
Research Article | DOI: https://doi.org/10.31579/jcpmh.2021/008
*Corresponding Author: André Léké, MD, PhD, Soins Intensifs de Néonatologie et Médecine Néonatale, CHU Amiens Picardie Site Sud, 80054 Amiens Cedex 1, France.
Citation: André Léké., Géraldine Amar., Bertin Elion Dzon., Gilles Morin., Guy Kongolo., et al. (2021) Coagulase-Negative Staphylococcal Bacteremia by Bacterial Translocation of Gastrointestinal Origin in Preterm Infants: Role of Molecular Analysis. J. Clinical Pediatrics and Mother Health, 1(1);Doi:10.31579/jcpmh.2021/008
Copyright: © 2021 André Léké, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 June 2021 | Accepted: 05 July 2021 | Published: 09 July 2021
Keywords: bacterial translocation; coagulase-negative staphylococcus; blood culture; stool culture; preterm infants; molecular typing
Background: One hundred fifty-seven preterm infants were enrolled in the study. Only 28 (17.8%) were included in this work. The aim of this study was to assess the proportion of intestinal bacterial translocation associated with coagulase-negative staphylococcal bacteremia.
Methods: Blood cultures, stool cultures, antibiotic susceptibility, and genotyping were performed. All Staphylococcus isolates were identified by MALDI-TOF MS.
Results: Sixteen resistance patterns were identified from blood and stool based on antibiotic susceptibility testing. Ten of the coagulase-negative staphylococcus strains isolated from blood samples exhibited R pattern e (35.7%) and 11 of the coagulase-negative staphylococcus strains isolated from stool samples exhibited R pattern e (39.2%). Fifteen isolates exhibited: three ERIC-2 patterns, A (S. epidermidis), B (S. haemolyticus), and C (unidentified coagulase-negative staphylococcus), and three RAPD patterns, D (unidentified coagulase-negative staphylococcus), E (S. haemolyticus), and F (S. epidermidis).
Conclusion: Molecular typing confirmed an intestinal bacterial translocation in the preterm infants with coagulase-negative staphylococcal bacteremia.
AC-FMS: Antibiogram Committee of the French Microbiology Society; APUH: Amiens-Picardie University Hospital; BT: bacterial translocation; CI: confidence interval; CoNS: coagulase-negative staphylococcus; CRP: C-reactive protein; ERIC: enterobacterial repetitive intergenic Consensus; EUCAST; European Committee on Antimicrobial Susceptibility Testing; GIT: gastrointestinal tract; LBP: LPS binding protein; LPS: lipopolysaccharide; MALDI-TOF MS: matrix-assisted laser desorption ionization time flight mass spectrometry; MODS: multiple organ dysfunction syndrome; MLN: mesenteric lymph modes; MSA: mannitol salt agar: nICU: neonatal intensive care unit; OR: odds ratio; pICU: pediatric intensive care unit; RAPD: random amplification polymorphic DNA; RF: risk factor; RR: relative risk; SBCA: sheep blood Columbia agar; SD: standard deviation; uCoNS: unidentified coagulase-negative Staphylococcus; WG: week of gestation
Bacterial translocation (BT) is defined as the passage of live bacteria, bacterial DNA, or bacterial degradation products [lipopolysaccharide (LPS), bacterial lipoprotein, peptidoglycan, flagellin, unmethylated CpG DNA, tri-acyl lipopeptide, and di-acyl lipopeptide)] or both, across the lamina propia to local mesenteric lymph nodes (MLN) and from there to extranodal sites [1-3]. The intestinal tract has multiple functions in the body apart from its primary function of absorption of nutrients. It represents a real barrier protecting the body from living microorganisms, and antigens of the intestinal lumen.
