
Research Article | DOI: https://doi.org/10.31579/2637-8892/234
Department of Pharmacology, Anand College of Pharmacy, Sharda University, Agra-282007, India
*Corresponding Author: Kashmira J. Gohil, Department of Pharmacology, Anand College of Pharmacy, Sharda University, Agra-282007, India.
Citation: Roshan sah., Manish Pal Singh., Kashmira J. Gohil, (2023), Cognitive Guardians: Exploring Flavonoids as Potential Therapeutic Agents in Alzheimer’s Disease Treatment, Psychology and Mental Health Care, 7(6): DOI:10.31579/2637-8892/234
Copyright: © 2023, Kashmira J. Gohil, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 September 2023 | Accepted: 26 September 2023 | Published: 04 October 2023
Keywords: alzheimer's disease; presenilin; apolipoprotein e;neurofibrillary tangles
Alzheimer's Disease (AD) is a devastating neurodegenerative disorder characterized by progressive cognitive decline. With no cure in sight, there is an urgent need to identify novel therapeutic strategies. This abstract summarizes the emerging research on the potential of flavonoids, a class of natural compounds found in various fruits, vegetables, and beverages, as promising agents for AD treatment. Flavonoids have gained attention due to their antioxidant and anti-inflammatory properties, both of which play crucial roles in AD pathogenesis. This review examines the accumulating evidence suggesting that flavonoids may exert neuroprotective effects through multiple mechanisms. Flavonoids demonstrate the ability to enhance synaptic plasticity and promote neurogenesis, crucial processes for memory and learning, which are severely impaired in AD. These compounds show promising effect in reducing the accumulation of amyloid-beta plaques and tau tangles, the pathological hallmarks of AD. Furthermore, their potent antioxidant capabilities help combat oxidative stress, a hallmark of AD, by neutralizing harmful free radicals and also, flavonoids modulate inflammatory pathways, reducing neuroinflammation and its detrimental effects on the brain. This abstract provides an overview of preclinical studies and epidemiological evidence supporting the potential of flavonoids in preventing or slowing the progression of AD. Additionally, it discusses challenges in translating these findings into clinical practice, including issues related to bioavailability and standardization of flavonoid-rich interventions. In conclusion, flavonoids represent a promising avenue in the search for therapeutic agents against Alzheimer's Disease. Their multifaceted neuroprotective properties make them attractive candidates for further investigation and potential inclusion in future AD treatment strategies. However, more rigorous research, including well-designed pre-clinical and clinical trials, is necessary to establish their efficacy and safety in AD patients.
NFTs - amyloid plaques and neurofibrillary tangles
Aβ - amyloid peptideβ
AD - Alzheimer's disease
PS – Presenilin
APP - Amyloid precursor protein
ApoE- Apolipoprotein E
NFTs - neurofibrillary tangles
MCI - mild cognitive impairment
PPARγ - Peroxisome proliferator-activator receptor-γ
GPx - Glutathione peroxidase
Erk - Extracellular regulated kinase
AMPK - AMP- activated protein kinase
GSK3β – Glycogen synthase kinase-3β
Cdk-5 – Cyclin-dependent kinase-5
PP2A – Protein phosphatase 2A
PGC-1α – Peroxisome proliferator-activated receptor-γ coactivator
GSHpx – Glutathione peroxidase
Er-α - Estrogen receptor-α
ACHE - Acetylcholinesterase
BCHE - Butyrylcholinesterase
GSH - Glutathione
NLRP3 – Nucleotide-binding oligomerization domain-like receptor pyrin domain-containing3
