
Research Article | DOI: https://doi.org/10.31579/2694-0248/059
Orthopedics Department, Spanish Hospital. Av. Mexican National Army 613, Granada, Miguel Hidalgo, 11520 Mexico City, CDMX, Mexico, USA.
*Corresponding Author: Gómez Mont Landerreche Juan Gabino, Orthopedics Department, Spanish Hospital. Av. Mexican National Army 613, Granada, Miguel Hidalgo, 11520 Mexico City, CDMX, Mexico, USA.
Citation: Rodriguez M V, Gómez Mont L J Gabino, Castañeda G Jossue, Jarquin G F de Jesus, and Palafox C. Ignacio, (2023); Clinical Results at Six Months of Follow-up, of an Isolated Reconstruction of the Medial Patellofemoral Ligament in the Population of the Spanish Hospital of Mexico, J. Clinical Orthopedics and Trauma Care, 5(2); DOI: 10.31579/2694-0248/059
Copyright: © 2023, Gómez Mont Landerreche Juan Gabino. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 April 2023 | Accepted: 25 May 2023 | Published: 19 May 2023
Keywords: patellofemoral instability; shuttle point; medial patellofemoral ligament reconstruction; traumatic patella dissociation
Background/ Aim: The patellofemoral instability is a common pathology in young patients. Rupture of medial patellofemoral ligament occurs in more than 90% of acute patellar dislocations and almost 100% of the recurrent ones. Isolated medial patellofemoral ligament reconstruction has better postoperative results in patients without significant anatomic abnormalities compared to combined procedures. The objective of this study is to evaluate the post-surgical functional result in a period minimum of 6 months after the isolated reconstruction of the medial patellofemoral ligament in the population of the Spanish Hospital of Mexico.
Materials and Methods: An observational prospective cohort study was conducted. During the period between February 2017 to January 2022. 15 knees with patellar femoral instability with rupture of the of medial patellofemoral ligament were acquired, without additional anatomic risk factors. An isolated reconstruction of the medial patellofemoral ligament with allograft was performed. Clinical results were evaluated with a 6-month follow-up using functional scales (IKDC, Lysholm, Tegner, Kujala), as well as Visual Analogue Scale (VAS) for pain. All data were collected and analyzed using Microsoft Excel.
Results: The median of the pre-surgical scores and at 6 months of follow-up were: IKDC from 37(30-56.3) to 77(74- 81, Tegner from 40(35-49) to 94(89-96), Kujala from 46 (37-66) to 75(70-82), EVA went from 6 to 2.
Conclusion: The patients had an improvement in their functional scales greater than 30 points compared to their pre- surgical assessment. The isolated reconstruction of the medial patellofemoral ligament is a good alternative for the treatment of patellar dislocations, when they have the appropriate indication.
MPFL: Medial Patellofemoral Ligament.
MPFLR: Medial Patellofemoral Ligament Reconstruction.
IKDC: International Knee Documentation Committee.
VAS: Visual Analogue Scale.
TT-TG distance: Tibial tuberosity- trochlear groove distance
Patellofemoral instability is a pathology that affects the general population, with a reported incidence rate of primary patella luxation of 5.8 per 1000,000 [1]; with a peak incidence in patients of all ages at 15 years [2]. The clinical presentation includes frequent episodes of patella luxation, knee inflammation, and restricted range of motion of the knee, “J” sign, and limited functional activities. Primary patellaluxation has the potential to lead to unfavorable clinical outcomes, including recurrent instability, anterior knee pain, and patellofemoral osteoarthritis; they can cause changes in physical activity and decreased physical capacity. Negative long-term outcomes are associated with decreased physical fitness [2].
Patellofemoral instability has been shown to be multifactorial, with both skeletal and soft tissue abnormalities playing a role. Bony restrictions include bony interaction of the patella within the trochlea [3]. Soft tissue restraints include both static and dynamic soft tissue. Soft tissue abnormalities can be dynamic in nature, including hypermobility due to collagen disorders or a weak vastus medial is oblique (VMO) muscle; or static such as medial patellofemoral ligament insufficiency (MPFL). MPFL is a thickening of the medial retinaculum, an important static stabilizer responsible for providing the main medial constraint. The MPFLR is estimated to provide 50-60% of the soft tissue restraint during the first 30° of flexion prior to patellar engagement in the trochlear groove. MPFL rupture occurs in >90% of acute patellar dislocations and ~100% of recurrent ones [4-6].
Conservative treatment includes periods of immobilization, patellar stabilization with braces or taping, activity modification, and physical therapy to strengthen quadriceps and range-of-motion exercises. Medial patellofemoral ligament repair (MPFL) is the preferred surgical treatment for recurrent patellar instability, and can be implemented alone or in combination with other procedures to correct soft tissue imbalance or bony malalignment. Isolated MLPFL reconstruction has better postoperative results in patients without significant anatomic abnormalities compared to combined procedures [7-9].
