
Research Article | DOI: https://doi.org/10.31579/2578-8868/147
*Corresponding Author: Mohammed A. Gomaa, Department of Otolaryngology, Minia faculty of Medicine at Minia University, Minia, Egypt.
Citation: Gomaa M A, Mamdouh H, khalaf Z, Abd El-hakeem WH, Zaky EA. (2021) Cognitive Impairment in Children with Adenotonsillar Hypertrophy. J. Neuroscience and Neurological Surgery. 8(1); DOI:10.31579/2578-8868/147
Copyright: © 2021 Mohammesd A. Gomaa, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 11 November 2020 | Accepted: 21 December 2020 | Published: 01 January 2021
Keywords: obstructive sleep apnea; adenotonsillectomy; cognition.
Pediatric OSA affects 1 to 3% of the population and appears to affect boys and girls equally [4]. The most commonly cause of pediatric OSA is adenotonsillar hypertrophy. Thus, the primary treatment is adenotonsillectomy. Pediatric OSA has been associated with some psychological problems, of which neurocognitive and depression , difficulties particularly in memory , attention, learning and executive function, are the most widely reported. The neurocognitive deficits is due to the adverse effects of sleep fragmentation and/or intermittent hypoxia .Scholastic performance have been reported in little studies of pediatric OSA, and such findings may underscore more extensive behavioral disturbances such as restlessness, aggressive behavior, excessive daytime sleepiness and poor test performances. The aim of this study was to evaluate the effect of adenotonsillectomy (AT), in children with Obstructive Sleep Apnea (OSA), on the cognitive and scholastic achievement.
Obstructive sleep apnea (OSA) in children is a breathing disorder that results in repeated and/or prolonged airway obstructions during sleep, in the form of apneas and hypopneas throughout the night [1]. The highest incidence of pediatric OSA occurs in early childhood [2], particularly between 2 and 8 years of age [3]. Pediatric OSA affects 1 to 3% of the population and appears to affect boys and girls equally [4]. The most [5] commonly cause of pediatric OSA is adenotonsillar hypertrophy. Thus, the primary treatment is adenotonsillectomy, which accounts for more than 500,000 procedures annually in the United States alone [5]. OSA is known as sleep-disordered breathing [6] (SDB). This spectrum ranges in severity from habitual snoring to upper airway resistance syndrome (UARS) to OSA. As OSA influence about one to three percent of pediatric population [6], it has been associated with some psychological problems, of which neurocognitive and depression , difficulties particularly in memory , attention, learning and executive function, are the most widely reported. The neurocognitive deficits is due to the adverse effects of sleep fragmentation and/or intermittent hypoxia [7]. Some studies have reported the presence of significantly reduced IQ scores compared with control children [8]. Scholastic performance have been reported in little studies of pediatric OSA, and such findings may underscore more extensive behavioral disturbances such as restlessness, aggressive behavior, excessive daytime sleepiness and poor test performances [9]. While Marcus et al. [10] pointed that the surgical treatment of pediatric OSA didn’t did not significantly improve attention or executive function as measured by neuropsychological testing but did reduce symptoms and improve secondary outcomes of behavior, quality of life, and polysomnographic findings, thus providing clues of beneficial effect of early AT.
The purpose of the present study is to evaluate the effect of adenotonsillectomy (AT) on the scholastic and cognitive achievement of children with OSAin order to establish a plan for proper management of those children.
Materials and Methods
The current study is a prospective one that done at the Department of Otorhinolaryngology from October 2016 to July 2019. It was approved by the Research ethics committee of the Faculty of Medicine, Minia University and signed informed consent was obtained from parents/ guardian of the children. One hundred Fifty children suffering from recurrent attacks of tonsillitis with or without chronic nasal obstruction were selected as pool for the present study. They were 73 males (48 %) and 77females (52%), with a mean age 101.5±15.6 of and a range of (72-120) months.