Around the world, there are at least 50 million people who have dementia. [1] This is expected to triple by 2050 as a result of longer life spans, yet there are still no treatments available to stop or delay the onset of dementia. Alzheimer's disease (AD), the most prevalent cause of dementia, is a neurodegenerative condition that is often characterised by the buildup of NFTs, which are brought on by tau aggregation and Aβ respectively. More recently, gliosis and chronic neuroinflammation have been added to the list of AD symptoms along with plaques and tangles. [2] One of the main challenges in halting the progression of AD, by the time it is clinical diagnosis, brain atrophy is already established and now pathogenic cascade are well established. Its complex pathology is characterised by a memory loss that often develops beyond the age of 60. Rarely, the symptomatology may appear between 40 and 50 years of age, in which case the disease advances quite quickly. [3] In most cases, the "familial" early-onset form of the disease is linked to particular mutations in the genes that code for PS1 and PS2 as well as APP, while occasional late-onset disease is linked to mutations in the gene that codes for ApoE and includes a number of environmental risk factors. [4] The extracellular Aβ deposits, which take the form of neuritic plaques, are the histopathological characteristics of AD. Aggregates of increased phosphorylation Tau protein make up intraneuronal NFTs. [5] Language, focus, and orientation problems that develop into motor problems and personality abnormalities are the hallmarks of the symptomatology, which has a significant negative influence on the general public's health and places a heavy load on the medical community. [6]
A number of medications have been chosen to treat the condition, but regrettably none of them alter the course of the disease; instead, they only provide milder management and temporary symptoms due to the diverse nature of the pathogenic targets involved in AD progression. [7] More research is required to fully characterise the element of danger that expose one to the advancement of AD and to find medications that can stop the disease's progression or protect against it. [8] In this regard, natural remedies and diet offer significant promise in preventing the onset of neurodegenerative illnesses. [9] In reality, using natural chemicals can be an excellent replacement medicine, unlike manufactured products, which have major negative effects. This review's objectives are to summarise the present level of knowledge regarding AD, the molecular targets that cause it to progress pathologically, as well as to emphasise the beneficial correlations that flavonoids may have for the prevention and treatment of AD.
According to the amyloid cascade hypothesis (ACH), the buildup of Aβ oligomers is what starts a chain reaction that results in neuroinflammation, tau-induced toxicity, synaptic dysfunction, and neuronal death. This hypothesis chain reaction is occurred in two ways such as non-amyloidogenic pathway and amyloidogenic pathway. [10] In the non-amyloidogenic pathway involves the splitting of APP by α-secretase between Lys16 and Leu17 in the Aβ domain, resulting in the production of a soluble N-terminal fragment (APPsα) and a membrane-bound C-terminal fragment, C83, which can be further broken down by γ-secretases to produce a soluble extracellular p3 peptide and prevent the formation of intact Aβ. In contrast to the non-amyloidogenic pathway, the amyloidogenic process involves the internalisation and delivery of APP to endosomes. The enzyme β-secretase cleaves APP during the processing of amyloidogenic APP, and producing both a membrane-bound C-terminal fragment (C99) and a soluble N-terminal fragment (APPsβ). [11] A set of enzymes called γ-secretase then breaks down C99 inside the membrane, releasing a cytoplasmic polypeptide called