Many physiological and pathological conditions, such as immaturity, fasting, mesenteric ischemia-reperfusion, shock states, can alter intestinal functioning. Alteration of the intestinal barrier results in a systemic inflammatory process and, more rarely, potentially fatal multiple organ dysfunction syndrome (MODS). Gastrointestinal tract (GIT) epithelial and immune cells play an essential role in initiation and resolution of the inflammatory process. Any adverse alteration of the intestinal barrier leads to disruption of this process, resulting in increased permeability of the intestinal barrier, promoting the passage of live bacteria, bacterial DNA or bacterial degradation products from the intestines to extraintestinal sites [4, 5]. The incidence of BT in humans undergoing emergency laparotomy has been reported to be 15.4%, and 14 to 21% [3, 6]. Numerous molecules have been evaluated as potential biomarkers for BT, including bacterial DNA, soluble CD14, l LPS/endotoxin, LPS binding protein (LBP), calprotectin, and d-lactate [7]. In humans, BT occurs commonly in clinical situations such as laparotomy, hematological malignancies, intestinal obstruction, trauma, liver resection, hemorrhagic shock, Crohn’ s disease, colorectal cancer, and aortic aneurysm repair [8, 9, 10, 11, 12]. The incidence of BT and its relationship to sepsis and MODS in preterm newborns remain unclear. Coagulase-negative Staphylococcal (CoNS) bacteremia is common in neonates and is often associated with the presence of a catheter. The mechanism responsible for intestinal BT remains poorly elucidated. It would therefore be interesting to study the proportion of BT responsible for CoNS bacteremia in a population of preterm infants. The objectives of this study were to assess the proportion of intestinal BT and its role in causing sepsis in clinical conditions, and to evaluate the correlation between CoNS isolated from blood cultures and stool cultures using molecular typing.
Ethical approval and consent to participate
All procedure performed in studies involving human participants were undertaken in accordance with the guidelines laid down in the Declaration of Helsinki and/or national research committee (Ethical Committee of Amiens-Picardie University Hospital (APUH), n° 139. Clinical and Laboratory data concerning the preterm infants were included in this study. Informed consent from legal guardians of the minors included in the study was not specifically requested. Study participants were all breastfeeding mothers considered to be autonomous and independent to decide on the participation of their baby in the study.
Study design and study population
During the study period, a total of 157 neonates (less than 28 days of life) born prematurely (<37>
Antibiotics used in patient treatment
Sixteen (57.1%) of the 28 preterm infants included in this study had received the following antibiotics during neonatal life: amoxicillin (9 cases), vancomycin (6 cases), amoxicillin + gentamicin (5 cases), fluoconazole (4 cases), piperacillin- tazobactam+ gentamicin (2 cases), vancomycin + amikacin (2 case), cefotaxime (2 cases), cilastine-imipenem + gentamicin (1 case), teicoplanin + amoxicillin (1 case), meropenem (1case), ceftazidime (1case), trimethoprim-sulfamethoxazole (1 case), metronidazole (1 case), and josamycin (1 case). These antibiotics were used individually or in combination in 15 suspected cases of maternal-fetal infections, and piperacillin-tazobactam+ gentamicin, vancomycin and metronidazole were used in one case of septic shock. Sixteen (57.1%) of the 28 mothers who delivered preterm had received the following antibiotics prior to delivery: amoxicillin (9 cases), ceftriaxone (2 cases), amoxycillin-clavulanic acid, piperacillin-tazobactam (1case), cefotaxime (1 case), ceftriaxone, cefixime and erythromycin (1 case), clindamycin and trimethoprim-sulfamethoxazole (1 case). These antibiotics were used individually or in combination to treat urinary tract infections, vaginal infections, and premature rupture of membranes.
Data collection
All data were obtained from the patient’s electronic medical records. Patient demographic characteristics, underlying conditions, and clinical and laboratory findings were collected.
