
Research Article | DOI: https://doi.org/10.31579/2690-4861/470
Division of Visceral Surgery, Department of Surgery, Sion Canton Hospital, Av. du Grand-Champsec 80, 1951 Sion, Switzerland.
*Corresponding Author: Clelia Dogny, Division of Visceral Surgery, Department of Surgery, Sion Canton Hospital, Av. du Grand-Champsec 80, 1951 Sion, Switzerland.
Citation: Clelia D, Sgardello S, Fournier I, (2024), Clinical Presentation and Risk Factors of Acalculous Cholecystitis in Outpatients: Retrospective Study, International Journal of Clinical Case Reports and Reviews, 18(3); DOI:10.31579/2690-4861/470
Copyright: © 2024, Clelia Dogny. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 May 2024 | Accepted: 10 June 2024 | Published: 10 July 2024
Keywords: acalculous cholecystitis; acalculous cholecystitis - risk factors; acalculous cholecystitis – outcomes; swiss cohort; acalculous cholecystitis – histopathology
Aim: Acalculous cholecystitis (AAC) accounts for only 5-10% of cholecystitis cases, primarily studied in intensive care units (ICU) patients. The aim of this study to identify risk factors and clinical presentation of AAC in non-ICU patients.
Material and methods: We conducted a literature review using PubMed MeshTerms “acalculous cholecystitis” and searched our institution’s database (2018-2022) for “cholecystitis” and “acalculous cholecystitis,” including patients with histopathological findings.
Results: 23 patients met the inclusion criteria. based on histopathology report and diagnosis. The most common co-morbidities were cardiovascular and metabolic syndrome. Abdominal pain was the predominant complaint. Ten patients (50%) presented with elevated CRP, bilirubin, and leukocytosis. No mortality was reported at 30 days.
Conclusion: AAC in outpatients is not associated with high mortality, unlike in ICU settings. However, it is more frequent in polymorbid patients with cardiovascular risk factors.
Acute cholecystitis accounts for 3-10% of emergency room diagnoses of abdominal pain [1]. Of these, gallstones are responsible for the vast majority of cases, whilst approximately 5-10% of cholecystitis are acalculous [1,2]. Acute acalculous cholecystitis (AAC) is usually described in children, in whom it accounts for 50-70% of cholecystitis [3], and in patients within the intensive care unit (ICU), where it is associated in the literature with high mortality rates reaching 30%-50% [4,5]. Patients developing AAC within the ICU typically include males who have undergone major surgery, often vascular surgery, or who have suffered major trauma and who are intubated, ventilated, and on parenteral nutrition [6]. In these patients who are often sedated, a diagnosis is often difficult to make, with no clear clinical signs, except for increased inflammatory markers and fever [1]. Three main mechanisms are thought to contribute to acalculous cholecystitis in ICU patients. The first is an ischemia-reperfusion mechanisms involving reduced blood flow through the cystic artery, which can lead to decreased perfusion and ischemia. This is exacerbated by factors such as vasopressor medications, and hypotension. The second, cholestasis can result from various conditions such as fasting, parenteral nutrition, and dehydration causing chemical aggression of the gallbladder wall. Third, bacterial colonization occurs as a secondary phase [1].
Other causes of AAC in otherwise healthy patients can be infectious (Gram-negative bacteria, parasites, viruses), mechanical (Phrygian cap) [7], autoimmune, and cardiovascular [8]. AAC is however, relatively understudies in healthy patients. In the literature, we found a few studies focusing on AAC in outpatients or inpatients without major comorbidities. The aim of this study is to review patients who have developed AAC in outpatients or non-ICU settings, identify risk factors, clinical presentation, and compare these data with those in the literature.
Retrospective Study: We performed a 5-year (2018-2022) search in our institution’s database, le Centre Hospitalier du Valais Romand (CHVR), Citrix_ HVS with the terms “cholecystitis” and “acalculous cholecystitis”. The inclusion criteria for the retrospective study included adult patients with a confirmed diagnosis of AAC by either ultrasound (US) or computed tomography (CT) scan and confirmed at pathology. Exclusion criteria included patients hospitalized within the intensive care unit (ICU), those with AAC resulting from multiorgan failure, and those lacking histopathological evidence of AAC.