AICD (APP intracellular domain) at the luminal side and Aβ peptides. γ-secretase breaks down APP at different locations in the transmembrane domain, resulting in Aβ peptides with lengths ranging from 38 to 43 residues. (fig.1) According to the amyloid cascade hypothesis, the aberrant buildup of amyloidβ (Aβ) plaques in multiple parts of the brain that triggers neurodegeneration in AD. Numerous Aβ-targeting treatments have been developed on the basis of this theory, with the hope that by focusing on this early Aβ-accumulation, the ensuing harmful pathways can be prevented. [12] Unfortunately, therapies that directly target APP processing have failed in Phase III, most likely as a result of side effects. [13] Examples of these therapies include BACE1 inhibitors. Aducanumab, an Aβ-targeting antibody, is said to have met its primary endpoint, according to recent reports, however approaches to diminish aggregating forms of Aβ via antibody techniques have also had poor results. It is becoming more and more obvious that lowering Aβ levels in the brain is unlikely to have a meaningful clinical impact if administered at MCI stage or later. The protracted prodromal period of AD will probably necessitate the use of Aβ-targeting therapies from the onset and throughout in order to become most successful.[14] This restriction calls for a tactical change, either focusing on targets that better correlate with later stages of disease progression, like neuroinflammation or tau, or sticking with the current targets while putting the emphasis on biomarker development to improve the classification of patients for earlier treatment. Finding and validating safe and affordable lifestyle therapies that might be widely used throughout midlife to lower AD risk throughout the public is another strategy. (Figure 1)
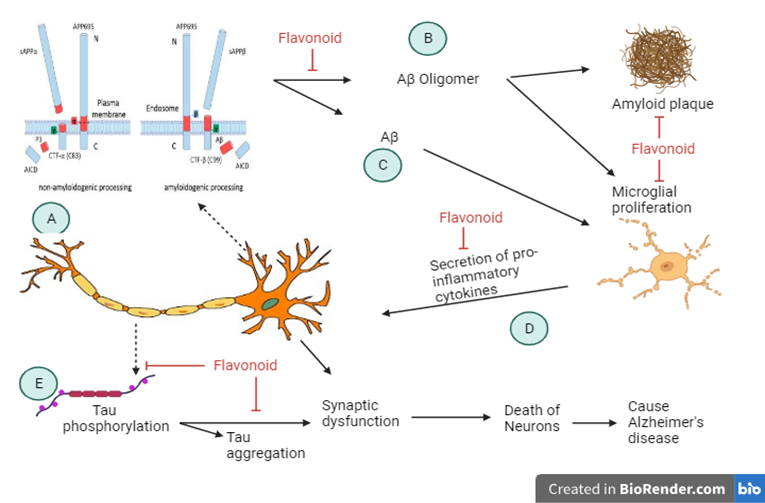
Figure 1: Mechanism of action of Alzheimer’s Disease.
Recent research has looked at the effectiveness of plant-derived natural substances in preventing AD. Fruits, nuts, and drinks are the main sources of the flavonoids and more than 6000 distinct flavonoids have been found. [15] Phenol has the capacity to pass the blood-brain barrier and has multitarget activity. Flavonoids have been shown in numerous studies to have biological effects as neuro anti-oxidants, as well as anti-amyloidogenic, metal-chelating, anti-inflammatory, and improvements in cognition and neuroprotection qualities. [17] According to epidemiological research, diets high in flavonoids are directly linked to a lower risk of dementia and the potential for improved symptoms in AD patients. Although there isn't any concrete evidence that flavonoid consumption lowers the risk of AD, only the epidemiological research indicate that flavonoid consumption may reduce the pathology of AD and improve symptoms. [18] Flavonoids can be categorised into six different groups: anthocyanidins, flavones, isoflavones, flavonols, flavanones, and flavan-3-ols (also known as flavanols). Although flavonoids are well-known for their antioxidant properties, it is also evident that they have the power to control intracellular reactions, primarily through altering protein-Kinase signalling pathways. [19] Furthermore, there is currently a lot of data in favour of flavonoids' potential to obstruct AD-related pathways. [20] But due to the high level of uncertainty surrounding absorption, metabolism, and fundamental drug kinetics, flavonoids have not yet been developed as treatment options for AD. With an emphasis on research where the potential for bioavailability of flavonoids has been seriously taken into account, growing mechanistic evidence supporting the modulation of AD pathways by flavonoid-mediated mechanisms is assessed in this review.