Diagnostic criteria for bacteremia
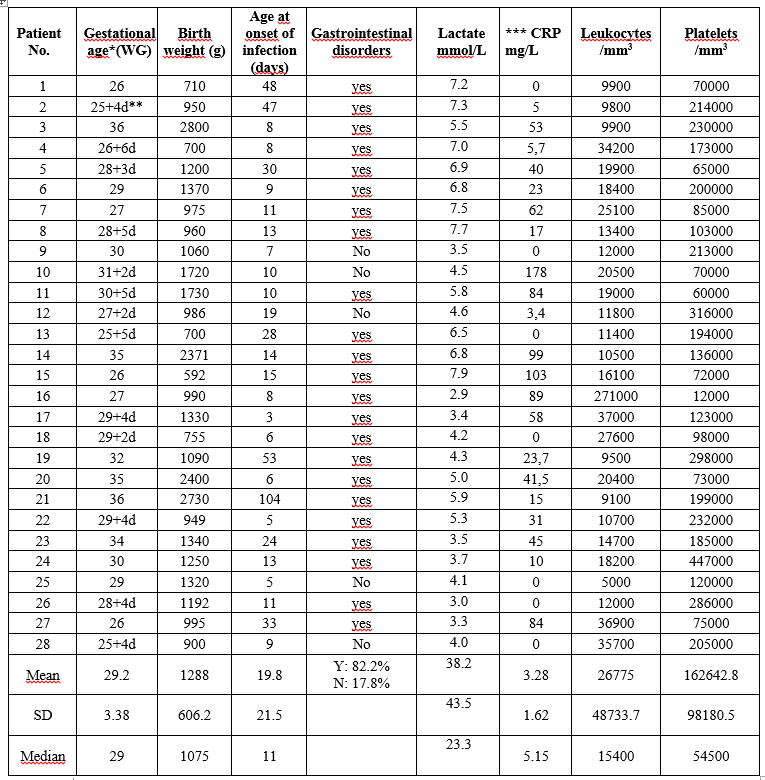
One positive blood culture in the presence of suggestive clinical signs: bradycardia, oxygen desaturation, increased respiratory requirements, total leukocyte count > 18,000/mm3, C-reactive protein (CRP) > 10 mg/L, serum lactate> 1.65 mmol/L, temperature > 38.3°C or < 36>
Blood and stool samples
Blood was obtained for routine hematological, biochemical and bacteriological tests, including polymorphonuclear leukocyte, platelet counts and CRP. Less than 0.5 mL of blood was inoculated into a Bactec Peds Plus F bottle and incubated in BactecTM Becton Dickinson instrument (BD Diagnostic Systems, Spark, MD, USA). Subcultures of initial blood culture broth were seeded on sheep blood (5%) Columbia agar (SBCA) and mannitol salt agar (MSA) (Oxoid, France) were incubated aerobically at 37°C for 24 hours. Anal or rectal samples using sterile swabs were seeded on SBCA and MSA and were incubated aerobically at 37°C for 48 hours.
Identification
Staphylococcus spp. were identified after examining all colonies. All isolates that were negative for mannitol and for bound coagulase (Pastorex Staph Plus-Bio-Rad, France) and positive for catalase and for Gram staining were classified as CoNS. All these Staphylococcus strains were examined by Matrix-Assisted-Laser Desorption Ionization Time of Flight Mass Spectrometry (MALDI-TOF-MS) (Brucker Daltonics, Bremen, Germany) according to a previously described procedure [13,14] when the child’s blood cultures were negative, the corresponding stool cultures and blood cultures were discarded.
Antibiotic susceptibility testing
Isolates were tested by the disk diffusion method on Mueller-Hinton (MH) agar according to the zone size criteria as recommended by the Antibiogram Committee of the French Microbiology Society (AC-FMS) and the European Committee on Antimicrobial Susceptibility Testing (EUCAST) – 2015 [15]. The antibiotics used were kanamycin (K), gentamicin (G), tobramycin (T), erythromycin (E), lincomycin (L), pristinamycin (PT), rifampin (RIF), ofloxacin (OFX), vancomycin (VAN), fusidic acid (FA), trimethoprim-sulfamethoxazole (SXT), and fosfomycin (FOS). Susceptibilities to benzylpenicillin (P) (disk loaded with 6 µg) and cefoxitin (FOX) (disk loaded with 30 µg) were determined by the disk diffusion method on salted MH at 37°C for 24 hours.