Inclusion criteria were as follows: (1) Children with age ranging (5-12) years. (2) Well diagnosed with obstructive sleep apnea (OSA) due to adenotonsillar hypertrophy.
The exclusion criteria were as follows: (1) Age below 5 years and above 12 years; (2) Children taking sleep (hypnotics) or neurobehavioral drugs; (3) Children with Previous adenotonsillectomy; (4) Children with craniofacial syndromes; (5) Children with hearing impairment (SNHL); (6) Obese children (Body Mass Index (BMI) ≥ 30).
All one hundred fifty children were subjected to the following protocol to classify the study and control groups
2-Auditory perceptual assessment (APA) of speech (degree of closed nasality). The speech of each case were assessed from two expert phoniatricians for the degree of closed nasality (From I to IV) after recording of the patient's speech for a nasal sentence [11].
3- (ENT) Examination Otolaryngological examination: Oral and oropharyngeal examination (lips, teeth, tongue, hard and soft palates, uvula, tonsillar pillars, tonsils, lateral and posterior pharyngeal walls) was examined by Otolaryngologist with a tongue blade and a good light. Then tonsillar hypertrophied were graded by Brodsky scale (From zero to 4) [5].
Examination of the nasopharynx through nasopharyngoscopy, for evaluation of the velopharyngeal area (velar mobility, lateral pharyngeal wall mobility, presence of adenoid and degree of narrowing the air column, type of closure, presence or absence of passivent's ridge).
4- Polysomonography PSG was performed using a digital polygraph system (Grass-Telefactor Twin version 2.6; Astro-Med Inc., West Warwick, RI, USA). The data were manually scored according to the American Academy of Sleep Medicine , Version 2.0 Berry et al., [11].polysomnography (PSG) study using standard clinical pediatric techniques and a commercially available sleep system for diagnosis of OSA. The current gold standard for the diagnosis of OSA, as recommended by the American Academy of Pediatrics (AAP), is a PSG study. Polysomnographic diagnostic criteria for OSA depends on the following parameters Apnea-Hypoapnea index (AHI) (represents the average number of obstructive or partially obstructive events per hour of sleep and considered abnormal if greater than 1 in children), a minimum oxygen saturation (less than 92 percent (average: 96 percent ± 2 percent) is considered abnormal in children).According to the inclusion criteria in table-2 we classified the patient to study group and control group [1].
We selected one hundred patients according to inclusion and exclusion criterias which were mentioned before , fifty child as study group with OSA that documented by PSG and fifty child suffer from chronic tonsillitis without OSA as a control group, . Both groups were subjected to protocol of evaluation the psycholinguistic abilities and IQ preoperatively as follow:
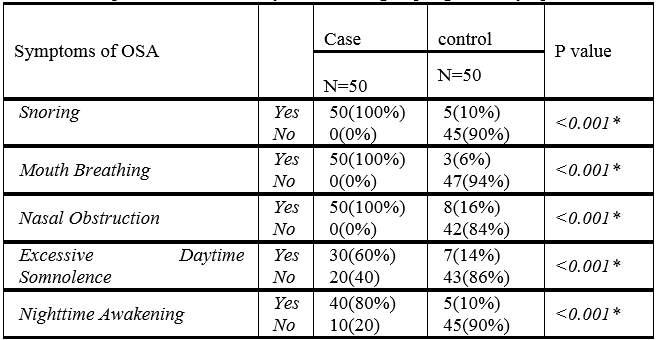
1-Parents interview and history including complaint, personal data, personal history, in addition to the clinical findings of prolonged upper airway obstructive symptoms, including OSA (recurrent episodes of apnea and hypopnea, secondary to collapse of the upper airways during sleep), snoring, mouth breathing, adenoid fancies, enuresis, and restlessness during sleep (if accompanied by snoring at night). History of arousal or awakening, and distrust sleep continuity.