| S. No. | Dietary | Flavonoids | Model | Route of administration | Mechanism of action | References |
| 1. | Onion | Quercetin | Rats | Gastric intubation | Apoptosis. | 127 |
| 2. | Garlic root | Quercetin | Rats | Gastric intubation | Apoptosis. | 128 |
| 3. | Lactuca capensis | Catechin | Rats | Intraventricular | By altering the cholinergic response. | 129 |
| 4. | Hot peppers | Zeaxanthin | Rats | Intraperitoneally | By lowering the Aβ-peptide levels. | 130 |
| 5. | Orange’s peel | Naringenin | Rats | Orally | Stimulating Ache activity | 131 |
| 6. | Broccoli juice | Quercetin | Cellular model | Injectable | Triggering the Nrf2 signalling pathway | 132 |
Table 1: Dietary’s flavonoid in Alzheimer’s Disease
Several studies show that flavonoids can act as acetylcholinesterase (AChE) inhibitors but, as AChE inhibitors are only symptomatic interventions and not preventative or disease modifying. [21] But the study of flavonoids in AD mouse models has made significant strides in the last few years. The evaluation of these in vivo studies will primarily focus on those that used an oral route of phenolic treatment, in food or drink. A summary of the research that used oral means of delivery are presented in the table. 2 The processes are demonstrated by flavonoids through the pathophysiology of Aβ and tau, inflammation of the brain, oxidative stress, and neurogenesis. [2]
4.1 Flavonoid suppression of APP processing and Aβ accumulation
Both in vitro and in vivo studies have indicated that a number of flavonoids can improve Aβ pathogenesis such as- ECG, myricetin, genistein (Figure 1). This conclusion could be attributable to an increase in Aβ degradation, inhibition of aggregation, and a shift towards a non-amyloidogenic processing route.
Epigallocatechin gallate (EGCG): A widely researched catechin that is prevalent in tea, is a well-known illustration of a flavonoid-mediated blocking of APP synthesis. It has been demonstrated in vitro that EGCG increases the ratio of mature ADAM10 (mADAM10) to pro-ADAM10 in a dose-dependent manner, which is associated with a change in processing from amyloidogenic to non-amyloidogenic and reduction in Aβ formation. [22-24] The levels of both soluble and insoluble Aβ were shown to decrease via oral administration of EGCG, by upregulating the α-secretase activity and downregulate the β- and γ-secretase activity. In-vivo, it has been demonstrated in numerous AD-related mice models that EGCG causes APP processing to shift in favour of a non-amyloidogenic route. [132,133]]
Myricetin: Myricetin is a naturally occurring flavanol that is found in a variety of fruits and vegetables, and also available in red wine, blackcurrant tea, and medicinal plants. [25-28] Myricetin has an anti-amyloidogenic properties by lessens the formation of Aβ-aggregation by creating H-bonds between its hydroxyl group and the carbonyl group on the surface of the β-sheet. As a result, myricetin limits the expansion of Aβ fibrils, inhibits the inter-strand hydrogen connections, and inhibit Aβ hazardous alterations. [29-33] Myricetin has been demonstrated to boost α-secretase level and enzyme activity, while inhibiting β-secretase activity, in cortical nerve cells of the cultured rat. It has been demonstrated that an H-bond is formed between the hydroxyl group at C7 of the A ring of myricetin and the pair of Asp 32 and 228 of BACE-1, resulting in a significant decrease in the enzyme's activity. [34,35]
Genistein: Genistein is a flavonoid that is mostly derived from the plant Glycine max soybean and is found in a variety of crops, including beans, green peas, and nuts. Numerous studies suggest that genistein may be used therapeutically to prevent the onset of Alzheimer's disease by enhancing cognitive ability and synapse formation. [36-38] By lowering the production and aggregation of Aβ, genistein guards against the advancement of AD. According to a study it has been shown that genistein's inhibitory efficacy against the degree of Aβ25-35 self-aggregation decreased when given after 24 hours of incubation. [39] Genistein altered the PPARγ receptor to promote the synthesis of ApoE in rat hippocampus neurons by decreasing presenilin levels, increasing αsecretase while decreasing βsecretase and BACE1 activity. [40-43]
Baicalein: Baicalein show its mechanism via a GABAAA receptor-dependent mechanism, promotes cleavage of APP that is not amyloidogenic while blocking cleavage that is amyloidogenic.[44] GABAA activation promote the non-amyloidogenic processing of APP and baicalein may control GABAA receptor activation by inhibiting the GABAA transaminase that breakdown GABAA and also inhibit the non-amyloidogenic processing of APP. [45-47]
4.2 Flavonoid inhibit aggregation and phosphorylation of tau
Physiologically, the microtubule-associated protein tau binds to microtubules primarily in axons. [48,49] Tau is assumed to have a major role in microtubule structure and stabilising, which facilitates the movement to and from synapses.889 Tau.