DNA isolation and molecular typing
Total nucleic acid extraction was performed using the bioMérieux NucliSENS easy MAG platform (bioMérieux, Marcy l’Etoile, France) according to the manufacturer’s instructions. ERIC-PCR (Enterobacterial Repetitive Intergenic Consensus-Polymerase Chain Reaction) was performed as previously described [16]. Extracted DNA (100 ng from each isolate) was amplified in a final volume of 50 µL of the ERIC-2 primer (5’-AAG-TAA-GTG-ACT-GGG-GTG-AGC-G-3’) and 5 µL of CoralLoad PCR buffer. PCR cycling consisted of 94°C for 7 min followed by 45 cycles of 94°C for 1 min, 45°C for 1 min and 72°C for 2 min, and 72°C for 7 min. RAPD-PCR (Random Amplification Polymorphic DNA) was performed as previously described [17]. The primer used was, 5’-GGT-TGG-GTG-AGA-ATT-GCA-CG-3’. Amplification reactions were carried out with a final volume of 50 µL containing 25 µL of Top Taq Master MIX (QIAGEN, Les Ulis, France), 1 µL of RAPD1 primer, 2 µL of DNA as template, 5 µL of CoralLoad PCR buffer. The cycling conditions were 95°C for 3 min, followed by 35 cycles of 94°C for 1 min, 40°C for 1 min, and 72°C for 2 min, and 72°C for 10 min. After amplifications, PCR products were resolved by electrophoresis on 1.2% agarose gels at 90 V for 6 h, followed by ethidium bromide staining and were visualized under UV light. A photograph was also taken.
Risk Factors (RFs) for gastrointestinal BT in preterm infants with CoNS bacteremia
The following clinical, laboratory and treatment parameters were analyzed as potential RFs for BT in this study. These RFs were categorized in two groups according to molecular typing: group1 included patients in whom BT was indicated; group 2, comprised patients in whom BT was not indicated.
Statistical analysis
We calculated the relative risk (RR) of BT among preterm infants with and without documented BT. Data are expressed as means ± standard deviation (SD) for quantitative variables and frequencies for qualitative variables. We calculated the RR of BT with associated 95% confidence intervals (CIs) using Fisher’s Exact test. Comparisons between documented BT and undocumented BT groups were performed with Wilcoxon-Mann-Whitney test for quantitative data and Fisher’s Exact test for qualitative data. All tests of significance were two-sided and a p value of < 0>
Patient characteristics
The characteristics of 28 preterm infants included in this study were as follows: gestational age (weeks): mean±SD:29.2±3.3, median: 29, range:25-36; birth weight (gram): mean± SD: 1,288±606.2, median: 1,075, range: 592-2,800; age at onset of infection (days): mean± SD: 19.8±21.5, median: 11, range: 3-104; Lactate (µmol/L): mean± SD: 38.2±43.5, median: 23.3, range: 3.0-43.5; CRP (mg/L): mean± SD: 3.28±1.62, median: 5.15, range: 0-178; Leukocytes (/mm3): mean± SD: 26,775±48,733.7, median: 15,400, range: 5,000-271,000; Platelets (/mm3): mean± SD : 162,642.8±98,180.5, median: 54,500, range: 60,000-286,000 (Table 1); maternal age at birth (years): mean± SD: 29.7±6.2, median: 29.5, range: 19-45.