2-Auditory perceptual assessment of speech (degree of closed nasality). The speech of each case were assessed from two experts for the degree of closed nasality after recording of the patient's speech for a nasal sentence [11].
3-Audiological evaluation included middle ear assessment through immitancemetry (Tympanometry and Acoustic Reflex threshold recording) and hearing assessment. According to the age of child. Hearing assessment was performed through one of the following methods: Free field audiometry and Behavioral Observational Audiomety (BOA).pure tone audiometry (Conditioned play or conventional audiometry).
4-Psychometric evaluation by Intelligence Quotient "IQ" using Stanford Binet Intelligence Scale (4th edition). The Stanford-Binet scale tests intelligence across four areas: verbal reasoning, quantitative reasoning, abstract /visual reasoning, and short-term memory. The areas are covered by 15 subtests. Raw scores were based on the number of items answered, and were converted into a standard age score corresponding to age group. Mental age was determined for each child: I.Q = Mental age chronological age ×100Gary [13].
5-Illinois test of psycholinguistic abilities (ITPA):
It is an individually administered battery of tests designed to measure the spoken and written language abilities of children aged 5-12 .it may be used for determining specific strengths and weakness among language abilities, for early identification of children at-risk for school failure.
It consists of twelve subtests Adel Aziz A et al., [14].
6-Percentage of the child's scores of his subjects (Academic performance) in two academic terms, which were obtained from academic reports taken from the school.
All patients (cases and control groups) underwent Adenotonsillectomy (AT) under general anesthesia. Then finally after eight months of adenotonsillectomy all the patients were followed by:
The data was collected from every battery of evaluation and subjected to I.B.M. compatible computer using software SPSS (Statistical Package for social science) for windows version 13 for statistical evaluation. Graphics were done by Excel. Quantitative data were presented by mean and standard deviation, while qualitative data were presented by frequency distribution. Wilcoxon signed-rank test for ordinal qualitative data between the two times: Significant level at P-value <
0.05. Paired samples T-test for parametric quantitative data between the two times: Significant level at P-value < 0.05. Pearson’s correlation: Significant level at P-value < 0.05. Spearman’s rho correlation. Significant level at P-value < 0.05 P-value was considered statistically significant (S) if <0.05 and highly significant (HS), if <0.001 and no significant (NS) if >0.05.
Results
The study group had age range between (7-10 years) and mean 8.8±14.6.They were 29 males and 21 females.
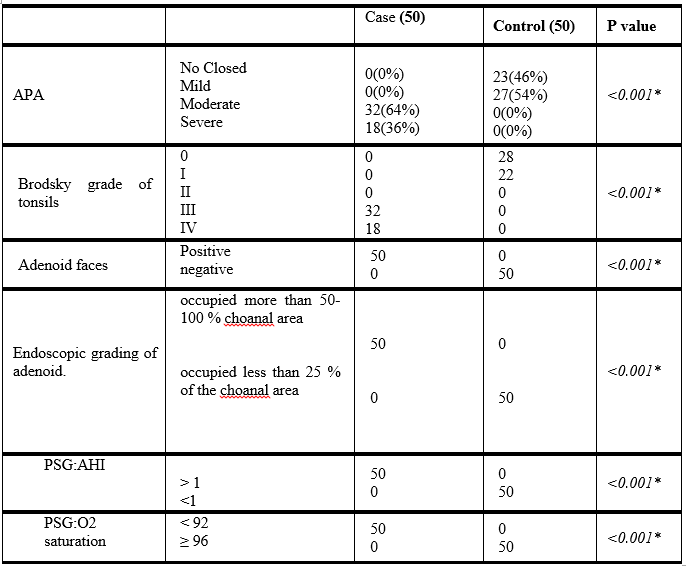
All patients in case group suffer from Moderate to severe closed nasality according to auditory perceptual assessment, Grade III to IV with tonsillar hypertrophied as measured by Brodsky scale, positive signs of Adenoid faces, Symptoms of OSA, the adenoid occupied 50-100 % of the choanal area. PSG of the study group revealed that Apnea-Hypopnea index (AHI) ˃ 1 and oxygen saturation less than 92 percent. The control group (children without OSA) included 50 children, they have mild closed nasality according to auditory perceptual assessment, Grade 0 to I of tonsillar hypertrophied with by Brodsky scale, negative signs of Adenoid faces, no Symptoms of OSA, the adenoid occupied less than 25 % choanal area and with the PSG the had Apnea-Hypopnea index (AHI) <1 and oxygen saturation more than ≥ 96 percent. The age of control group between (7-9 years) and mean 7.9±14.6.They were 26 male and 24 female (table 1-2).