Table 2: Mechanism of flavonoid in Alzheimer’s Disease
On the other hand, becomes hyperphosphorylated and separates from the microtubule in AD. [48] Tau's mis-localization to the somatodendritic area, where it has been demonstrated to impede nuclear import and synaptic function, is facilitated by hyperphosphorylation. Local translating of tau mRNA, which is triggered by Abeta application via an FYN/ERK/S6 pathway, has also been linked to tau aggregation in the somatodendritic area. [50] Additionally, hyperphosphorylated tau forms oligomers that eventually form insoluble helical filaments and tangles of neurofibrillary cells (NFT), which are one of the distinguishing features of Alzheimer's disease (AD). [51] More precisely, numerous different kinases, including Erk, Akt, p38, AMPK, GSK3β, cdk5, and PP2A, influence the phosphorylation of Tau. An activation of MAPK, a heterotrimeric protein kinase, results in Tau being hyperphosphorylated in neurons. Additionally, it monitors Aβ's metabolism and participates in cell division, apoptosis, and inflammatory reactions. [52-55]

Figure 2 holecular target of flavonoid in Alzheimer’s Disease
Inhibiting the MAPK pathway is therefore a viable strategy for slowing the onset of AD and can considerably enhance synaptic remodelling, consciousness, and mental abilities. Numerous signalling pathways in cells are connected by GSK3β. It is regarded as the primary cause of the phosphorylation of the Tau protein in AD.
Quercetin: According to the research it has been shown that the main target of quercetin is MAPK. [56] As per study, by affecting GSK3β and reducing kinase activity, quercetin indirectly inhibits the hyperphosphorylation of Tau protein, which contributes to the strengthening of its neuroprotective effects. By pre-incubating HT22 cells with 5 mol/L of the medication for 12 hours, researchers were able to determine quercetin's anti-apoptotic effects through MAPKs and PI3K/Akt/GSK3ß signalling pathways. [57,58]
Genistein: In rat models of AD, genistein inhibits the formation and deposition of Aβ aggregates along with the excessive phosphorylation of the tau protein. [59-61]
Naringenin: In PC12 cells from AD-rats, naringenin increased learning and spatial memory via controlling the PI3K/Akt/GSK-3K pathway and lowering the hyperphosphorylation of TAU. The activation of PI3K/Akt, the modification of the signalling pathway GSK3β, and blocking the caspase 3 activity are all components of the intracellular system that enables this neuroprotective function and is essential for the survival of neuronal cells. [62-64]
Proanthocyanidins: It were given orally through a gavage, and this decreased the amount of lead-induced tau phosphorylation that was connected to the activation of p38 kinase and JNK, however not any direct correlation was found. [65]
Epicatechin: Exercise and dietary polyphenols epicatechin may improve brain function and decrease the course of a moderate- or mid-stage AD. [66]
Baicalein: The flavonoid baicalein's potential as a cutting-edge and effective oral bioactive treatment for Alzheimer's that inhibits memory loss. [67]
Hesperidin: In the hippocampus of APP/PS1 mice, EGCG administration decreased TNF-/JNK signalling and enhanced Akt and glycogen synthase kinase-3 phosphorylation. [68] Hesperidin may enhance cognitive performance in the APPswe/PS1dE9 transgenic mice model of AD by reducing mitochondrial dysfunction via suppression of GSK-3 activity, along with an improvement in anti-oxidative defence. [69] Through the stimulation of Akt/Nrf2 signalling and the suppression of RAGE/NF-B signalling, hesperidin reduces inflammation and oxidative stress while also providing neuroprotection. [70]

Figure 4: Mechanism of flavonoid inhibit aggregation and phosphorylation of tau
4.3 Flavonoid enhanced antioxidant reaction in AD