Literature Review: We performed a literature review using the PubMed Mesh Terms “acalculous cholecystitis” from march 2023 to June 2023.
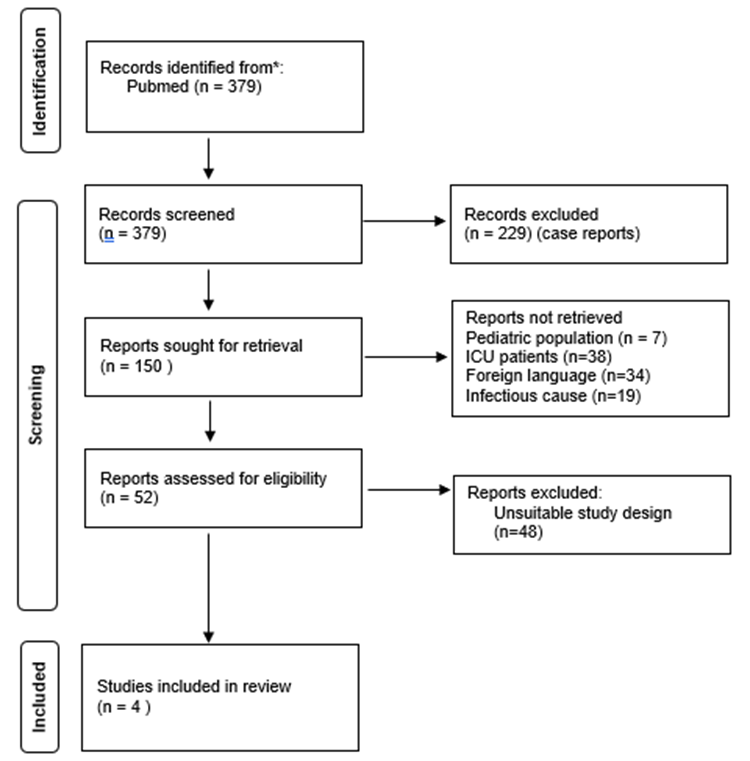
Figure 1: Selection of articles, excluding, articles focusing on intensive care patients, in foreign language or with unsuitable study designs
Literature review:
The literature review initially yielded 379 results. Of those, 229 were case reports, 148referred to the pediatric population, ICU patients, had infectious causes or were written in a foreign language, 48 had unsuitable study design. Only 4 were studies focused on AAC in outpatients abd were conducted between 1989 and 2012. Three were retrospective and one of was a prospective study (2,9–11) (Figure 1 & Table 1).
| Authors | Savoca et al.(9) | Ganpathi et al.(10) | Ryu et al.(11) | Nikfarjam et al.(2) |
| Publication Year | 1989 | 2006 | 2002 | 2012 |
| Number of patients | 47 | 11 | 22 | 35 |
| Ratio (M/W) | 36:11 | 9:2 | 15:7 | 18:17 |
| Male % | 77% | 82% | 68% | 51% |
| xAges (years) | 65.5 (27-89) | 52.4 (30-69) | 63 (40-85) | 69 (45-94) |
| Outpatients (n) | 36 | 11 | 20 | unknown |
| Inpatients (n) | 4 | - | - | 2 |
| ICU (n) | 7 | - | - | - |
| Presentation | ||||
| RUQ pain (%) | 83% | 73% | unknown | 25% |
| Fever (%) | 55% | 27% | unknown | 46% |
| Leukocytosis (%) | 96% | 81% | unknown | 34% |
| Co-morbidities | ||||
| No-co-morbidities | unknown | 36% | 60% | unknown |
| Hypertension (%) | 56% | 45% | 25% | unknown |
| Diabetes (%) | 15% | 18% | 20% | 23% |
| CV risk factors (%) | 72% | unknown | 35% | unknown |
| Diagnostic | ||||
| US (n) | 18 | 10 | unknown | unknown |
| CT (n) | 3 | 2 | unknown | unknown |
| HIDA scan (n) | 36 | - | unknown | unknown |
| Histopathology | ||||
| Necrotic (%) | 28% | 36% | 63% | 37% |
| Perforated (%) | unknown | unknown | 13% | unknown |
| Mortality (%) | 6.4% (ICU) | 0% | 0% | 0% |
Table 1: Summary of results from previous studies. RUQ: right upper quadrant, CV: cardiovascular
Retrospective Study
23 of the 115 patients who were initially identified were included in this study (Table 2). We excluded 70 patients because of coding errors or the presence of gallstones following the pathology exam or during the operation, 20 additional cases were treated conservatively, without histopathological confirmation of the AAC. Of the 25 patients diagnosed with AAC, we excluded two, one was an ICU inpatient, and the other was a long-term inpatient with significant vascular co-morbidities and multi-organ failure. The patient cohort included patients between 48 and 87 years of age (mean age was 75 years), 22% were female (5/23) and 78% were male (18/23).