Also, we found 30% of the children in the study group had type B tympanogram in comparison to 6% in the control group (table-5).

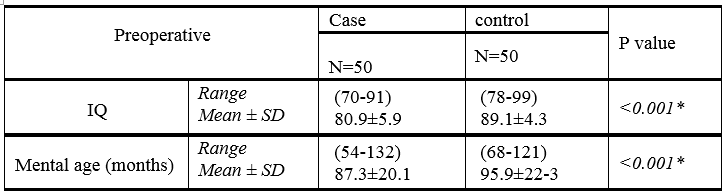
The children in the study group had low IQ and low mental age in comparison to the control group (table-6).
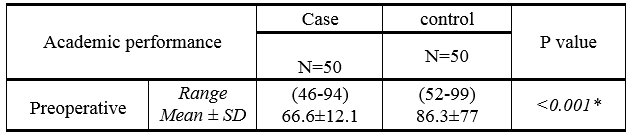
The children in the study group had low score in all subtest of Illinois test of psycholinguistic abilities (table-7) and had low percentile of academic performance in comparison to the control group (table-8).
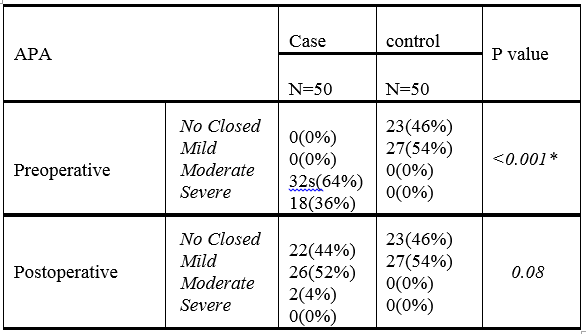
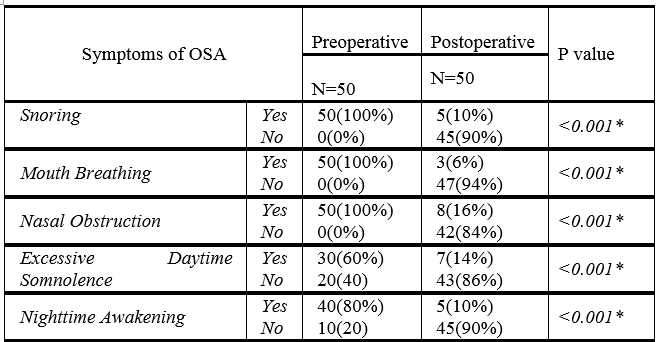
After eight months of adenotonsillectomy, the children in the study group had improvement in nasal tone of speech as 2% only has marked closed nasality (table-9) and most symptoms of OSA disappeared (table-10), only 8% had type B tympanogram (table-11).


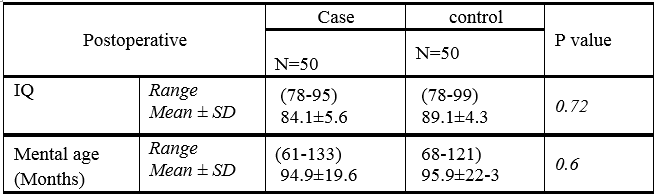
The results revealed no statistically significant difference were obtained between the two groups regarding the mental age, IQ (table-12), as well as subtest of Illinois test of psycholinguistic abilities (table-13). Also, our data showed improvement in percentile of academic performances of the study group in comparison to the control group (table-14).


