
Case Report | DOI: https://doi.org/10.31579/2694-0248/003
1 Shahid Beheshti University of Medical Sciences, Tehran, Iran
2 Joint, Bone, Connective tissue Rheumatology Research Center (JBCRC), Golestan University of Medical Sciences, Gorgan, Iran
3 Shahid Beheshti University of Medical Sciences, Tehran, Iran
*Corresponding Author: Seyyed-Mohsen Hosseininejad , Bone, Joint and Related Tissue Research Center, Shahid Beheshti University of Medical Sciences, Elahiyeh, Tehran, Iran.Email: hosseininejad.s.mohsen@gmail.com.
Citation: Seyyed-M Hosseininejad , Sahab-S Tabatabaei, Shabani S. (2020) Coincidence of Ipsilateral Humeral Shaft, Monteggia and Both Bone Fractures; A Floating Elbow with Significant Recovery. Clinical Orthopaedics and Trauma Care. 2(1); DOI:10.31579/2694-0248/003
Copyright: ©2020 Seyyed-M Hosseininejad, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 January 2020 | Accepted: 07 February 2020 | Published: 20 February 2020
Keywords: Monteggia ; bone forearm fracture ; floating elbow
The coincidence of forearm and humeral shaft fractures results in a “floating elbow” injury necessitating surgical open reduction and internal fixation of all fractures to allocate for maintenance of elbow joint suitable motion and minimizing stiffness. Here we introduce a case of an ipsilateral humeral shaft fracture and Monteggia and both bone fracture with terrible triad open fracture from a pedestrian car accident (PCA) to his right upper extremity.
The coincidence of forearm and humeral shaft fractures results in a “floating elbow” injury necessitating surgical open reduction and internal fixation of all fractures to allocate for maintenance of elbow joint suitable motion and minimizing stiffness [1]. Here we introduce a case of an ipsilateral humeral shaft fracture and Monteggia fracture with terrible triad open fracture from a pedestrian car accident (PCA) to his right upper extremity.
This is a rare devastating combination of injuries resulting in a floating elbow variation with interruption of the proximal radioulnar joint [2, 3]. A written informed consent was obtained from the patients regarding the data would be submitted for publication. and the patient agreed. A 40 year-old previously healthy man suffered a forceful twisting and loading injury to his right upper extremity which due to a PCA caused a large wound plus severe pain and deformity of his right arm, elbow and forearm. He was transferred by ambulance of Urban Emergency System to our emergency department.
On physical exam, he suffered an open fracture of Elbow, arm and forearm and neurovascular examination was not clearly intact. X-rays of the humerus, elbow, and forearm showed a right humeral shaft fracture and terrible triad open fracture besides Monteggia fracture (Figures 1). An interruption of the distal radioulnar joint could be considered as well.

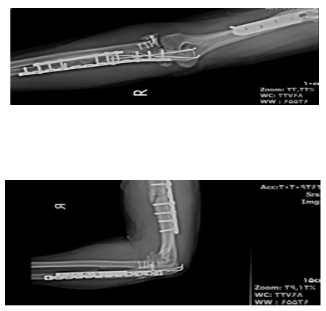
After stabilizing measures, he was prepared to transfer into the operating room. The operation was performed under general anesthesia. He was positioned on a radiolucent table in the lateral decubitus position with the right arm which was supported over a foam roller. The right upper extremity was then prepped and draped, preceding 2 grams of cefazolin injection. The wound was completely irrigated with 9 liters of Sterile Normal saline serum and the patient was scheduled for definite fixation in five days later, receiving cefazolin and gentamycin, in the mean time. Our case’s postoperative period was interesting. The splint was removed after 10 days postoperatively, and gentle elbow and passive range of motion exercises were started. At 3 month follow-up, radiographic study demonstrated healing of the humeral and ulna shaft fractures (Figures 2). At this time, elbow and forearm full active range of motion and strengthening exercises were performed for 6 weeks.

At follow-up 6 months follow up postoperatively, radiographs demonstrated healed wound and fixed elbow, humeral and forearm fractures in anatomic position with stable reduction of the distal radioulnar joint (Figures 3). The distal and proximal radioulnar joint was stable on examination. The patient is pain-free and had near full and acceptable range of motion (video file). The neurovascular condition was also recovered well.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
