
Research Article | DOI: https://doi.org/10.31579/2692-9562/151
1department Of Ent And Hns Bgs Global Institue Of Medical Sciences No 67, Bgs Health And Education City, Utarahalli Road, Kengeri, Bengaluru 560060
2professor And Head Of Department Department Of Ent And Hns Bgs Global Institue Of Medical Sciences No 67, Bgs Health And Education City, Utarahalli Road, Kengeri, Bengaluru 560060.
*Corresponding Author: Dechu Muddaiah, Department Of Ent And Hns Bgs Global Institue Of Medical Sciences No 67, Bgs Health And Education City, Utarahalli Road, Kengeri, Bengaluru 560060.
Citation: Dechu Muddaiah, Srinivas V, (2025), Coblation Adenotonsillectomy vs. Cold Steel Dissection Adenotonsillectomy – A Prospective Observational Study of Pediatric Population at Teritiary Care Hospital, Journal of Clinical Otorhinolaryngology, 7(4); DOI:10.31579/2692-9562/151
Copyright: © 2025, Dechu Muddaiah. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 September 2025 | Accepted: 30 September 2025 | Published: 10 October 2025
Keywords: adenotonsillectomy; coblation; cold dissection; surgical trauma; pain; haemorrhage
Background and Objective: This is a prospective study that comparing two different surgical techniques for adenotonsillectomy in terms of age, gender, intraoperative time and postoperative outcomes. The study population was allocated by purposive sampling into two groups; one underwent coblation adenotonsillectomy, while the other group was managed with cold steel dissection adenotonsillectomy.
Results
The study shows that both groups were similar in terms of age and gender distribution and it was not statistically significant. The intraoperative time in the coblation adenotonsillectomy (group 1) was significantly shorter with a mean of 84.4 vs. 119.8 minutes, p <0.05. Group 1 also had significantly less intraoperative blood loss than conventional adenotonsillectomy (Group 2) (mean 4.4 ml vs 16.2 ml, p <0.05). The postoperative pain assessment using the visual analog scale (VAS). Group 1 had significantly lower VAS scores on postoperative day 1 than Group 2 (mean 0.8 vs mean 4.4, p <0.05). However, there was no statistically significant difference in VAS scores between the two groups on postoperative day 7. The recovery day after surgery was significantly shorter in Group 1 than in Group 2 (median is 1 day vs 2 days, p <0.05).
Conclusions
In conclusion, Coblation Adenotonsillectomy is a faster and less traumatic surgical technique than Cold Steel Dissection Adenotonsillectomy. Coblation Adenotonsillectomy also resulted in less postoperative pain and faster recovery than Cold Steel Dissection Adenotonsillectomy.
Each year it has been estimated that about half a million adenotonsillectomies are to be performed in the US children itself.[1] There is no proper statistics available on Indian population especially among pediatric cases.
Tonsillectomy is one of the most commonly performed surgeries in the field of Otorhinolaryngology performed either with or without adenoidectomy. Tonsils are part of the body’s immune system and play a huge role in children below the age of 10 years.[2]
Considering children, age can’t become a determining factor for tonsillectomy, moreover tonsillectomy in healthy children lesser than 2 years of age was not associated to have any higher morbidities unless any concurrent co morbidities in such younger children. [3-5]
Although being the most commonly performed surgical procedure, tonsillectomies are associated with common complications such as primary and secondary hemorrhages as well as pain. Which in turn hamper the quality of life by reducing the ability of oral intake of both solids and liquid foods, which impairs the quality of life of the child as well as the parent, caretaker, or guardian. In a few cases, these may even lead to hospitalization and fatal outcomes as well.[6]
Several surgical modalities can be used for performing the adenotonsillectomy and the choice of technique may depend on the surgeon's experience, preference, and the specific needs of the patient. Cold steel dissection is the traditional technique used for adenotonsillectomy. The main advantage of this technique includes its simplicity.[7] and the lower cost. However, this technique may be associated with a risk of bleeding and pain8, which may cause discomfort for the patient.