Lippacher in his study, the purpose of which was to demonstrate the postoperative results and the rate of return to sports in a minimum period of 2 years after reconstruction of the medial patellofemoral ligament (MPFLR). He conducted a cohort study between 2007 and 2010 with a total of 72 MPFL surgeries for recurrent dislocation. Pre- and post-operative evaluation of the knee included a complete history of symptoms and knee function was assessed using the Kujala, IKDC and Tegner scales [6]; as well as the visual analog pain scale (VAS) and the activity scale (ARS). Of the patients who participated in sports before the operation (62 of 68), 100% returned to participate in sports after MPFLR. 53% returned at the same or higher levels. 54 of 68 patients (79.4%) rated themselves as very satisfied or satisfied with the results. The median of the functional scales improves, that of Kujala from 66 to 87.5, that of IKDC from 60 to 79.8. The median VAS improved from 4 to 2. The Tegner score decreased from 4.5 to 4, and the median Activity Rating Scale score decreased from 6 to 3. MPFLR is a safe and effective treatment. Effective for patellofemoral instability without severe trochlear dysplasia and allows most patients to participate in regular sporting activities 2 years postoperatively [7].
Ambrozic’s work, his objective was to demonstrate the postoperative results and the return to physical and sports activities in an average of 6 years after medial patellofemoral ligament reconstruction surgery (MPFLR).In a period of time between November 2006 and January 2010, 31 MPFLR surgeries were performed with a diagnosis of recurrent patella luxation. Knee function was assessed pre and postoperatively using the IKDC, Tegner, and Kujala functional scales. The mean Kujala score increased from 75±10 to 95±10, the IKDC patient satisfaction from 6.1±1.4 to 8.7±1.4, and the Tegner score from 4.4±1.5 at 5.7±1.3. Isolated MPFL reconstruction is an efficient treatment option for all patients with patellofemoral instability, allowing most patients to return to their activities of daily living and sports after surgery [4, 12].
The functional scales (IKDC, Tegner and Lyshom) are criteria that make it possible to identify how the MPFLR improves the functional results of patients diagnosed with patella luxation in follow-up studies from six months to four yearsin some studies [6, 11, 12].
The objective of this work is to evaluate the clinical status after the isolated repair of the MPFL at six months of follow-up, comparing it with their functional scales prior to surgery those are: IKDC, Lysholm, Tegner, Kujala; and the visual analog pain scale (VAS). The secondary objectives are the presence of complications after the surgery.
Isolated MPFL reconstruction is an efficient treatment option for all patients with patellofemoral instability, allowing most patients to return to their activities of daily living and sports after surgery. Is a well-accepted procedure, excluding additional bone risk factors, leading to successful results in the majority of patients and improving the patient's ability to perform activities of daily living [6, 14]. However, there are few follow-up studies after MPFLR. In the literature, the percentage of patients who return to their preoperative levels of sports activity after surgery varies from 32% to 76% [6].
This study was approved by the ethics protocol of our institution. A prospective observational cohort study, with a minimum follow-up of 6 months after the surgical procedure. The patients were diagnosed and treated surgically by two orthopedic physicians at the Spanish hospital of Mexico. Once they met the inclusion and exclusion criteria (which are detailed below): for the study protocol, their data was recorded in a database, which only the treating physicians have access to. The foregoing in order to follow up on the day of his surgical intervention and in his post- surgical evolution.
The data of the variables will be collected from the clinical records, during the period of February 2017 to January 2022. The collection was carried out by the resident orthopedics doctor of the Spanish Hospital responsible for the study protocol. These files are stored in the medical file of the unit or electronically in the hospital computers; they can be located with the help of the patient's file number. The functional scales (IKDC, Lysholm, Tegner, Kujala), as well as the visual analogue scale of pain (VAS) will be filled out by patients at the time of admission to the hospital, at their 6-month follow-up consultation, by phone call or email with prior authorization by the treating physicians and patients. For patients who did not have functional scales at the time of admission to the hospital or during their follow- up, the responsible resident was in charge of communicating with the patients to obtain the information by email or phone call with prior authorization from the patient.
A database was created using Excel, later the data was analyzed using the statistical program STATA VERSION 17. Variables with non-parametric distribution are reported with median, range; and Man Whitney U test is used for statistical significance. For qualitative variables, absolute numbers, averages, and percentages were used.