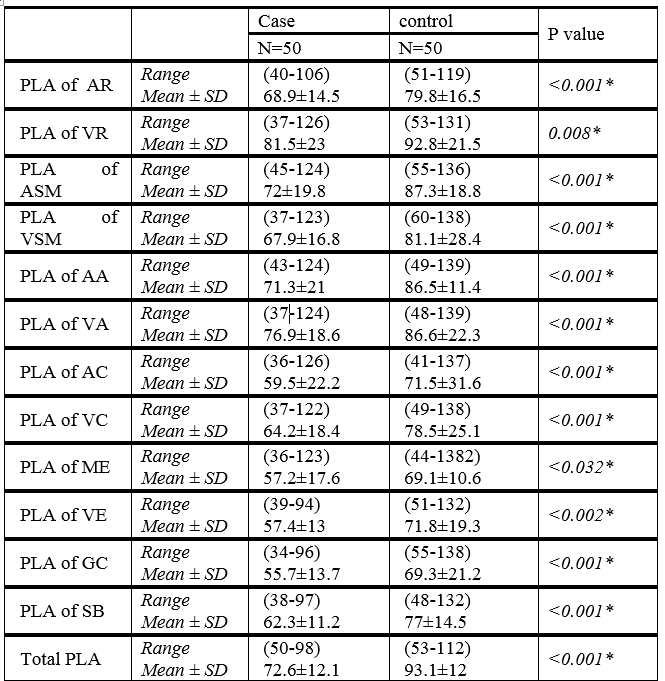
Our results showed that, there were a Statistical significant differences between preoperative and postoperative results of the study group in the following parameters, the PLA of AR (auditory reception), VR (visual reception), auditory sequential memory, VE (Visual Expression), ME (Mental Expression) as p<0.05). Also, Statistically significant differences were obtained between the preoperative and postoperative of the study group concerning the PLA of VSM (Visual sequential memory), AA (Auditory association) VA (Visual association), AC (Auditory closure), VC (Visual closure), GC (Grammatical closure) and SB (Sound Blending) as p<0.001). The current study pointed out that a statistically significant differences were obtained between the preoperative and postoperative results of the study group in the the Total PLA. (p<0.001). The mean Total PLA in the preoperative examination of the study group were 72.6±12.1 with a range (50-98) months, and the mean Total PLA in the postoperative data of the study group were 83.1±12 with a range (50-98) months (Table-15).

A Statistical significant differences were obtained between the preoperative and postoperative results of the study group as regard Academic performance. (p<0.05). The mean Academic performance in the preoperative examination of the study group were 66.6±12.1 with a range (46-70) percentage, and the mean Total row score in the postoperative examination of the study group were 83.1±12 with a range (60-98) percentage (Table-16).

In children, OSA is a disorder characterized by repeated and/or prolonged airway obstructions during sleep, in the form of apneas and hypopneas throughout the night [1]. OSAS exhibits specific cognitive dysfunctions that include deficits in memory, problem-solving, and behavioral functioning [14-15]. This is problematic, as SDB with AHI < 1 can still impact children's academic performance and behavior [16]. Friedman et al. [17] reported that young children who snore frequently and loudly during sleep are at greater risk for poor academic performance in later years, even well after snoring has resolved, suggests that the neurocognitive deficits may be only partially reversible after treatment. AT results in significant improvement in clinical as well as polysomnography parameters. Improvement in learning and behavior has been reported following the treatment of OSAS in children. The purpose of our present study was to evaluate the effect of AT on the academic and cognitive achievement of children with OSA so proper management of those children can be established. The study group included 50 children well diagnosed as OSA due to adenotonsillar hypertrophy confirmed by polysomnography compared to another control group of 50 children without symptoms of OSA.