Coblation is a newer technique used for adenotonsillectomy. The advantages of coblation include less postoperative pain, less blood loss, and faster healing.[8] However, this technique need proper setup and may be associated with a higher cost and time.[9,10] All these makes adenotonsillectomy surgery recommended to improve the nutrition and growth of children.[11].
The current study aims to present the outcomes such as intraoperative time, intraoperative blood loss, post-operative pain, and complications with coblation tonsillectomy versus the traditional cold steel tonsillectomy.
This was a prospective study in a tertiary hospital with 50 children between the age group of 3 to 15 years presenting to the out-patient ENT department with symptoms of chronic adenotonsillitis like recurrent URTI and adenotonsilar hypertrophy with snoring/OSA not relieved on medications were included in the study. All the participants underwent a thorough ENT examination and adenotonsillar hypertrophy of grade 3 and grade 4 were considered candidates for elective surgical removal of adenoids and tonsils. Exclusion criteria was age below 3 years, acute adenotonsillitis and bleeding disorders. Patients/parents/caretakers were given the choice of surgical technique after informing both the methods. Consent was obtained and the children were considered for surgery on the basis of the parents'/caretakers' choice.
Twenty-five patients who opted for the coblation adenotonsillectomy were considered as group 1 and the other 25 patients who opted for cold steel adenotonsillectomy were considered as group 2 for analysis purposes.
All the surgeries were performed by a single surgeon to avoid the physician skill factor. Standard anaesthetic and surgical techniques were followed for all the surgeries performed. The patients were placed in Trendelenburg’s position for coblation adenotonsillectomy and Rose’s position for cold steel adenotonsillectomy.
For the coblation technique, procise max wand, with default power setting 7, and coagulation 3 were used. Haemostasis was achieved and analgesics were used per the regular protocol.
The time from the start of the incision till the achievement of haemostasis was considered as intraoperative time and was noted in minutes. The number of completely soaked single-fold dry gauge pads and blood collected in the suction jar was considered for calculating the intraoperative blood loss. A seven-point visual assessment scale (VAS)with smiley face was used for assessing the pain perception (with a gradation of ‘0’ = no pain & ‘7’ = very severe pain) of the patients. The VAS scores were taken on postoperative day 1 (POD-1) and day 7 (POD-7). All the patients received intravenous antibiotic treatment for 24 hours followed by oral antibiotics for 5 days, and paracetamol was given for analgesia after the surgery. The ability to take solid foods and return to normal activity was considered as recovery time after surgery.
All the data collected were entered into a Microsoft Excel worksheet and analysed using R Software R-4.2.1. The qualitative variables like gender and age group were expressed in frequency with percentage. The descriptive statistics for quantitative variables age (in years), duration of surgery (minutes), intraoperative blood loss (ml), VAS score, and recovery day (after surgery) are expressed in mean with standard deviation (SD) and median with interquartile range (IQR). The study variables are tested for normality, using the Shapiro-Wilk test. And data was found to be non-normal hence non-parametric tests are applied. To compare study variables between any groups Mann-Whitney U-Test is applied. To Compare the VAS score from day 1 to 7 Wilcoxon Signed Ranks Test is applied. The p-value is considered statistically significant at a 5% level of significance.
As mentioned above all the patients were distributed equally into two groups with 25 in each group. The age distribution was between 3-15 years, and there was no statistically significant difference in age between the two groups (as shown in Figure. 1a).
Most of the study subjects were males, and there was no statistically significant difference in gender distribution between the two groups (as shown in Figure. 1b).
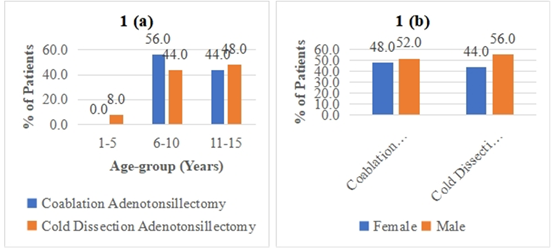
For age distribution analysis, the test statistic Mann-Whitney U test value was 302.5 with a p-value of 0.845 (>0.05).
