
Research Article | DOI: https://doi.org/10.31579/2578-8949/120
1 Third year resident, Department of Dermatology, Shree Krishna Hospital, Karamsad, India. 2 First year resident, Department of Dermatology, Shree Krishna Hospital, Karamsad, India. 3 Professor and Head, Department of ENT, Shree KrishnaHospital, Karamsad, India.
4 Head of Dentisry Department, Shree Krishna Hospital, Karamsad, India.
5 Professor and Head, Department of Dermatology, ShreeKrishna Hospital, Karamsad, India.
*Corresponding Author: Vora Rita V, Professor and Head, Department of Dermatology, Shree Krishna Hospital, Karamsad, India.
Citation: Patel Jalpa K., Pillai Devna S., Sharma Yojana A., Prajapati Aalap S., and Vora Rita V., (2024), Clinicoepidemiological Study of Oral Mucosal Lesions and Its Impact on Quality of Life in Patients Attending Skin OPD at Rural Based Tertiary Health Care Centre, Dermatology and Dermatitis, 10(1); DOI:10.31579/2578-8949/120
Copyright: © 2024, Vora Rita V. This is an open-access article distributed under the terms of The Creative Commons. Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 July 2023 | Accepted: 09 August 2023 | Published: 02 January 2024
Keywords: oral mucosal lesions; oral lichen planus; dermatology life quality index; patients; tongue abnormality
Background
Oral mucosa is one of the first barriers to the outside world which encounters various antigens, microorganisms and physical agents and it is in direct continuity with the skin externally and with the mucosa of oropharynx and nasopharynx internally.
Objectives
The objective of our study was to study the prevalence of oral mucosal lesion, its association with various dermatoses and quality of life in patients with oral mucosal lesions attending outpatient department of dermatology at a tertiary care health centre.
Methods
This study was an observational, purposive type of study conducted in Department of Dermatology at a tertiary health care centre. All the patients with oral mucosal lesion were included with full history and detailed examination noted in a prestructured proforma. Dermatology Life Quality Index (DLQI) and Children’s Life Quality Index (CDLQI) both were used to assess quality of life.
Results: Among 202 (prevalence-0.8%) patients, maximum numbers of patients 53 (26.23 %) belonged to age group 31-40 years followed by 49(24.25 %) patients with age group of 21-30 years. Maximum numbers of patients were female 108 (53.46
%). Among oral ulcers recurrent aphthous stomatitis was the commonest finding seen in 56 (27.72%). Among cutaneous conditions associated with oral lesions oral lichen planus 50(24.75%) was the most common condition followed by pemphigus in 15(7.42%) patients. Out of 195 patients, maximum 86 (44.10%) patients were categorised as a moderately affected DLQI group.
Conclusion: Oral ulcers were the most common finding seen in our study. There were a significant number of patients of cutaneous conditions associated with oral lesions seen.
Oral mucosa is one of the first barriers to the outside world which encounters various antigens, microorganisms and physical agents and it
is in direct continuity with the skin externally and with the mucosa of oropharynx and nasopharynx internally, yet, the specialized nature of the
oral environment carries with it distinct adaptations responsible for its unique properties and functions [1]. The oral mucosa serves as a protective barrier against trauma, pathogens, and carcinogenic agents [2] .Oral mucosal manifestation may be the initial feature, most florid clinical feature or the only sign of such disease and sometimes lesions occur in both skin and mucous membrane. [3].
Oral lesions have a great impact on quality of life of an individual. Quality of life (QL) is a multidisciplinary and multi-dimensional assessing concept that refers to the subjective and objective conditions related to physical, emotional and social factors [4].