The study group reported nighttime symptoms, including mouth breathing, apneic episodes, frequent awakenings, and restlessness. Children also had enuresis, behavior problems, deficient attention span, and daytime somnolence. The study group improved most of OSAS symptoms post AT, and this attributed to the removal of the upper airway obstruction. 60% of patients in our study had a severe degree of hyponasal speech, and 40% had a moderate degree of hyponasal speech pre-AT, but 8 months post AT only 4 % of the patients had moderate hyponasal speech, and 12 % had a mild degree of hyponasal speech. This improvement of the auditory perceptual assessment can be attributed to the removal of the obstructive effect of adenoid on the choana, i.e., get rid of the anatomic and physiological factors that constrict the space of nasopharynx and compromising the soft tissues surrounding the pharynx that predispose to upper airway collapse and change in normal resonance of the vocal tract.
Cognition is a mental act that includes perception, reasoning, awareness, and intuition. Executive function encompasses the mental processes that enable children to plan, focus, remember instructions, and juggle multiple tasks successfully.
Psycholinguistics evaluations were carried out before and after AT for our patients revealed a significant difference between children in the study and the control group. The mean IQ of children in our study was increasing from 80.9±5.9 (pre AT) to 84.1±5.6 (post AT). Our result revealed a negative significant correlation between AHI and IQ, of the study group (p<0.001). This improvement of IQ in our patients with OSA can be attributed to the improvement of the upper airway obstruction during sleep, disappearance of intermittent hypoxemia, improvement of ventilation, and enough hours of a deep sleep. Eight months post AT considered enough duration to raise intellectual functions, so improvement in IQ was detected. These results match most of the published data about the improvement of IQ after AT in children with OSA. As Friedman et al., [17] conducted a prospective study to evaluate neurocognitive functions of children with OSAS, before and after AT, he found that six to ten months after adenotonsillectomy, the children with OSAS demonstrated significant improvement in sleep characteristics, as well as in daytime behavior, and their neurocognitive performance improved considerably in most tests conducted. However, on the other side Abd-Allatif et al. [18] in their study stated that the intelligent quotient (IQ) as an indicative parameter of neurocognitive function in children with adenoid hypertrophy not improved with adenoidectomy and there is no relation between adenoid hypertrophy and IQ. Taylor et al. [19] stated that significant improvement in the NESPY Auditory attention and response set of children with OSA seven months after early AT Children with primary snoring, as well as those with OSA, are at higher risk for deficits in attention compared to control children when measured on parental report scales, and that such deficits are substantially improved following treatment with AT [9].
The mean PLA of Auditory association, visual association, auditory closure, visual closure, and manual expression, were raised 8 months after AT. This wide improvement in neurocognitive functions was attributed to the correction of the obstructive symptoms, improvement of sleep disruption, intermittent hypoxemia and inattention after AT, and in turn the improvement of the neurocognitive function as well as the intellectual functions demonstrated from the results of the IQ. We think that normal language development in children is such an important factor in acquisition of reading and writing skills. Most children with OSA had a history of delayed language development during their early life. Phonetic sounds are acquired between ages 3–7 years, which is also the peak age for hypertrophy of the tonsils and childhood OSA. Our results matched to Correa et al., [20] who stated that the late diagnosis and treatment of OSA is associated with a delay in verbal skill acquisition.
The study that done by Marcus et al, [10] it evaluate the difference between adenotonsillectomy and wait and watch policy for management of OSAS, the study was randomized, multicenter and controlled trial. It measures cognitive, Polysomnography and behavioral patterns, At baseline and seven months after AT, they found that As compared with a strategy of watchful waiting, surgical treatment for OSAS in school-age children did not significantly improve executive function or attention when measured by neuropsychological testing but did reduce symptoms and improve secondary outcomes of behavior, quality of life, and polysomnographic findings, thus providing evidence of beneficial effects of early AT.
we found that children with OSA due to adenotonsillar hypertrophy had poor academic achievement owing to obstructive symptoms of upper respiratory tract but eight months post adenotonsillectomy there were improvement of 12 points of Illinois test in the Mental Processing and increasing in the academic performance also Parents of our children noticed that their children became more attentive and slept better without snoring, less impulsive and hyperactive.