Blood culture and stool culture results
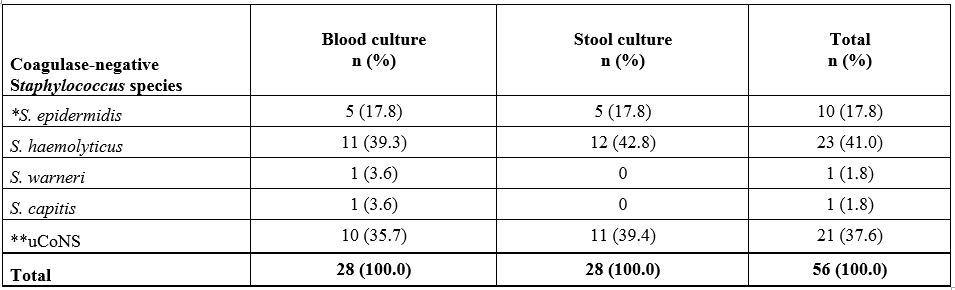
S. haemolyticus, unidentified coagulase-negative Staphylococcus spp. (uCoNS), and S. epidermidis were isolated from 39.3%, 35.7% and 17.8% of blood cultures respectively. S. haemolyticus, uCoNS, and S.epidermidis were isolated from 42.8%, 39.4%, and 17.8% of stool cultures, respectively. (Table 2).
Antibiotics susceptibility of CoNS strains
One hundred percent of the 28 CoNS strains isolated from blood cultures were resistant to penicillin, cefoxitin and kanamycin, and 96.4% of isolates were resistant to gentamicin, tobramycin and netilmicin. The resistance of these strains to other antibiotics tested are shown in Table 3.
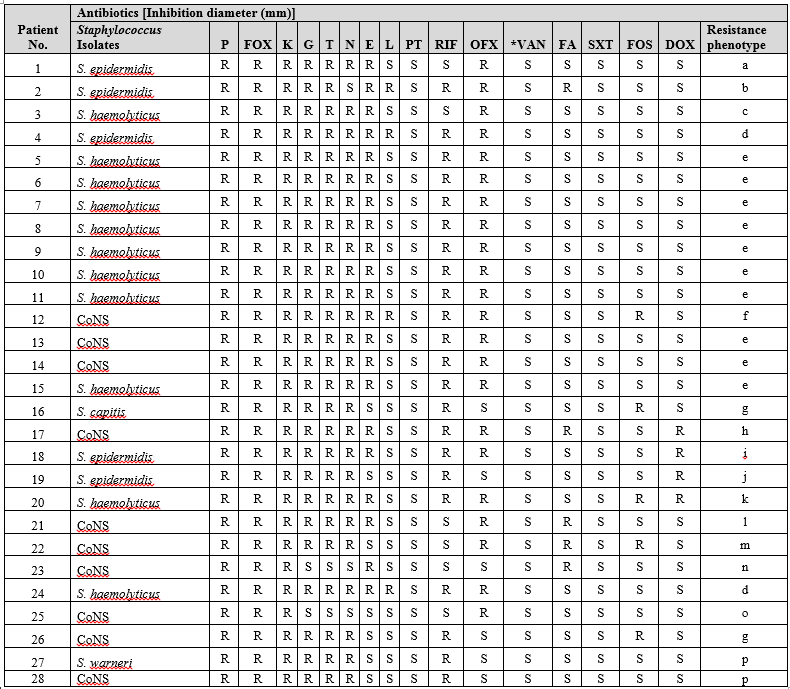
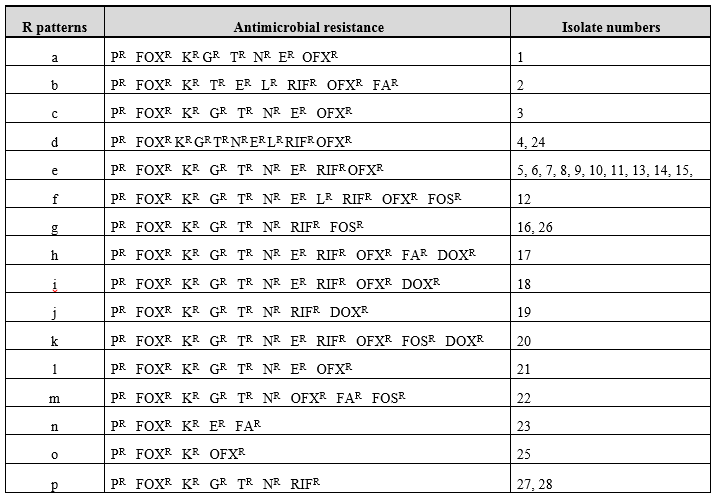
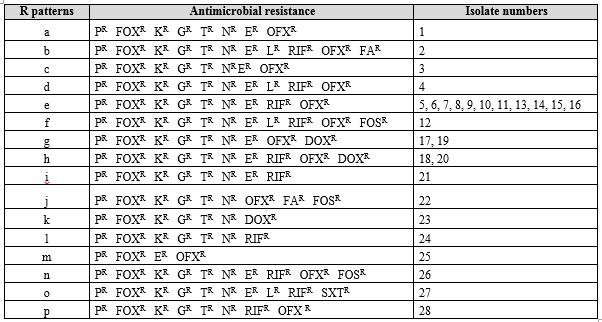
The distribution of resistance patterns of these isolates showed sixteen antimicrobial resistance patterns (R patterns) a-p, and 10 of these strains exhibited R pattern e [(35.7%) (isolates 5-11,13-15)] (Table 4).
One hundred percent of the 28 CoNS strains isolated from stool samples were resistant to penicillin, cefoxitin, and kanamycin, and 96.4% of isolates were resistant to gentamicin, tobramycin and netilmicin (Table 5).

The resistance of these isolates to other antibiotics tested are shown in Table 5. All these isolates were classified into sixteen R patterns a-p, and 11 of these strains exhibited R pattern e [(39.2%), (isolates 5-11,13-16)] (Table 6).
Comparison of blood culture and stool culture results according to phenotype resistance pattern