This study is an observational, purposive type of study conducted in Department of Dermatology, Venereology and Leprology at a tertiary healthcare centre over a period of Twelve months from April 2021to March 2022 after approval from ethical committee. (IEC/BU/127/Faculty/7/73/2021) All the patients with oral mucosal lesion were included. Informed written consent was taken in vernacular language from all patients. Patient’s full history and detailed examination was noted in a prestructured proforma. The parameters included in proforma are age, sex, occupation, duration of lesion, past history, family history, habits and oral hygiene status. Oral cavity examination was carried out according to prestructured proforma and findings were recorded. Dermatology Life Quality Index (DLQI) and Children’s Life Quality Index (CDLQI) both were used to assess quality of life. Descriptive Statistics [Mean (SD), Frequency (%)] were used to depict the baseline profile of the study participants. Used Quality of life scale was analysed by reporting Descriptive Statistics [Median, Mode].
We have examined a total of 24,868 patients from April 2021 to March 2022 over a period of twelve months. Out of which, 202 (prevalence- 0.8%) patientspresented with variousoral mucosal lesions.Demographic details are summarised in Table 1.
In present study most common chief complaint was burning sensation (n=73, 36.14%) followed by difficulty in eating (n=46, 22.77%) and multiple raw area in oral cavity (n=40, 19.80%). Most common oral complaint was difficulty in eating (n=183, 90.59%) followed by intolerance to food (n=82, 40.59 %) and redness (n=76, 37.62 %). In present study 59(29.21%) patients had gradual onset while 143 (70.79 %) had sudden onset. The duration of complaint were < 10>3 months in 19(9.41%). Among 202 cases 190 (94.06%) lesions were progressive and 12(5.94%) were non progressive. Tobacco chewing was the most common habit(n=23,11.38%) followed by cigarette smoking (n=21, 10.40%). Oral hygiene was fair in 158(78.22%) patients and poor in 44(21.78%). Among Oral lesions buccal mucosa (n=154, 76.24%) followed by lips (n=59, 29.21%) and floor of mouth (n=53, 26.24%) were the common sites involved. The most common morphology was ulcer (n=62,30.69%) and erosion (n=56, 27.72%). Other mucosal sites affected were genital(n=14,22.95%) and conjunctival mucosa (n=3, 4.92%).
In present study we have divided oral lesions in 10 groups according to etiological factors and morphology of lesions. Maximum numbers of
patients were seen in group of oral ulcers (n=70, 34.65%) followed by cutaneous conditions associated with oral lesion (n=67, 33.16%) and Infections (n=33, 16.33%).
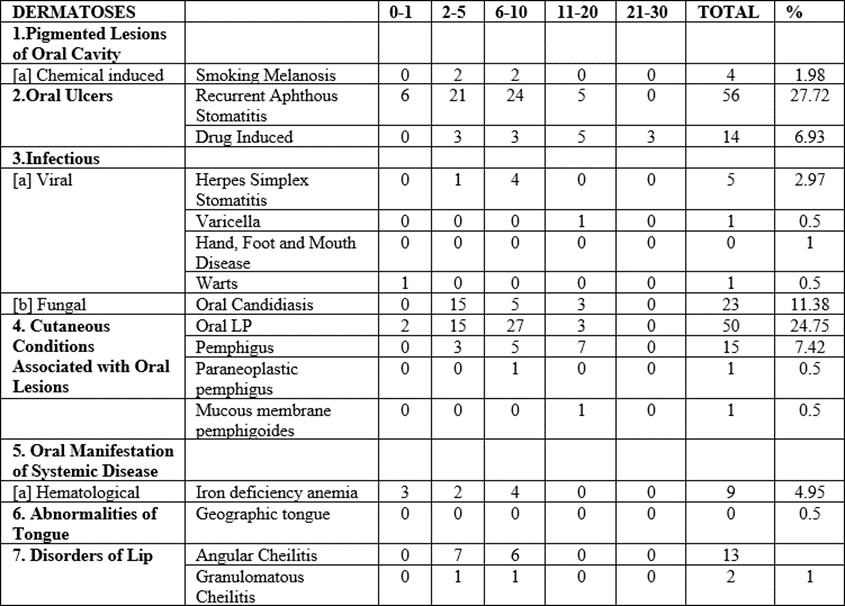
Among pigmented oral lesion smoking melanosis [Figure 1A] was seen in 4(1.98%) patients. In oral ulcers, recurrent Aphthous stomatitis [Figure 1B] was the commonest finding seen in 56 (27.72%) and drug induced in 14(6.93%) patients [Figure 1C]. Among infectious condition, in viral infection most common findings were herpes simplex stomatitis 6(2.97%) [Figure 1D] and hand foot mouth disease in 2(1%). In fungal infection oral candidiasis was seen in 23(11.38%) patients [Figure 2A]. Iron deficiency anemia was seen in 10(4.95%) patients among oral manifestation of systemic disease. Among abnormalities of tongue, geographic tongue [Figure 2B] was seen in 1(0.5%) patient. Among disorder of lip group 13(6.43%) patients were of angular cheilitis and 2(1%) of granulomatous cheilitis [Figure 2C and D]. Among cutaneous conditions associated with oral lesions oral lichen planus 50(24.75%) [Figure 3(A and B)] was the most common condition followed by pemphigus in 15(7.42%) patients [Figure 3(C and D)]. Among nodule and swelling group mucocele [Figure 4 (A&B)] was seen in 2(1%) patients.

