
Research Article | DOI: https://doi.org/10.31579/2640-1045/084
*Corresponding Author: Rizwan Khalid, Professor, Departments of Surgery and Biomedical Engineering University of California Irvine.
Citation: R Khalid, M Hassaan, A Raza. (2021) Clinical Presentation of Primary Hyperparathyroidism in Lahore, Pakistan – A Single Center Study. Endocrinology and Disorders. 5(5): DOI:10.31579/2640-1045/084
Copyright: © 2021 Rizwan Khalid. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 09 August 2021 | Accepted: 21 August 2021 | Published: 30 August 2021
Keywords: primary hyperparathyroidism; calcium; parathyroid hormone
Aim: To assess different clinical presentations and outcomes of primary hyperparathyroidism in Pakistan.
Study Design: Retrospective cross-sectional study.
Study Setting: East Surgical Ward, Mayo Hospital, Lahore.
Duration: 2011 to 2016
Introduction: PHPT is a common endocrine condition with a wide range of clinical manifestations differing according to geographic.
Discussion: The most common clinical presentation in our study was bone pains which were in contrast to the asymptomatic cases being most common manifestation in US and Western countries. 90% (n 36) of the patients had bony involvement while 47.5% (n 19) had renal involvement at the time of presentation.
Conclusion: Due to lack of routine biochemical screening tests in developing countries, primary hyperparathyroidism is detected late.
Primary hyperparathyroidism (PHPT) is a common endocrine condition which is manifested as elevated serum calcium levels with increased or unsuppressed serum parathyroid hormone (PTH) levels [1]. It is more prevalent in females i.e. 1:400 while being 1:1000 in males [2]. Most patients with primary hyperparathyroidism are asymptomatic with only few presented with classical signs and symptoms including bony and renal manifestations [2, 3]. The clinical presentation of PHPT may be atypical, ranging from normocalcemic PHPT to symptomatic hypercalcemia (parathyroid crisis) depending upon the severity of calcium disturbance [3].
Before 1970s, asymptomatic PHPT remained undiagnosed leading to introduction of biochemical screening tests including serum calcium level measurement [2, 4]. The classical features of PHPT i.e. bones, stones, abdominal moans and psychic groans, are common in developing countries [3]. In United States, biochemical screening results in detection of large number of asymptomatic patients, which is the most common presentation of PHPT [1-3].
A study was conducted by Castellano E et al in which clinical presentations was assessed in older age population [5]. There is no such study conducted in a developing country like Pakistan. It is important to assess the different clinical presentations and outcomes of PHPT in our country so that routine biochemical screening for serum calcium levels is implemented to facilitate early detection of asymptomatic patients.
This retrospective cross-sectional study was conducted in East Surgical Ward, Mayo Hospital, Lahore during 2011 to 2016. All the patients who underwent parathyroid gland surgery were evaluated for our study. Patients with age > 18 years and with serum calcium level > 11.3 mg/dl and serum PTH level > 55 pg/ml, both on 2 separate occasions at least 7 days apart in last 6 months, were included in our study. Patients with H/O thiazide diuretics or lithium intake, family H/O familial hypocalciuric hypercalcemia (FHH) or pregnancy/lactation were excluded from the study. A self-constructed questionnaire was filled. Data was analyzed using SPSS version 20. Qualitative variables like age and gender were represented as frequencies and percentages. Quantitative variables like serum calcium levels were represented as mean.
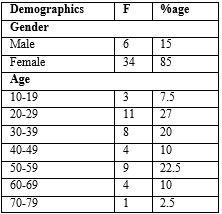
A total number of 40 patients with primary hyperparathyroidism were included in our study. Table 1 represents the demographic characteristics which show that females were 85% (n 34) higher than males i.e. 15% (n 6). Majority of them were in 20-29 years age category i.e. 27% (n 11) , with 22.5% (n 9) in 50-59 years, 20% (n 8) in 30 -39 years, 10% (n 4) in 40-49 years, 10% (n 4) in60-69 years, 7.5% (n 3) in 10-19 years and 2.5% (n 1) in 70-79 years.
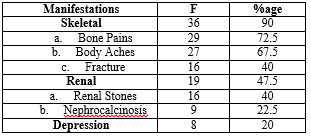
62.5% (n 25) were referred from orthopedic department, 20% (n 8) from medicine, 7.5 % (n 3) from urology, 5% (n 2) from maxillofacial, 2.5% (n 1) from neurology and 2.5% (n 1) from nephrology to our ward.As shown in table 3, 90% (n 36) of the patients presented with skeletal symptoms and 47.5% (n 19) were with renal manifestations while only 20% (n 8) of the patients had psychiatric issues at presentation.
In our study, the mean serum calcium level was 12.57 mg/dl (Normal: 8.6 – 10.3 mg/dl) while mean PTH level was 1511 pg/ml (Normal: 1.6 – 7.5 pg/ml) [6].
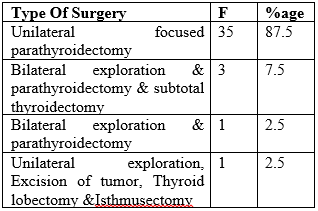
Among the surgeries done for PHPT in our study, unilateral focused parathyroidectomy, bilateral exploration and parathyroidectomy with sub- total thyroidectomy, bilateral exploration with parathyroidectomy and unilateral exploration, excision of tumor thyroid lobectomy and isthmusectomy was done in 87.5% (n 35), 7.5% (n 3), 2.5% (n1) and 2.5% (n 1) patients respectively.
Among the retrieved specimens, 95% (n 38) of them were solitary adenomas while 2.5% (n 1) were hyperplasia and 2.5% (n1) were carcinomas.

Previous studies show that primary hyperparathyroidism is commonly diagnosed on routine biochemical screening tests making asymptomatic PHPT the most common clinical presentation [1-3]. In our study, we have taken only the symptomatic patients as there is no routine biochemical screening present in developing countries like Pakistan. Like other studies, there was female predominance in our study with majority of the patients in 20-29 years of age [5, 6].
62.5% of the patients were referred from orthopedics to our ward showing that most of the patients had bony manifestations. The most common presentation in our study was bone pains i.e. 72.5% (n 29) which was comparable to study conducted by Reid LJ et al in which 27.5% of the patients presented with bone pains [6]. In contrast to our results, the common clinical manifestation in a study done by Grigorie D et al was renal involvement i.e. 51.7% [7].
The mean calcium level was 12.57 mg/dl in our study while it was slightly lower in previous studies being 11.2 mg/dl in study done by Castellano E et al and 11.3 mg/dl in that by Grigorie D et al. [5, 7].Our mean PTH level was 1511 pg/ml which much higher as compared to other studies [5-7].
87.5% (n 35) of the patients underwent focused unilateral parathyroidectomy. Histopathology revealed 95% (n 38), 2.5% (n 1) and 2.5% (n 1) of the specimens were unilateral adenoma, hyperplasia and carcinoma respectively, which was equivalent to the results shown in study by Grigorie D et al [7].
In developing countries like Pakistan, majority of the patients present late when primary hyperparathyroidism become symptomatic and patients develop debilitating features of bony and renal involvement. Like US and other western countries, routine biochemical screening tests should be implemented to aid in early detection and treatment of the disease.
The author (s) declare that there is no conflict of interest.
The author (s) received no specific funding for this study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
