
Case Report | DOI: https://doi.org/10.31579/2693-2156/075
Student at the Technological University of Pereira Pereira, Risaralda Department, Colômbia.
*Corresponding Author: Felipe Anduquia-Garay, Student at the Technological University of Pereira Pereira, Risaralda Department, Colômbia.
Citation: Felipe Anduquia-Garay, Yesica Cardona-Ríos, Paydieg Márquez, Dana Vargas, Cher Guzmán, et al., (2023), Colocutaneous Fistula after Gastrostomy Tube Replacement without an Endoscopic view of a Previous Percutaneous Endoscopic Gastrostomy: A Case Report, J Thoracic Disease and Cardiothoracic Surgery, 4(6); DOI:10.31579/2693-2156/075
Copyright: © 2023, Felipe Anduquia-Garay. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 29 December 2023 | Accepted: 08 January 2024 | Published: 16 January 2024
Keywords: heart transplantation; organ donor; primary graft failure; data base analysis
Background: Percutaneous endoscopic gastrostomy (PEG) has become a widely used technique to provide a safe, simple and inexpensive route for enteral nutrition. Despite the precautions, numbers of complications have been described in the literature. Complications after a procedure like bleeding, injury to internal organs, tumor seeding, infections, or gastrocolocutaneous can occur with rates that range between 0,4 - 22.5%.
Colocutaneous fistula is an unusual complication that can present as intractable diarrhea after feeding. A proper technique of PEG placement including transillumination and finger palpation are key preventive measures. The aim of our paper is to describe a case of a colocutaneous fistula after gastrostomy tube replacement without an endoscopic view of a previous PEG. Our case shows the importance of endoscopic vision for gastrostomy tube replacement.
Percutaneous endoscopic gastrostomy (PEG) has become a widely used technique to provide a safe, simple and inexpensive route for enteral nutrition. Despite the precautions, numbers of complications have been described in the literature. Complications after a procedure like bleeding, injury to internal organs, tumor seeding, infections, or gastrocolocutaneous can occur with rates that range between 0,4 - 22.5% [1].
Colocutaneous fistula is an unusual complication that can present as intractable diarrhea after feeding. A proper technique of PEG placement including transillumination and finger palpation are key preventive measures [2]. The aim of our paper is to describe a case of a colocutaneous fistula after gastrostomy tube replacement without an endoscopic view of a previous PEG. Our case shows the importance of endoscopic vision for gastrostomy tube replacement.
An 88-year-old man with a history of ischemic stroke 7 years ago, convulsive syndrome, atrial fibrillation and chronic kidney disease, had a PEG tube inserted at our clinic 6 months before for enteral nutrition without any complications.
The gastrostomy tube was functional and useful for those 6 months for feeding and medication administration, at which time a tube replacement was performed without an endoscopic view in an external hospital.
The patient was admitted twelve days later in the emergency room with several episodes of diarrhea and abdominal pain. Abdomen exploration was unreliable, with a normal white blood cells count, a low serum albumin/protein levels and a stool sample incompatible with infection.
After evidence of a persistent intractable and white colored diarrhea, the gastroenterology and surgery teams were consulted, who decided to perform an upper endoscopy with an absent gastrostomy tube in the stomach. Figure 1.

Figure 1: Absent gastrostomy tube in the stomach.
Colocutaneous fistula was diagnosed and the patient underwent a laparotomy. At the time of surgery, no injuries or signs of previous connection with the stomach were seen and PEG was located into the transverse colon. Figure 2. The colocutaneous fistula was excised, the colonic hole was closed, and a regular open gastrostomy performed without any complications. Figure 3. The patient was discharged 5 days after the procedure with an uneventful postoperative course.
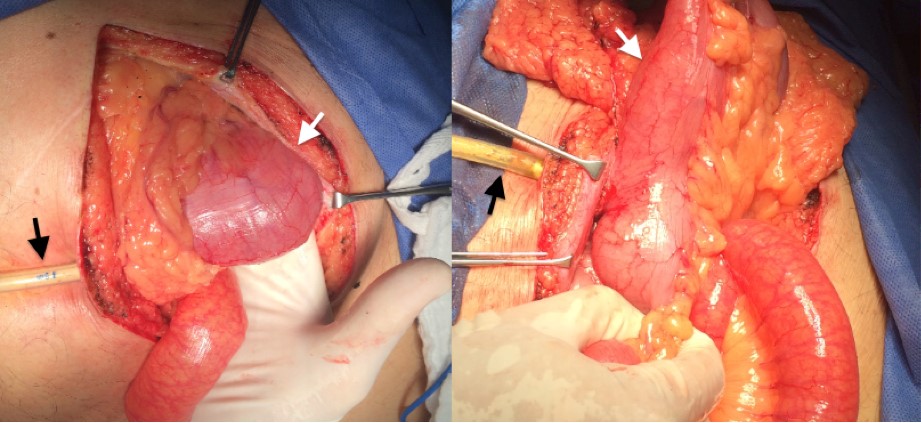
Figure 2: PEG was located into the transverse colon.