For gender distribution analysis, the Chi-square test value was 0.0805 with a p-value of 0.7766.
Figure 1: Age & gender distribution of the study subjects
The median duration of intraoperative time, was significantly differentiating the Coblation Adenotonsillectomy group (90 minutes) was significantly lesser then the Cold Dissection Adenotonsillectomy group (120 minutes) (as shown in the Figure. 2a).
The median intraoperative blood loos in the Coblation Adenotonsillectomy group (5 ml), was significantly lesser then the Cold Dissection Adenotonsillectomy group (15 ml) (as shown in Figure. 2b).
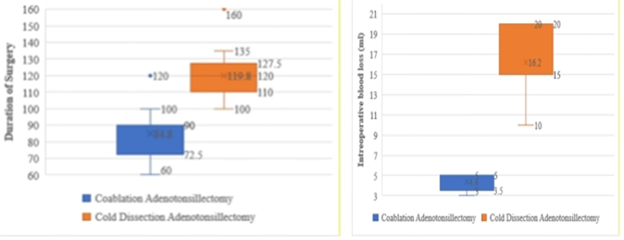
Figure 2: Intraoperative duration and blood loss between both the groups
The test statistic Mann-Whitney U test value was 31.0 with a p-value of 0.000 (<0.05)
The test statistic Mann-Whitney U test value was 0.000 with a p-value of 0.000 (<0.05).
Postoperative pain perception was assessed in the study subjects using VAS score. The post-operative day 1 (POD1) pain perception was significantly
lower in the Coblation Adenotonsillectomy group compared to the Cold Dissection Adenotonsillectomy group (Figure. 3a).
Similarly, the pain perception assessed by VAS score on POD7 in the Coblation Adenotonsillectomy group significantly lesser than the Cold Dissection Adenotonsillectomy group (Figure. 3b).

Figure 3: Post-operative day 1 and day 7 pain perception
The test statistic value for POD1 VAS in Mann-Whitney U test was 0.0 with a p-value of 0.00000000063 (<0.05). The test statistic value for POD7 in Mann-Whitney U test value was 225.0 with a p-value of 0.043 (<0.05).
The change in VAS Score from POD1(D1) to POD7 (D7) was assessed in both groups. In the Coblation Adenotonsillectomy group (Group 1), the median change in VAS score was 0 with a (0-1) interquartile range, also it was observed that 20% (5) had an increase in VAS score and 36% (9) had no change in VAS score on Day 7 compared D1 (p value of 0.1083 >0.05), showing that at D7 VAS score is not a statistically significant change compared to D1 (Table 1).
In the Cold Dissection Adenotonsillectomy group (Group 2), the median change in VAS score was 4 with (4.0-5.5) interquartile range, also it was observed that 100% (25) had a significant decrease in VAS score on Day 7 compared to D1 (p-value of 0.000009< 0.05) (Table 1). Therefore, as per VAS in the Cold Dissection Adenotonsillectomy group (Group 2) there was reduced post-operative pain from D1 to D7.
| VAS Post-Op | Paired Differences | VAS Score from POD 1 | Wilcoxon Signed Ranks Test | p-value | |||
| D1-D7 | Mean±SD | Median (Q1-Q3) | Decreased n (%) | Increased n (%) | Constant n (%) | ||
| Group 1 | 0.28±0.84 | 0 (0-1) | 11 (44%) | 5 (20%) | 9 (36%) | -1.6059 | 0.1083 |
| Group 2 | 4.4±1.35 | 4 (4-5.5) | 25 (100%) | 0 | 0 | -4.4499 | 0.000009 |
Table 1: Comparison of VAS scores from POD 1 to 7 among the groups
The recovery day after the surgery was between 0-2 days (median 1 day, IQR was 0-1) in Coblation Adenotonsillectomy, and most of them recovered in 1 day, 44% (11). In Cold Dissection Adenotonsillectomy it was between 1-3 days (median 2 days, IQR was 1-2 days), most of them recovered in 2 days, 56% (14).