Generally speaking, flavonoids are renowned for their antioxidant properties [71], which may be helpful in AD given that oxidative damage has been linked to neurodegeneration. [72] According to evidence from post-mortem investigations on AD-brain, there is a net decline in the capacity to lower H2O2 levels and activate anti-oxidative stress pathways when compared to control brain. [73] H2O2 either activate MAPK signaling pathway or can react with metallic cation such as Fe2+, due to this it has been reported of abnormal brain-iron levels in AD. [74,75]
Although flavonoids have the ability to act as reactive oxygen scavengers by donating hydrogen ions, it is unlikely, that this is how they elicit their antioxidant potential because of the low potential to cross blood-brain barrier of flavonoids in the brain in comparison to better marked ROS scavengers. [76,77] It is more likely that the manipulation of intracellular pathways like the MAPK pathway by flavonoids, such as those found in plants, is how they suppress oxidative stress. [78]
In another study it is concluded that, nitric oxide synthase (NOS) activity is regulated by p53, and one of the most potent inducers of biosynthesis of mitochondria and respiration, and PGC-1a, is suppressed. The decrease in PGC-1α expression in AD is one of the factors contributing to the disease's progression because it is associated with an increasing in the production of peptide Aβ. It is another mechanism through which flavonoid show its anti-oxidant property in AD via inhibiting p53. [79,80]
Myricetin: Remarkable antioxidant properties as well as radical detoxification activities are ademonstrated by myricetin. Myricetin has been shown to be able to prevent the production of ROS, myeloperoxidase, and ATP depletion associated with oxidative stress in mouse models. But in animal models, it raises the degree and activities of the major antioxidant enzymes, including SOD, CAT, and GSHpx. As per study, treatment with myricetin for 3 hours enhanced the cell survival of isolated, inebriated cardiomyocytes, decreased aluminum phosphide, and also inhibited mitochondrial dysfunction. [81-83]
The pyrogallol group in myricetin is responsible for its antioxidant properties. This property helps to break the chain of events started by ROS. The molecule has a tendency to combine with radicals that are free to create radical semiquinones. [84-86] Moreover, the substance possesses chelating characteristics on metal ions like Cu2+ ions and Fe2+; this, on the one hand, significantly boosts its antioxidant activity since the Fenton reaction is hindered and, as a result, the creation of ROS is decreased. On the other hand, the toxicity of Aβ complexes is decreased by myricetin, which works directly on them, by limiting the number of metal ions that can interact with them. [87-89]
Genistein: Due to its strong antioxidant capacity and excellent ROS scavenger activity, genistein has been successfully demonstrated to alleviate oxidative stress in vitro. [90] The binding of the ER-α and activation of AMPK are both known to increase the production of antioxidant enzymes including SOD, CAT, and GPx. Genistein's antioxidant properties are also linked to these two processes. [91-93]
Quercetin: Because p53 is a substantial promoter of the ROS-mediated apoptosis pathway, quercetin's effect on p53 has an impact on the reduction of oxidative stress. By significantly scavenging ROS, quercetin has been proven for regaining the cellular redox equilibrium. [94,95] GSH levels and the expression of certain antioxidant enzymes, such as SOD, catalase CAT, and GPx, were raised in the mice by feeding a 1% quercetin diet for 20 weeks. [96-99]
Apigenin: Apigenin pretreatment effectively reduced the generation of intracellular ROS, reduced cellular DNA damage, decreased lipid peroxidation, alleviated protein carbonylation, and reinstated cell apoptosis. In another study, and it is also shown that apigenin enhanced the cellular antioxidant defence mechanism. [100-101] In another study, it has been shown that the apigenin demonstrated superoxide anion scavenging properties and enhanced glutathione peroxidase and superoxidase dismutase antioxidative enzyme activity in AD. [102]

Figure 5: Mechanism of flavonoid enhanced antioxidant reaction in AD
4.4 Flavonoid inhibiting AChE and BChE in AD
