
Research Article | DOI: https://doi.org/10.31579/2642-9756/085
1 Obstetrics and Gynecology Department, Faculty of Medicine, Ain Shams University
*Corresponding Author: Nourhan Adel Abu Elfotouh Tantawy, Obstetrics and Gynecology Department, Faculty of Medicine, Ain Shams University
Citation: Mahmoud Youssef Ali Ahmed Abdalla, Abdel Rahman Mohammed Saleh & Nourhan Adel Abu Elfotouh Tantawy. (2021) Clomiphene Citrate versus Letrozole for Induction of Ovulation in Infertile women having Polycystic Ovarian Syndrome (Randomized Controlled Trial). J. Women Health Care and Issues. 4(7); DOI:10.31579/2642-9756/085
Copyright: © 2021 Nourhan Adel Abu Elfotouh Tantawy, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 August 2021 | Accepted: 20 August 2021 | Published: 25 August 2021
Keywords:
Background: Polycystic ovary syndrome is a disorder but with unclear etiology that its diagnosis depends on exclusion of other etiologies with ovulatory disorders and androgen excess as congenital adrenal hyperplasia, 21-hydroxylase deficient non classic congenital adrenal hyperplasia (NCAH), adrenal or ovarian androgen-secreting tumors, disorders of adrenocortical dysfunction as Cushing’s disease, and abuse of androgenic or anabolic drugs. Polycystic ovary syndrome affects approximately 6-15% of women in reproductive age and constitutes 50% of the causes of infertility in women.
Aim of the Work: To compare the efficacy of letrozole on ovulation induction to that of clomiphene citrate in women suffering polycystic ovary syndrome and the effect on the follicular maturation, endometrial thickness and pregnancy rate. This study was carried in the outpatient infertility clinic of Ain-Shams Maternity Hospital during the period from November 2020 till April 2021.
Patients and Methods: This study included 80 infertile women diagnosed as having polycystic ovary syndrome. Women were randomized into two groups. Letrozole group (1) included 40 women who were given the aromatase inhibitor (Letrozole) orally in a 5mg dose daily from day 3 to day 7 of the menstrual cycle. While Clomiphene citrate group (2) included 40 women who were given the clomiphene citrate orally in 100mg dose daily from day 3 to day 7 of the menstrual cycle. All women were counseled and informed consent was obtained before recruitment.
Results: In this study, ovulation rate was significantly more frequent in the Letrozole group (82.5%, 33 women reached ovulation successfully) than in Clomiphene citrate group (60%, 24 women reached ovulation successfully) within P value=0.024. Clomiphene citrate at a dose of 100mg showed more efficacies in the number of follicle ≥18mm than Letrozole at a dose of 5mg. In Letrozole group, the number of follicles (≥18mm in diameter) ranged from 1 to 2 with a Mean±SD= 1.4±0.65 and in Clomiphene citrate group, the number of follicles (≥18mm in diameter) ranged from 1 to 3 with a Mean±SD= 1.9± 0.41 (P value=0.0001).
Conclusion: Letrozole can be considered as a first line treatment of anovulation in polycystic ovary syndrome. But, moreover studies including larger number of cases will further confirm the efficacy of letrozole versus clomiphene citrate in induction of ovulation, reaching to the optimum doses for aromatases inhibitors, more observation on endometrial thickness, incidence of pregnancy outcomes, incidence of abortion and incidence of congenital fetal malformations.
Ovulation is a main event in reproduction cycle. Anovulatory dysfunction is common problem and is responsible for approximately 40% of female infertility (Baadwy et al., 2009).
Polycystic ovary syndrome (PCOS) considers a complex condition characterized by elevated androgen levels, menstrual irregularities, and/or small cysts on one or both ovaries (Ndefo, 2013).
The National Institute of Child Health and Human Development (NICHD) of the National Institutes of Health (NIH) gathered a panel of experts who developed the first known criteria for PCOS in year 1991 and realized that ovarian morphology was a key component in the diagnosis. After that, The European Society of Human Reproduction and Embryology (ESHRE) and the American Society for Reproductive Medicine (ASRM) sponsored a workshop in Rotterdam. Through the workshop, polycystic ovarian morphology on pelvic ultrasound was added to the NICHD/NIH criteria (Legro, 2013).
In year 2006, the Androgen Excess Society (AES) suggested that the NICHD/NIHS criteria might be used with modifications that contained the Rotterdam tool. The AES describes PCOS as a disorder primarily involving androgen excess, along with different combinations of phenotypic features (e.g., hyperandrogenemia, hirsutism, oligo-ovulation/anovulation, and/or polycystic ovaries) that may promote a more accurate diagnosis (Dewailly, 2011).