In this series of 28 Staphylococcus isolates, blood culture results were concordant with stool culture results in 53.5% (15/28) of cases and discordant in 46.5% (13/28) of cases. Ten of the fifteen concordant strains exhibited R pattern e and corresponded to eight S. haemolyticus and two uCoNS isolates; five strains exhibited R patterns a, b, d, e, and f, and corresponded to three S. epidermidis, one S. haemolyticus and one uCoNS isolates, respectively. The following resistance patterns were detected on blood cultures from the 12 discordant cases: g (S. capitis isolate), h (uCoNS isolate), j (S. epidermidis isolate), k (S. haemolyticus isolate), l (uCoNS isolate), m (uCoNS isolate), n (uCoNS isolate), d (S. haemolyticus isolate), o (uCoNS isolate), g (uCoNS isolate), p (S. warneri and uCoNS isolates). Similarly, the following R patterns were detected on stool cultures from the 12 discordant cases: e (uCoNS isolate), g (uCoNS isolate), h (S. haemolyticus isolate), i (uCoNS isolate), j (uCoNS isolate), k (uCoNS isolate), l (S. epidermidis isolate), m (uCoNS isolate), n (S. haemolyticus isolate), o (S. epidermidis isolate), and p (uCoNS isolate). The S. epidermidis (R pattern i) and S. haemolyticus (R pattern h) strains were isolated from blood culture and stool culture of patient 18, respectively.
Molecular typing results
Phenotyping results suggested BT from the GIT to the circulatory system in 15 preterm infants. When the same Staphylococcus spp. were isolated from both stool and peripheral blood, and exhibited the same resistance pattern, they were further genotyped by ERIC-PCR and RAPD-PCR to confirm BT. Fifteen isolates were selected to obtain a diverse sample of patients (blood and stool samples), and R patterns. These 15 selected Staphylococcus strains were compared by ERIC-PCR and RAPD-PCR.