Acetylcholinesterase (AChE) is a particular esterase that is a member of the carboxylesterase class of enzymes. Acetylcholine (ACh), a neurotransmitter, is what it mostly hydrolyzes. AChE is primarily present in high quantities in red blood cells, as well as at cholinergic brain synapses and neuromuscular junctions in the brain. [103] The pathophysiology of AD is influenced by the decline in cholinergic activity in the brain regions in charge of higher cognitive tasks. The hallmarks of AD include localised A production and accumulation, intracellular neurofibrillary tangles, and extracellular senile plaques.mExtracellular deposits of the human beta-amyloid (Aβ) peptide are detected in senile plaques that are found in the brains of AD patients. [104,105]
According to research, a region close to the human AChE's C-terminus and the Alzheimer's disease Aβ peptide's N-terminus are only weakly homologous. The development of amyloid fibrils in plaques of senility and the toxicity linked to such deposits are further indications that AChE may be implicated. [106] BChE appears to be involved in the brain's conversion of risky amyloid plaques into the pathogenic formations that cause dementia and AD. [107]
Genistein: Genistein supplementation has been shown to affect dopaminergic and cholinergic activity, assisting in memory restoration and neuroprotection in mice and also alleviated brain insulin resistance. [108] As per study, the two variants of genistein inhibit the enzyme AChE, and demonstrating the medicinal potential of genistein. [109] According to the study, in MPTP-induced PD mice, genistein exhibits neuroprotective effects on dopaminergic neurons; this effect may be explained by increasing Bcl-2 gene expression. [110]
Quercetin: ACh levels drop and communication between neurons slows down in the brain. Through the phenyl ring's OH groups, quercetin establishes hydrogen bonds with certain amino acids in the AChE active site. Memory loss symptoms are reduced by AChE and BChE inhibition, which improves neuronal signalling and activates cholinergic pathways in the brain. [111,112] As per study, it has been shown that via using in vitro models, quercetin treatment caused the inhibition of AChE and secretase enzymes, blocking the breakdown of acetylcholine and reducing the synthesis of A, respectively. [113]
Myricetin: According to the study, myricetin have capacity to suppress AChE significantly lessened the mice's loss of learning and memory in the scopolamine-induced mouse model of Alzheimer's disease. [114]

Figure 6: Mechanism of flavonoid inhibiting AChE and BChE in AD
4.5 Flavonoid regulating neuroinflammatory response in AD
Alzheimer's disease (AD) causes complicated and poorly understood neuroinflammatory reactions. They relate contact among the central nervous system (CNS) and the periphery and involve diverse cellular and molecular actors. In the brains of AD patients and in mouse models of the disease, amyloid peptides seen in senile plaques and improperly phosphorylated tau in tangles of neurofibrillary cells can trigger inflammatory responses. These reactions' impact on pathophysiology of AD varies on a number of variables and may be advantageous or harmful. Thus, comprehending the function of neurological inflammation in AD may aid in the creation of safer and more effective therapy approaches. [115]
Myricetin: Myricetin decreases the amounts of proinflammatory mediators, such as IL, NF-kB, TNF, iNOS, and COX2, in the microglial BV2 cell line, which prevents lipopolysaccharide (LPS) from causing neuroinflammation. [116] Myricetin has the ability to suppress NLRP3, decrease microglia activation, and directly lower inflammatory factor levels. [117] By interfering with the NF-kβ signaling pathway, myricetin's anti-inflammatory activities primarily aim to lower levels of IL, TNF-, iNOS, COX-2, as well as other inflammatory mediators in the brain and lessen the damage these inflammatory factors cause to the neurological system. [118] Myricetin’s anti-inflammatory properties may eventually aid in easing AD symptoms.