Using the modified Rotterdam criteria in clinical diagnosis of polycystic ovarian syndrome is easily reached and most often treatment can be initiated following a few basic investigation and exclusion of the male factor problem (Azziz, 2007).
For more than four decades, clomiphene citrate has been used as the first line therapy for induction of ovulation in women with anovulatory infertility and for super-ovulation in couples with unexplained infertility. It’s orally administrated, available and inexpensive (Palomba, 2004).
In addition, predictors of the ovulatory response to clomiphene are body mass index, the free androgen index, ovarian volume and low concentrations of IGF-BP-I. On the other hand, pregnancy predictors with clomiphene are age and the severity of the cycle disorders, i.e. better responses occur in women of a younger age and with maintained oligomenorrhoea or amenorrhea, suggesting that FSH threshold (amount of FSH required to stimulate the follicular maturation and the ensuing ovulation) and oocyte quality are specifically regulated (Imani et al., 1999).
Because of its long half-life (two weeks), clomiphene citrate accumulates in the body and may have a negative effect on the quality and quantity of cervical mucus, endometrial development, which may cause implantation failure, luteal phase defect (LPD) and significant thinning of endometrium. Clomiphene citrate resistance together with side effects like multi-follicular development and cyst formation are areas of concern. The desire for an effective alternative persist (Kamath, 2010).
Clomiphene Citrate has drawbacks, including its overall poor efficacy, a nearly high multiple-pregnancy rate (3 to 8%) as compared with the rate associated with unassisted conception (<1>
Letrozole is a third generation selective aromatase inhibitor that was used as an ovulation inductor in anovulatory infertility women with more than 5mm endometrial thickness (Guang and Rezk, 2018).
Letrozole has been in use as an ovulation induction agent for more than a decade. Even though emerging evidence suggests that it's an effective ovulation induction agent, comparable if not better than clomiphene (Kamath & George, 2011).
Other studies also reported that letrozole is effective in clomiphene-resistant patients, and also resulted in ovulation of 62
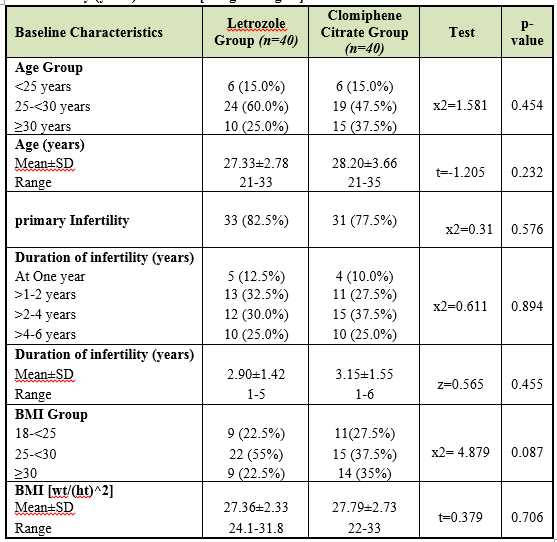
Table 1: Comparison between Letrozole Group and Clomiphene Citrate Group according to their demographic data regarding age (years), type of infertility, duration of infertility (years) and BMI [Weight/Height2].
t-Independent Sample t-test; z-Mann-Whitney test; x2: Chi-square test
p-value>0.05 NS; *p-value <0>
The two groups were comparable in age with the mean Age ±SD in each of Letrozole Group and Clomiphene Citrate Group was 27.33±2.78 compared to 28.20±3.66 respectively, there is no statistically significant difference between the two groups with p-value (p=0.232).
This table showed also Primary infertility that were comparable in each of Letrozole Group (were 33 patients (82.5%)) and Clomiphene Citrate Group (were 31 patients (77.5%)). there is no statistically significant difference between the two groups with p-value (p=0.567).
Also, the two groups were comparable in duration of infertility “years” with the mean in each of Letrozole Group and Clomiphene Citrate Group was 2.90±1.42 compared to 3.15±1.55 respectively, there is no statistically significant difference between the two groups with p-value (p=0.455).
Finally, the two groups were comparable in BMI with the mean in each of Letrozole Group and Clomiphene Citrate Group was 27.36±2.33 compared to 25.79±2.73 respectively, there is no statistically significant difference between the two groups with p-value (p=0.706).
