methods for detection of colon cancer is a screening program with blood in stool, routine physical and endoscopic examination. Classical prognostic markers in histopathology are histological grade, mitotic activity, histological type, angiogenesis, and tumor necrosis. With increasing malignancy an increased frequency of invasion and metastasis are observed. Rational mutations in one allele of the p53 gene associated with congenital leads to continuous cell growth the later can promote carcinogenesis in the colon. Tumor-infiltrating lymphocytes were found to be the best histological predictor of microsatellite instability. Further studies about colorectal cancer are needed to prove strategies for controlling the prevalence of the disease and the more accurate method for diagnosis.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