Genistein: As per study, genistein suppresses neuro-inflammation in the RAW 264.7 cell culture by controlling the transcription of cytokines such TNFα, IL-1β, IL-6, and IL-12. [119,120]
Naringenin: Naringenin effectively modulates the (NF-kB) signaling system, which is linked to inflammatory processes, and lowers interleukin (IL)-6, IL-1, and tumour necrosis factor (TNF). [121] By significantly reducing the phosphorylation process and nuclear translocation of P65, an NF-kB subunit, as well as by raising sirtuin 1 (SIRT1) levels in the hippocampus, naringenin causes the lowered expression of NF-kB. [122]
Quercetin: It has been demonstrated that quercetin exerts anti-inflammatory effects via lowering the production of cytokines and other chemicals that cause inflammation. [123]

Figure 7: Mechanism of flavonoid regulating neuroinflammatory response in AD
The discussion of challenges in translating findings into clinical practice, including concerns regarding the bioavailability of flavonoids and the standardization of flavonoid-rich interventions, is pivotal in the treatment of AD. Addressing bioavailability underscores the importance of optimizing the delivery of flavonoids to ensure they reach therapeutic levels effectively, while acknowledging the variability in flavonoid content necessitates standardized approaches to ensure consistent dosing and research reproducibility. These challenges not only highlight the need for further investigation but also raise questions about the practical implementation of flavonoid-based interventions in Alzheimer's Disease treatment, emphasizing the complexities involved in transitioning promising research into effective clinical strategies. [124]
The inclusion of a discussion on the challenges related to translating findings into clinical practice, particularly focusing on issues of bioavailability and standardization of flavonoid-rich interventions, is a crucial aspect for effective pharmacological action. Here's an evaluation of this section:
5.1 Bioavailability Concerns: Addressing the bioavailability of flavonoids is essential because it reflects how effectively these compounds are absorbed and utilized by the body. This issue is relevant because some flavonoids may have low bioavailability, meaning they might not reach therapeutic levels in the brain or other target tissues. Discussing this challenge highlights the need for research to identify delivery methods or formulations that enhance flavonoid bioavailability. [124]
5.2 Standardization of Interventions: The mention of standardization is important as it recognizes the variability in flavonoid content among different sources, such as fruits, vegetables, and beverages. Standardization ensures that the intended dose of flavonoids is consistent across studies or clinical applications. It's a valid concern as inconsistent dosing can lead to inconsistent outcomes and hinder the reproducibility of research results.
5.3 Practical Implementation: While not explicitly mentioned, addressing these challenges also raises questions about the practicality of incorporating flavonoid-rich interventions into the daily lives of individuals at risk of or suffering from Alzheimer's Disease. It's not just about efficacy but also feasibility and acceptability to patients. [125]
5.4 Future Research Directions: Enhancement of flavonoid effect in AD, emphasizes the need for further rigorous research, including clinical trials. It would be beneficial to briefly suggest potential research directions to overcome these challenges. For example, exploring novel delivery methods to enhance bioavailability or developing standardized flavonoid supplements could be avenues for further investigation. [126]
In summary, discussing the challenges related to bioavailability and standardization of flavonoid-rich interventions in the context of Alzheimer's Disease treatment adds depth and realism to the further research in the treatment of AD. It highlights the practical hurdles that researchers and clinicians must address when considering the use of flavonoids as potential therapeutic agents.
In conclusion, this abstract presents a compelling case for exploring flavonoids as potential therapeutic agents in the treatment of Alzheimer's Disease. It effectively highlights their multifaceted neuroprotective properties, including antioxidant and anti-inflammatory effects, modulation of key pathological hallmarks, and promotion of critical brain processes like synaptic plasticity and neurogenesis. However, it judiciously acknowledges the challenges ahead, particularly regarding flavonoid bioavailability and the standardization of interventions. These obstacles underscore the necessity for rigorous research, including well-designed clinical trials, to assess the safety and efficacy of flavonoids in Alzheimer's Disease treatment. Despite these challenges, flavonoids represent a promising avenue for further investigation and potential inclusion in future Alzheimer's Disease therapeutic strategies, offering hope in the quest to combat this devastating neurodegenerative disorder.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