The outpatients cases were 19 and 4 developed symptoms during their hospitalization. 3 of them had their gallbladder removed in an elective setting, rather than at the first presentation due to initial conservative treatment. Amongst inpatients, three were post-operative patients, (orthopedics, urological, and visceral surgery) and the latter was a cardiology patient who was hospitalized for investigations of basithoracic pain. The most frequent co-morbidities were cardiovascular: arterial hypertension [11] and ischemic heart disease [8] as well as metabolic risk factors for cardiovascular disease such as diabetes [7] and hypercholesterolemia [10]. Four patients had no comorbidities (Table 2) The patients were mainly ASA III (57%), following ASA II (30%) only three were ASA IV (13%).
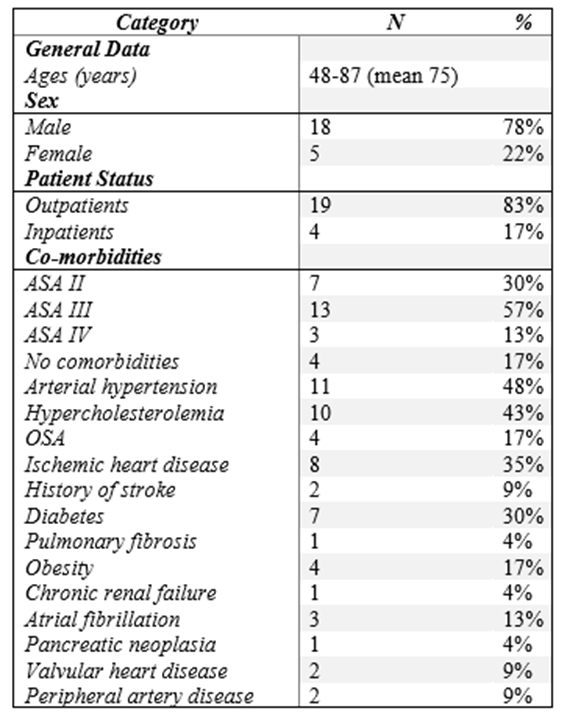
Table 2: patients’ co-morbidities OSA: obstructive sleep apnea, CRF chronic renal failure, PAD: peripheral arterial disease
The most common complaint was abdominal pain (18). 4 patients had basithoracic pain and one presented with delirium. We considered the
presence of leukocytosis (>10 G/L), CRP (>5mg/L) and total bilirubin (>17µmol/L) at patient admission, we did not include the three post-
operative patients in these results since leucocyte counts and CRP are increased postoperatively. Ten patients (50%) presented to the emergency department with an increase of at least two of three biological markers, six (30%) presented with an alteration in only one of the three biological markers, and four (20%) patients did not present any biological alteration. Abdominal US and CT were the primary imaging modalities. Thirteen patients underwent both exams, five were diagnosed with US alone, and four with CT alone. One patient required MRCP following an inconclusive US to diagnose a thickened gallbladder wall.