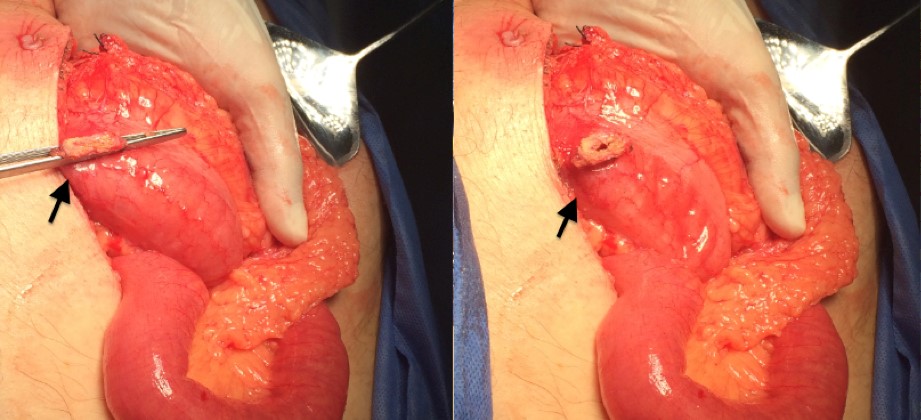
Figure 3: Regular open gastrostomy performed.
Percutaneous endoscopic gastrostomy is an effective, simple, inexpensive and widely used procedure to provide a safe route for enteral feeding. First introduced by Ponsky and Gauderer in 1980, the gastrostomy tube can be used in different types of acute and chronic diseases associated with malnutrition and/or swallowing disorders [1].
Despite the precautions and using a proper technique, complications are described, generally minor with peristomal infection being the most common and easily manageable, with low rates that range between 13–43% and major complications that do not exceed 22%. Complications mainly occur in elderly, multi- pathological, malnourished patients and those with a history of bronchospasm or infections. Furthermore, the technique has a very low mortality rate (0–2%), although this percentage increases at 30 days (6.7–26%), especially in patients with cardiovascular comorbidities. [1].
Colocutaneous fistula is a rare complication that occurs as a result of the interposition of the colon between the anterior abdominal and gastric wall, it may present as intractable diarrhea after feeding (watery or white colored diarrhea), abdominal pain, fecal leakage around the tube and other symptoms (upper gastrointestinal symptoms) [3]. In some patients as reported in the literature, symptoms can start soon after the tube replacement [4].
Our patient had some risk factors for PEG related complications as reported by Lucendo et al [5]. as being older than 75 years old, malnutrition (low serum albumin levels) and multiple comorbidities (coexistence of congestive heart failure, renal failure, urinary tract infection, previous aspiration, chronic pulmonary disease, coagulopathy, circulation disorders, metastatic cancer, and liver disease). Another risk factor reported in the literature is the presence of infection, demonstrated with a high C-reactive protein levels and abnormal leukocyte counts [5]. but our patient didn’t meet these criteria.
Complications can be minimized when using a proper technique during the procedure, the reasons for failure include an inappropriate transillumination or position (bed elevation up to 30 degrees), with inappropriate techniques (approximation of the gastric and abdominal walls) and unsafe tract (air return and endoscopic visualization of the needle). With the proper technique, the success rate ranges from 76% to 100% [5-6].
A CT scan, colonoscopy and a fistulogram can be useful to determine the location of the gastrostomy tube and to plan a surgical repair, with treatment options ranging from the conservative tube extraction to surgical management (exploratory laparotomy). The small number of cases reported in the literature makes it difficult to draw conclusions on the best treatment [7].
We were surprised to find that the stomach didn’t show evidence of perforation and that the gastric wall was completely intact, without any scare tissue, and we can speculate that the gastrostomy tube migrated to the colon probably secondary to a high tension.
In any case in our report, which is unique, it is difficult to determine if the gastrostomy tube migrated from the stomach to the colon after PEG or if it was a colon perforation after gastrostomy tube replacement without an endoscopic view. This case demonstrates the importance of: a) Using a proper technique during the procedure and b) Using an endoscopic view for gastrostomy tube replacement.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