The diagnosis and treatment of OSA should be emphasized, not only because of the possible implications for oral language, as demonstrated in the reviewed studies, which tend to worsen as the chronological age increases but also for the benefits in neurocognitive performance and quality of life. Weber et al. [21] stated that OSA children show a higher frequency of disorders of receptive and expressive language skills, mostly under diagnosed and thus not treated. A more multi-disciplinary investigation of OSA children is needed to foster the evidence. In current study, there were increase in the score of PLA of VE (Verbal Expression) and grammatical closure. This improvement can be attributed to children with OSA due to adenotonsillar hypertrophy and Eustachian tube dysfunction, positive middle ear pressure, middle ear fluid accumulation, conductive hearing loss, all these causes impaired language acquisition, causing impairment in language development (semantic, syntactic, phonological and pragmatic development).
Ikedia et al [22] reported that to assess whether tonsillectomy and AT surgeries would bring benefits as far as school performance is concerned in children with OSA, psychological evaluations were carried out before and after the surgery. Gozal& Pope [22] investigated 300 children with the worst grades in a school, 18.1% of them had gas-exchange (O2 and CO2) disorders during sleep. Of those with obstructive sleep disorders, half were submitted to adenoidectomy. They noticed that the group submitted to adenoidectomy had a significant increase in school performance. The other half, without disorders, kept their mean scores. AT is effective in treating breathing problems in most children with OSAS and also appears to help improve their academic and intellectual performance and general behavior [17].
In the current study, eight months post AT, the mean Academic performance was increasing from (post AT) in comparison to the control group. This improvement was demonstrated from increasing in the scores of the children' school subjects also from the results of the tests carried out (Stanford Binet Intelligence Scale and Illinois tests). Parents / guardian of the study group noticed that their children became more attentive, no snoring, sleep better, less hyperactive and less impulsive All these changes will Benefit the entire family. The improvement in the previous parameters attributed to correction of frequent arousals during sleep, intermittent nocturnal hypoxia, anxiety, impulsivity, deficits in emotional regulation, alertness, inattentive behaviors, And attention to tasks after removal of Adenoid and tonsils that obstruct upper airway. This correction leads to improvement in the memory and IQ, resulting in an increase in academic performance. The improvement of language expression,, which was impaired in the Illinois subsets, after surgical correction of OSA, This correction lead to increase in the mean age of the verbal expression, grammatical closure and sound blending subtests of Illinois test After eight months post AT than pre AT.
Language is a very important factor for good academic achievement so this important finding can help in the prediction of poor academic achievement or learning disabilities through appreciation of language impairment; also we raise attention to the importance of early detection or screening for language impairment in children in the hope of preventing possible late severe learning disabilities. This study (up to our knowledge) is the first study to use Illinois test to determine specific strengths and weaknesses among language abilities, for early identification of children at-risk for school failure. An improvement of 12 points of Illinois’ test in the Mental Processing following AT is a very substantial improvement. This change enables the children to reach their original abilities and fulfill their cognitive potential. Cognitive factors such as memory, attention, intellectual and school performance improved significantly after AT. Visual and auditory short-term memory, as well as the ability to solve problems and to think analytically improved. These findings suggest that OSAS is a reversible disruptive factor to the neurocognitive function and school performance of children, at least in the short term (8 months after therapy).
The study was approved by the research ethics committee of the Faculty of Medicine and in agreement with Helsinki declaration. Informed signed consent is taken from the parents/ guardian of the children.
Conflict of interest: None
Funding: None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