Between February 2017 and January 2022, the author made 15 reconstructions of the MPFL in 12 patients [6]. This patient met the following inclusion criteria: medial patellofemoral ligament rupture, acute patella dislocation, recurrent patella dislocation, patellofemoral instability, recurrent subluxation (apprehension), and presence of the “J” sign. Patients with trochlear dysplasia (according to the Dejour classification) [10], a high patella, previous knee surgery, tibial torsional deformity, advanced chondral lesions, open growth physis, and established patellofemoral osteoarthritis were excluded.
The diagnosis of patellofemoral ligament rupture was established by simple magnetic resonance imaging of the knee. MPFL is a thickening of the medial retinaculum [1], an important static stabilizer which provides the main medial restriction. Clinically, patients present a history of presenting patella luxation. On physical examination they may present: "J" sign, pain on the anterior side of the knee, pain on the MPFL, increased patellar translation to passive mobilization, positive patellar apprehension sign, increased "Q" angle. Anteroposterior, lateral, and axial radiographs with 30° of flexion were requested to rule out fractures, angular deformities, trochlear dysplasia, and high patella [2, 3, 8].
The objective of this work is to evaluate the clinical status after the isolated repair of the MPFL with a minimum follow-up of six months, comparing it with their scales prior to surgery. We use the functional scales (IKDC, Lysholm, Tegner, Kujala), and the visual analog pain scale (VAS).
During the period between February 2017 and January 2022, a sample of 12 patients (15 knees) was obtained, because3 patients underwent bilateral surgery at different surgical times.
The median age at the time of the surgical intervention was 28 years, with a minimum of 13 years and a maximum of 33 years of age. Of the 12 patients, 6 identified themselves as male and 6 as female; who had a minimum follow-up of 6 months after their surgical intervention.
The median IKDC score improved from 37 (30-56.3) preoperatively to 77 (74-81) at follow-up (P 0.10). Median Tegner score improved from 40 (35-49) preoperative to 94 (89-96)6-month postoperative (P 0.56). The median Kujala score improved from 46 (37-66) before surgery to 75 (70-82) at postoperative follow-up (P 0.15). The median for the visual analog scale for pain (VAS) was from 6 (5-8) preoperatively, with a decrease in pain to 2 (1-4) postoperatively (P 0.94). The results were not statistically significant (P>0.05%), using the Mann-Whitney U test; Therefore, studies with a larger sample and a follow-up of more than 6 months are required to evaluate the statistical significance of the reconstruction of the MPFL. (Table 1 & Graphic 1)
| Characteristic | No. = 15 |
| Age, Median (Range) | 28 (13 – 33) |
Sex, n (%) Female Male |
6 (50) 6 (50) |
| IKDC First Assessment Score, Median (Range) | 37 (30 – 56.3) |
| IKDC Second Assessment Score, Median(Range) | 77 (74-81) |
| Tegner Score First Assessment, Median (Range) | 40 (35-49) |
| Tegner Score Second Assessment, Median(Range) | 94 (89-96) |
| Score Kujala First Assessment, Median (Range) | 46 (37-66) |
| Kujala Second Assessment Score, Median (Range) | 75 (70-82) |
| First Assessment EVA Score, Median (Range) | 6 (5-8) |
| Second Assessment EVA Score, Median(Range) | 2 (1-4) |
Complications, n (%) Yeah No |
3 (20) 12 (80) |
Table 1: Results table (variable, median and range):
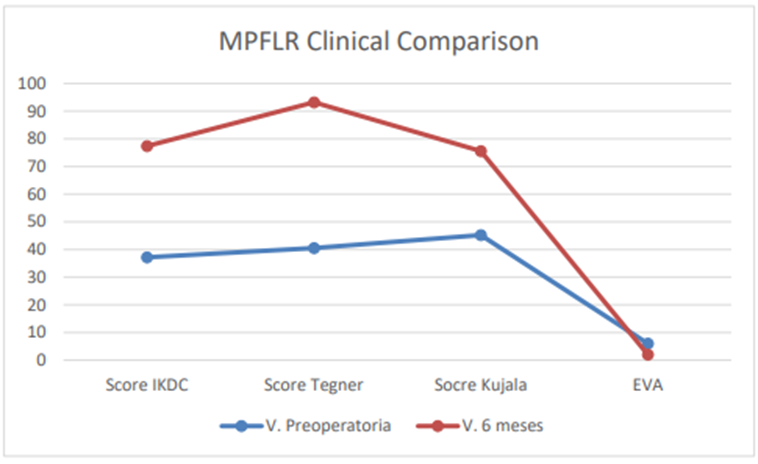
Graphic 1: Comparative graph of clinical results6 months after the surgical procedure(MPFLR *):
Medial Patellofemoral Ligament Reconstruction.
During the follow-up period of the study, 3 patients (20%) presented complications after surgery, which could be resolved with good results. One of them was a patella fracture 3 months after surgery, treated surgically. One patient presented an infection at the surgical site which was treated conservatively with targeted antibiotic therapy. The other patient presented a soft tissue infection which was surgically treated with surgical cleaning and targeted antibiotic therapy.