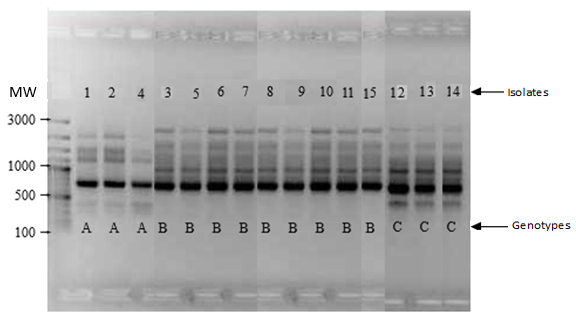
Three different ERIC-2 patterns (A, B, C) (Figure 1) and three different RAPD patterns (D, E, F) (Figure 2) were identified in the 15 selected isolates. ERIC-2 patterns comprised A [S. epidermidis (isolates 1, 2 and 4)]; B [S. haemolyticus (isolates 3,5-11, and 15)], and C [uCoNS (isolates 12-14)].
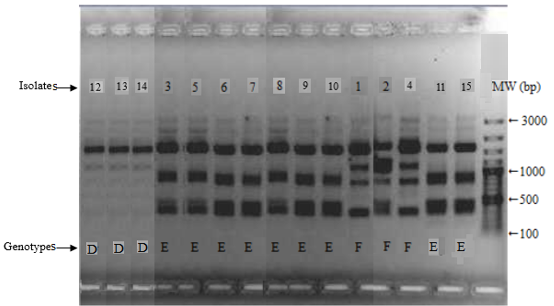
RAPD patterns consisted of D [uCoNS (isolates 12-14)], E [S. haemolyticus (isolates 3,5-11, and 15)], and F [S. epidermidis (isolates 1, 2, and 4)]. The three S. epidermidis R patterns a, b, and d exhibited the AF genotype; The three other uCoNS strains with resistance patterns e and f exhibited the CD genotype. Finally, nine S. haemolyticus phenotype e strains exhibited the BE genotype. This major epidemic BE profile included 60% of S. haemolyticus strains (9/15) isolated in both blood culture and stool culture, and was identified in both units participating in this study. The remaining strains (three S. epidermidis and three uCoNS) exhibiting AF and CD genotypes, respectively, were considered to be sporadic cases.
Combined analysis of ERIC-2 and RAPD results identified three different genomic groups (gg): I to III. The strains isolated from blood culture and stool culture in each group were more similar to each other than to the other strains.
Bacterial Translocation results
Translocation from the GIT to the circulatory system was documented in 53.5% (15/28) of preterm infants. The same Staphylococcus spp. was not found in blood and stool in 46.5% (13/28) of preterm infants, strongly suggesting the absence of BT in these preterm infants. In patient 18, blood culture was positive for S. epidermidis, and stool culture was positive for S. haemolyticus, although culture of a nasopharyngeal sample taken prior to the onset of bacteremia isolated S. epidermidis, suggesting that the respiratory tract was the probable source of bacteremia in this child (this source was not included in this study).
Risk factors for the occurrence of BT in preterm infants with CoNS bacteremia
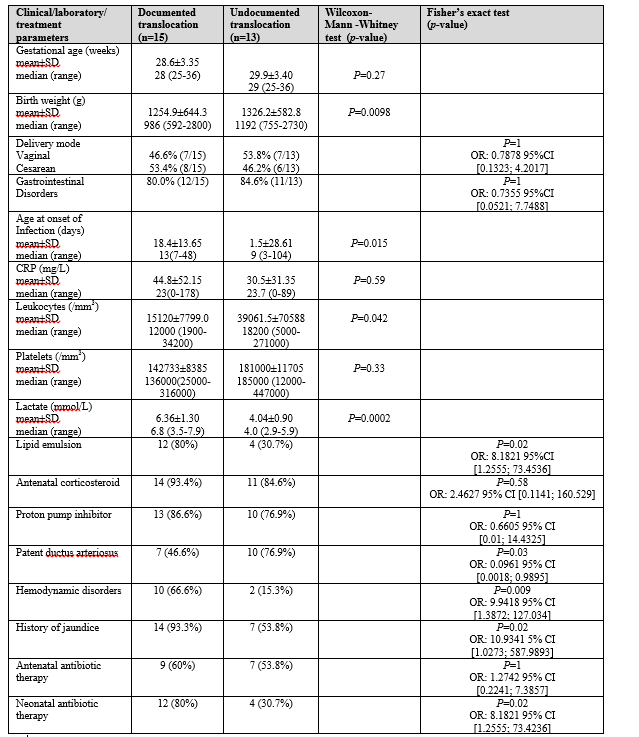
Comparison of documented (group1) and undocumented (group2) gastrointestinal BT is shown in Table 7. Two tests, Wilcoxon-Mann-Whitney test and Fisher’s Exact test, identified the presence of BT RFs, such as: birth weight (p=0.0098); age at onset of infection (p=0.01); leucocytes/mm3 (p=0.042); lactate/mmol/L (p=0.0002) (Wilcoxon-Mann-Whitney); intravenous perfusion lipid emulsion (OR:8.1821; 95% CI [1.2555; 73.4536]), p=0.02; treated patient ductus arteriosus (OR: 0.0961; 95% CI [0.0018; 0.9895]), p=0.03; hemodynamic disorders (OR: 9.9418; 95% CI [1.3972; 127.034]), p=0.009; history of jaundice (OR: 10.9341; 95% CI [1.0273; 587.9893], p=0.02; neonatal antibiotic therapy (OR: 8.1821; 95% CI [1.2555; 73.4236]), p=0.02 (Fisher’s Exact test) were direct independent RFs for the occurrence of gastrointestinal BT. None of the other RFs tested were significant.