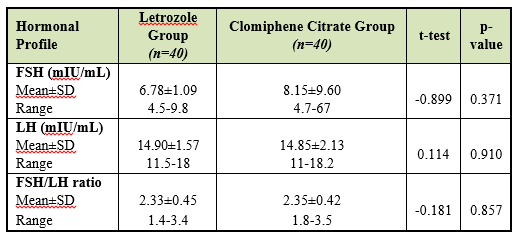
Table 2: Comparison between Letrozole Group and Clomiphene Citrate Group according to their hormonal profile regarding FSH, LH and FSH/LH ratio.t-Independent Sample t-test; p-value>0.05 NS
The two groups were comparable in FSH with the mean ±SD in each of Letrozole Group and Clomiphene Citrate Group was 6.78±1.09 compared to 8.15±9.60 respectively, there is no statistically significant difference between the two groups with p-value (p=0.371).
This table shows also, the two groups were comparable in LH with the mean ±SD in each of Letrozole Group and Clomiphene Citrate Group was 14.90±1.57 compared to 14.85±2.13 respectively, there is no statistically significant difference between the two groups with p-value (p=0.910).
While, the two groups were comparable in FSH/LH ratio with the mean ±SD in each of Letrozole Group and Clomiphene Citrate Group was 2.33±0.45 compared to 2.35±0.42 respectively, there is no statistically significant difference between the two groups with p-value (p=0.857).
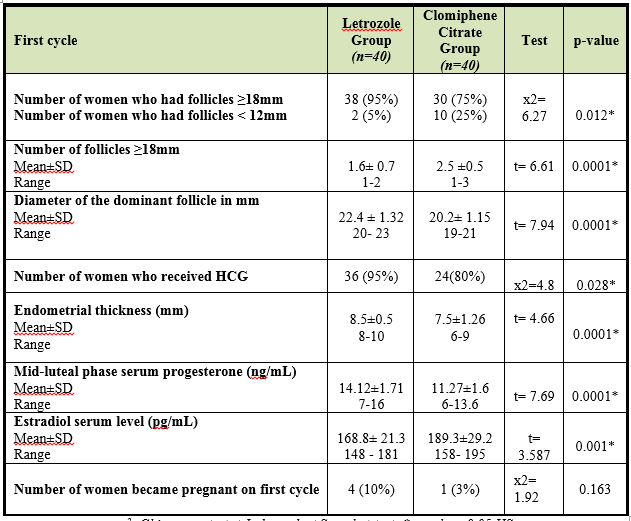
Table 3: Comparison between Letrozole Group and Clomiphene Citrate Group according to number of women had follicles ≥18mm and <12mm>
x2: Chi-square test; t-Independent Sample t-test; * p-value<0>
There was a highly statistically significant difference between two groups according to Number of women who had follicles ≥18mm and women who had follicles <12mm xss=removed>
There was a highly statistically significant difference between two groups according to Number of follicles ≥18mm on the day of hCG administration (p=0.0001). The highest value was found in Clomiphene citrate Group with Mean±SD 2.5 ±0.5 compared to Letrozole Group with Mean±SD 1.6± 0.7.
Also, there was a highly statistically significant difference between both group according to Diameter of the dominant follicle (p=0.0001). The highest value was found in Letrozole Group with Mean±SD 22.4 ± 1.32 compared to Clomiphene Citrate Group with Mean±SD 20.2± 1.15.
There was a highly statistically significant difference between two groups according to Number of women who received HCG (p= 0.034). The highest response was found in Letrozole Group 36 (95%) than Clomiphene Citrate Group 24 (80%).
There was a highly statistically significant difference between two groups according to Endometrial thickness (mm) on the day of hCG administration (p=0.0001). The highest value was found in Letrozole Group 8.5±0.5 compared to Clomiphene Citrate Group 7.5±1.26.
There was a highly statistically significant difference between two groups according to Mid-luteal phase serum progesterone level (p=0.0001). The highest value was found in Letrozole Group 14.12±1.71 ng/mL compared to Clomiphene Citrate Group 11.27±1.6 ng/mL.
There was a highly statistically significant difference between two groups according to Estradiol serum level on the day of hCG administration (p=0.001). The highest value was found in Clomiphene Citrate Group 189.3±29.2 pg/mL compared to Letrozole Group 168.8± 21.3 pg/mL.
The two groups were comparable in Number of women became pregnant on the first cycle, in Letrozole Group 4 women became pregnant (10%) while in Clomiphene Citrate Group 1 became pregnant (3%), there is no statistically significant difference between the two groups with p-value (p=0.163).