Figure 1 (A): Smoking Induced Pigmentation; (B): Recurrent aphthous Stomatitis; (C): Drug Induced Oral Ulcers; (D): Herpes SimplexStomatitis

Figure 2(A): Oral Candidiasis; (B): Geographic Tongue; (C): Angular Cheilitis; (D): Granulomatous Cheilitis

Figure 3 (A&B): Oral Lichen Planus; (C&D): Oral Pemphigus

Figure 4 (A&B): Mucocele
Out of 195 adult patients, maximum86 (44.10%) patientswere categorised as a moderately affected DLQI group followed by 70 (35.90%) patients as a small affected DLQI group. Among 7 children’s patients maximum5 (71.43%) patientswere categorised as a moderately
affected CDLQI group followedby 2 (28.57%) patients as a not affected CDLQI group.
We have done DLQI wise distribution of various oral dermatoses and summarized it in Table 2.

Table 2: DLQI Wise Distribution of Various Oral Dermatoses
Mucocutaneous lesions commonly manifest as erosive, ulcerative, pigmented and sometimes as vesicular lesions. Various etiological factors contribute to the development of these lesions and encompass autoimmune, infectious, neoplastic, hematologic, reactive, nutritional, and idiopathic causes [5]. The oral cavity is vulnerable to a limitless number of environmental insults because of its exposure to the external world [6].
In our study total of 202 patients were enrolled. In present study maximum number of patients were seen in age group of 31-40 years, that is 53(26.23%) which is similar to Modi et al. [7] study (21.8%) and Gambhir et al. [8] study (21.5%). Out of 202 patients, 94 (46.5%) were males and 108 (53.4%) were females which was comparable to study done by Modi et al. [7] where males were 39.5% and females were 60.5%. In Andrej et al. [9] study males were 37.4% and females were 62.6 %. While in Byakodi et al. [10] study males were 66.6% and females were 33.4% which could be due to higher number of males examined in this study.
In present study the most common site of involvement was buccal mucosa in 76.24% of patients, which was comparable to Roy et al. [11] (68%) and Scully et al. [12] study (71%). In present study smoking was reported in 18.32% patients which is comparable to Suliman et al. [13] where it was seen in 17.7% patients. Total 4.46% patients were taking alcohol while tobacco chewing was seen in 11.38% patients which is comparable to Suliman et al, [13] that is 4.3% and 12.7% respectively. In present study smoking melanosis was seen in 4 (1.98%) patients which is comparable to Mohammad et al. [14] study where pigmentation was seen in 3(2.4%) patients and Kamble et al. [15] where it was seen in 2.7% patients.
In our study among oral ulcers, recurrent aphthous stomatitis 56 (27.72%) was the most common finding which is similar to Byakodi et al. [10] 31.3% and Mohammad et al. [14] 22.4% while in Kamble et al. [15] study it was seen in 3.57% patients. Our study was conducted in area which is the hub of tobacco production. This might be the reason for higher number of cases of recurrent aphthous stomatitis.
Drug induced oral ulcers were seen in 14(6.93%) patients while in Babu RA et al.[16] study it was 15 (23.08%) which might be due to small sample size of Babu RA et al. [16] study .Among viral infection herpes simplex stomatitis (2.97%) was the most common finding in our study which is comparable to Kamble et al. [15] (2.89%) and Suliman et al. [13] (6.2%).Oral candidiasis was present in 23(11.38%) patients in this study which is similar to Mohammad et al. [14] study (12%). In Kamble et al. [15] 6(1.02%) patients had oral candidiasis. Ours is a tertiary care health centre so reference from other specialities were also included in the study which might be the reason for higher number of oral candidiasis.
Among cutaneous conditions associated with oral lesions, oral lichen planus 50(24.75%) was the most common finding which is comparable to Babu RA et al. [16] study where it was seen in 18% patients and 22.2% in Gambhir et al. [8] study. Pemphigus vulgaris was seen in 15(7.42%) patients in present study which is similar to Mohammad et al. [14] study where it was seen in 4.8% patients.
Among tongue abnormality, geographic tongue was seen in 1(0.5%) patient in our study while in Andrej et al. [9] and Kamble et al. [15] it was 2.81% and 4.25% respectively. It might be due to larger sample size in this study. In our study angular cheilitis was seen in 13(6.43%) patients which is similar to Mohammad et al. [14] where it was seen in 6.48% patients and 10.71% in Roy et al. [11] Mucocele was seen in 2(1%) patients in present study which is comparable to Mohammad et al. [14] and Kamble et al. [15] where it was seen in 0.4% and 1.29% patients respectively.
Strengths of the study are already included in the above details. This is a single centred study so results could not be generalised, hence multicentric study is required. There were no controversies related to the study. Future research prospects of this study are it can be helpful in diagnosing various pattern of oral lesions in Anand district.
This study providesan idea about pattern of oral mucosallesions in Ananddistrict. Oral ulcers were the most common finding seen in our study. A significant number of patients of cutaneous conditions associated with oral lesions were seen. Oral manifestations can be a clue to a difficult to diagnose the dermatological conditions.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