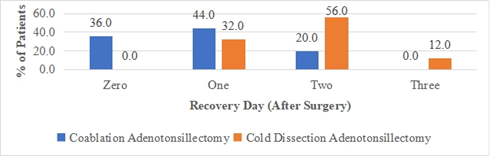
Figure 4: Post-operative recovery between the two groups.
The test statistic Mann-Whitney U test value was 119.0 with a p-value of 0.00006 (<0.05).
There were no significant differences observed in patient demographics in terms of age or gender among the patients between both groups. Although the age distribution was between 1-15 years among the patients, only 2 patients in cold dissection adenotonsillectomy were below the age of 5 years. The median age of the patients in the current study was 10 years for both groups and show no significant inter-group differences.
According to a scoping review, many randomized controlled trials in children on tonsillectomy/adenotonsillectomy published so far have included patients aged up to 13–18 years.[12]
The median intraoperative time (90 vs. 120 minutes, p < 0>
Shakeel et al., had reported lesser primary and secondary bleeding in children operated with coblation technique.[15]
A new classification of the anatomical subsites of the tonsillar fossa was presented to aid surgeons in minimizing the risk of haemorrhage during tonsillectomy.[16]
Children can be vulnerable to blood loss, and the loss of blood is seen more with the increase in age.[17]
The blood loss in tonsillectomy and adenotonsillectomy may depend on various factors such as age, sex, the type of tonsillitis, method of dissection, hemoglobin levels, clotting time and the use of antibiotics as reported by Prasad and Prasad, 2011.[17]
Over the past decades’ tonsillectomy indications have been increasing including for infections as well as for sleep disorders. [18]
Postoperative haemorrhage is a well-known risk if unaddressed would even cause a fatal outcome. Body weight alone may not convey all the characteristics of the patients that may affect the medication. Our study has the limitation of BMI which may further also need to be interpreted to come to one more conclusion that only surgical technique per se has resulted in lower pain scores.
In line with previous studies, the VAS scores in the current study were observed to be lower with the coblation adenotonsillectomy group compared to the cold dissection adenotonsillectomy group.[8,9]
The postoperative pain and discomfort is common for surgeries, this may compromise the recovery of the patient as it may affect the food and water intake especially in case of children. Mösges R et al. mentioned that coblation method as one such ‘gentle’ technique along with no more extra rates of secondary haemorrhage as of other comparable techniques.[19]
Although, the visual‐assisted scale is a commonly used system to report pain but has the bias of subjectivity. This can be further overcome by actually measuring the analgesic requirements in the immediate period following the surgery. Moreover, despite studies that have found that tonsillectomies are associated with severe pain but the data on adequate pain management strategies still was not sufficient and need further research.[12]
The recovery day after surgery was significantly shorter in Group 1 than in Group 2 (median is 1 day vs 2 days, p <0.05). Faster healing was reported in studies with coblation technology. It’s not only the dual benefit of ablation and coagulation via single instrument that can make coblation a faster technique but also having no cutting blade advantage can also promote faster healing.[20]
Another observation reported by a meta-analysis is better perioperative outcomes with coblation technique.[21]
Together both faster recovery to normal even to work makes Coblation a preferred method over traditional.8
The current study did not consider the BMI of the patients which may further also need to be interpreted to come to one more conclusion that only surgical technique per se has resulted in lower pain scores. Because the body weight alone may not convey all the characteristics of the patients that may affect the medication.
In conclusion, we could re-establish that Coblation Adenotonsillectomy is a faster and less traumatic surgical technique than traditional Cold Dissection Adenotonsillectomy. Coblation Adenotonsillectomy also resulted in less postoperative pain and faster recovery than Cold Dissection Adenotonsillectomy.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