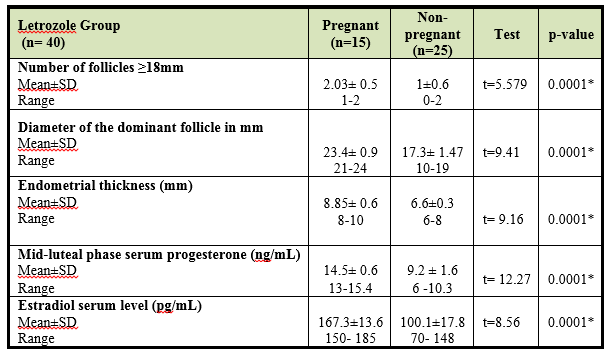
Table 4: Comparison between Pregnant and non-pregnant women in Letrozole Group according to their number of follicle(s) ≥18mm on the day of hCG administration, diameter of the dominant follicle, endometrial thickness (mm), estradiol serum level on the day of hCG administration (pg/ml) and mid-luteal phase serum progesterone level (ng/mL)
t-Independent Sample t-test; *p-value<0>
There was a highly statistically significant difference between two groups according to Number of follicles ≥18mm on the day of hCG administration (p=0.0001). The highest value was found in Pregnant Group with Mean±SD 2.03± 0.5 compared to Non-pregnant Group with Mean±SD 1±0.6.
Also, there was a highly statistically significant difference between both group according to Diameter of the dominant follicle (p=0.0001). The highest value was found in Pregnant Group with Mean±SD 23.4± 0.9 compared to Non-pregnant Group with Mean±SD 17.3± 1.47.
There was a highly statistically significant difference between two groups according to Endometrial thickness (mm) on the day of hCG administration (p=0.0001). The highest value was found in Pregnant Group 8.85± 0.6 compared to Non-pregnant Group 6.6±0.3.
There was a highly statistically significant difference between two groups according to Mid-luteal phase serum progesterone level (p=0.0001). The highest value was found in Pregnant Group 14.5±0.6 ng/mL compared to Non-pregnant Group 9.2±1.6 ng/mL.
There was a highly statistically significant difference between two groups according to Estradiol serum level on the day of hCG administration (p=0.0001). The highest value was found in Pregnant Group 167.3±13.6 pg/mL compared to Non-pregnant 100.1±17.8 pg/mL.
Polycystic ovary syndrome (PCO) is a disorder but with unclear etiology. For that, it became a diagnosis of exclusion, by exclusion of other etiologies with androgen excess and ovulatory disorders. For example, Androgen excess disorders should be excluded are 21-hydroxylase deficient non classic congenital adrenal hyperplasia (NCAH), adrenal or ovarian androgen-secreting tumors, disorders of adrenocortical dysfunction as Cushing’s disease, and abuse of androgenic or anabolic drugs. Although not true androgen excess, namely idiopathic hirsutism, should be excluded (Azziz, 2007).
According to Rotterdam criteria, diagnosis of polycystic ovary syndrome needs two of three characteristics: oligomenorrhea and/or anovulation, clinical and/or biochemical signs of hyperandrogenism and polycystic ovaries according to pelvic ultrasound (Dunaif, 2013; Lawrenson, 2014; Escobar-Morreale, 2018).
Clomiphene citrate is a non-steroidal selective estrogen-receptor modulator that binds to estrogen receptors and makes agonist effects in some tissues and antagonist effect on other tissue (Grese, 1997; Barroso, 2006).
The main mechanism of action of clomiphene citrate is to induce ovarian stimulation through the anti-estrogenic effect on the hypothalamus and pituitary leading to increase the pulse frequency and concentration of the FSH and LH within increase of ovarian follicles to reach the ovulation (Casper & Mitwally, 2006; Porter, 2008).
Aromatase inhibitors are three generations that might be steroidal or non-steroidal inhibitors (Bhatnagar, 1990 and Brodie, 1996) which block estrogen synthesis affect directly hypothalamic pituitary ovarian axis function and that theoretically may increase pregnancy rate (Casper & Mitwally, 2006).
Letrozole is a triazole derivative (antifungal) which is potent, reversible, competitive, non-steroidal, and highly selective aromatase inhibitor (Badawy, 2009). It prevents androgen to estrogen conversion in the ovary and leads to decrease in estrogen level providing negative feedback in hypothalamus which stimulates the pituitary gland to secrete FSH and development of follicle (Stafeno, Legro et al., 2014). Letrozole is rapidly absorbed from GIT and completely bioavailable up to 99.9
Letrozole has efficacy as that of clomiphene citrate in induction of ovulation in polycystic ovary syndrome. Within 5mg daily dose of letrozole, women can achieve ovulation in about (82.5%) and pregnancy in about (37.5%).
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