Patellofemoral instability is a pathology that affects the general population, with a reported incidence rate of primary patella luxation of 5.8 per 1000,000. This pathology is more common in young patients with an incidence rate of patella luxation of 29 per 1000,000 from 10 to 17 years old [1]; with a peak incidence in patients of all ages at 15 years [2].
The most consistent indication for performing an isolated MPFL reconstruction was recurrent patella instability without bone alterations [5]. Common reasons for not performing this procedure were bone malalignment (TT-TG abnormality), trochlear dysplasia, and high patella [10]. The significant disability associated with patellofemoral instability has led to the development of numerous patella and soft tissue stabilization procedures. Our patients met the inclusion criteria to perform an isolated reconstruction of the MPFL Such as medial patellofemoral ligament rupture, acute patella dislocation, recurrent patella dislocation, patellofemoral instability, recurrent subluxation (apprehension), and presence of the “J” sign.
Patients with more than one anatomical alteration for patellar instability should be treated according to the abnormality that every patient has. Such alterations as trochlear dysplasia (according to the Dejour classification) [10], a high patella, TT-TG distance >20mm, or tibial torsional deformity. This is because the isolated reconstruction of the MPFL cannot resolve the other abnormalities, which would increase the risk of re-dislocation and a poor functional outcome in the follow-up [6, 9, 10, 13].
The surgical treatment option of MPFL reconstruction is emerging as the gold standard for the treatment of recurrent patellar dislocations, compared to conservative treatment or ligament repair [7, 9, 11, 14]. In our present work, MPFL reconstruction proved to be a safe and effective treatment for isolated patellofemoral instability in a court of patients from the Spanish Hospital, but surgical indications must be carefully considered and individualized for each patient. During the follow-up our patients showed improvements in their functional scales.
The mean age at the time of the surgical intervention was 25 years. It is an active population, which requires a good resolution of its symptoms to be able to return to its daily physical activities. The good results reported are comparable with the works published by other authors[9, 6]. In our study we evaluated same number of male and female patients, six for each one; being reported in the literature a higher prevalence of women with patella instability [6, 7, 3].
The patients obtained a global improvement in their symptoms at the 6-month follow-up, managing to resume their activities. Good results were demonstrated in all knee scores (Kujala, IKDC, and Tegner) and pain improvement in their VAS result, with an improvement greater than 30 points. The median Kujala score improved from 46 (37-66) before surgery to 75 (70-82) at follow up; this score is reported to assess subjective symptoms and functional limitations for patellofemoral disorders [4]. The Tegner score can be used as an indicator of return to sports[8], the median Tegner score improved from 40 (35-49)preoperative to 94 (89-96) 6-monthpostoperative. The presence of pain can limit a patient's ability to return to their daily activities; our work found an improvement in the pain scores (VAS) from 6 to 2; reported by our patients after MPFL reconstruction.
Straume‑Næsheim report that patients treated only with active rehabilitation have a six-told increased risk of persistent patellar instability, in patients with patellofemoral instability; compared to MPFLR in combination with active rehabilitation [13]. In our follow-up the patients received the same physical rehabilitation protocol and no dislocations events were reported after surgery.
Manjunat [8] reported in his work 26.1% of complications related to the reconstruction of the MPFL, most of them being patellar fracture, recurrent instability in post-surgical examination, loss of knee flexion, complications with the wound and post-operative persistent pain [2, 6, 8]. In our follow-up there were three complications, one patella fracture and two problems related to the wound; represented 20% of our population. The complications were resolved satisfactorily and it helped us to create preventive measures for adequate post-surgical follow-up. In our experience, we recommend using the smaller size anchor (3.0 mm) or using all-suture anchors; with the purpose of avoiding subsequent patella fractures.
This work had potential limitations and biases, the mainly one was due to having a small number of patients which result without statistical significance. The follow-up should be longer, at least up to five years, to really know the functional results of the isolated reconstruction of the patellofemoral ligament. The assessment at follow-up was not blinded, which must be considered a limitation of this study.
Patellofemoral ligament reconstruction has become a popular option in the treatment of patellofemoral instability; demonstrating a significant improvement in the functional scales of the knee. Although this treatment can be accompanied by additional procedures, it is generally an effective option when it has the appropriate indication. In our study, good clinical results were obtained, with improvement in all functional scales. Follow-up studies with a larger number of patients are needed to be able to consider this procedure as the gold standard for the treatment of recurrent patellar dislocations. There is little published literature that investigates sports activity after MPFL reconstruction and its physical rehabilitation protocols for the return of athletes to their level of physical activity prior to their injury.
The content is solely the responsibility of the author.
The author has no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