In this study, S.haemolyticus and S.epidermidis were the CoNS species most isolated, with rates of 41.8% and 17.8% respectively. These pathogens are a major cause of nosocomial bacteremia and catheter infections in nICUs [18], and are the most common cause of late-reported sepsis [19, 20].
The results of this study established that birth weight, age at onset of infection, leucocytes, serum lactates, intravenous lipid emulsion perfusion, treated patient ductus arteriosus, hemodynamic disoders, history jaundice, and neonatal antibiotic therapy were independent RFs for the occurrence of BT in preterm infants with CoNS bacteremia. MacFie et al. [6] showed that the following factors were independently associated with an increased prevalence of BT based on univariate analysis: intestinal obstruction, jaundice, inflammatory bowel disease, malignancies, preoperative total parenteral nutrition (TPN) and emergency surgery. However, multivariate analysis showed that only emergency surgery and preoperative TPN were independently associated with translocation [7]. These results differ from those of our study in that our study population consisted of only a sample of preterm infants due to our inclusion criteria, whereas the participants in MacFie’ study with BT had a median age of 71 years.
Our study also showed that BT in preterm infants with sepsis is responsible of secondary bacteremia and is driven by external factors such as length of stay in the nICUs or prolonged feeding by an enteral feeding tube. Such results have been observed by Jezioski et al. [21].
According to the study conducted by Pappoff et al [2], prematurily appears to play a significant predisposing role by reducing mucosal barrier function. Other factors influencing BT have been reported in the literature [22, 23]. Various publications have identified BT in a wide group of diseases, such as acute pancreatitis, cirrhosis, malignancy, heart failure, aortic aneurysm repair, cardiopulmonary bypass, and bowel transplant [22-24].
In this study, the presence of BT from the gut to the circulatory system in 15 of 28 preterm infants with CoNS bacteremia represents a prevalence of 53.5
This study clearly demonstrates that BT from the intestinal tract was the most likely source of CoNS bacteremia in hospitalized preterm infants. BT appears to be an important early step in sepsis in debilitated preterm patients. Reinforcement of the intestinal barrier, regulation of the intestinal microbiota by breast milk and prebiotics or probiotics would be a possible approach to the prevention of intestinal BT.
The authors would like to thank the Clinical Research and Innovation Department for proofreading and correcting the English of the manuscript.
The authors have no financial relationships relevant to this article to disclose
The authors declare that they have no conflict of interest
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