Regarding management, four patients had an intravesicular transhepatic drain placed before surgery. Three subsequently had elective laparoscopic cholecystectomy, and one within 24 hours. The remaining patients underwent cholecystectomy at presentation. A laparotomic approach was repeated in two inpatients who had already undergone a previous laparotomy during their same hospitalization; no conversion to laparotomy was reported in the other patients who underwent laparoscopic surgery. At the histopathological level, half of the cholecystitis (12/23) were described as acute cholecystitis, seven were necrotic with one being perforated, and five ulcerophlegmonous. The rest were chronic with eight described as acute attacks of chronic cholecystitis, two were perforated. No malignancy was reported, and all were described as acalculous on histopathological final analysis. Upon discharge, 3 patients were admitted for rehabilitation, and 20 were discharged home. No mortality or morbidity greater or equal than Clavien-Dindo III was reported up to 30 days post-operative, one patient developed pneumonia treated with antibiotics.
From an epidemiological standpoint, the characteristics of this study's population align with other studies. The majority of patients were male (18:5, 78%), consistent with literature values ranging from 51% [2] to 82% [10]. Patients in this study were older (average age 75years) compared with an averages of 52.4 [10] to 69 [2] years of age. The ICU patients were excluded from the study, but they represented only two patients out of 25. Savoca et al [9], which also included ICUs patients, described only 15% of AAC from ICU patients. Most of our patients were ASA III (57%), which suggests that this pathology concerns more polymorbid patients.
The main identified risk factors for the development of AAC were cardiovascular risk factors with diabetes II (30%), hypertension (48%), hypercholesterolemia (43%) and ischemic heart failure (35%) being the main co-morbidities. Hypertension was frequently found to be the most frequent co-morbidity in the literature. However, diabetes was slightly more prevalent in our study (30% vs. between 15% and 23%) [2,9]. It is however interesting to notice that we found up to 17% of patients without known co-morbidities, which is less than other studies (up to 60% [11]). This highlights the fact that AAC can occur in healthier patients and not just in the initially identified group of ICU patients. However, since patients who were treated conservatively were excluded from the study, there could be a selection concerning the proportion of patients without co-morbidities.
The impact of cardiovascular disease in AAC can be partly explained by what is known about its pathophysiology. Several studies report two main mechanisms for AAC namely ischemia-reperfusion injury and chemical injury with biliary stasis and infiltration of bile into the wall of the gallbladder [1,12]. Both mechanisms are histologically reported by Laurila and al. Ischemia-reperfusion is identified via the presence of leukocytes at the margin of blood vessels, similar to what is found in myocardial infarction. In outpatients, the prevalence of cardiovascular diseases, may be correlated with advanced visceral atherosclerosis [12] which, with a small drop in flow, could cause ischemia-reperfusion injury. The mechanism of ischemia-reperfusion in ICU patients is also due to the use of vasopressors and the state of shock inducing vasoconstriction of the terminal cystic artery. In the same study, chemical injury through bile infiltration in the wall of the gallbladder was described, indicating endothelial disruption or biliary stasis. For ICU patients, biliary stasis is partially due to parenteral nutrition and a nil by mouth (NBM) diet. In outpatients this mechanism seems less important. Furthermore, infectious, and parasitic causes were found in the literature for outpatients, including some tropical diseases (Appendix 1). These pathologies were not found at histopathology in our study, which focus on diseases that are present in Europe.
An interesting point, which is similar to the ICU patients, was the relative difficulty in making a diagnosis. At presentation, while most patients presented with the classic right upper quadrant pain, only 50% of patients presented with two elevated biomarkers, and half of the remaining patients either presented with only one or no biomarker alteration. While studies have shown leukocytosis in over 80% of patients[9,10), our study found it in only 60% of patients. Right upper quadrant pain, whether associated with leukocytosis or not, seems to be the main decisive factor requiring further investigation.
Abdominal US is considered the diagnostic technique of choice with the diagnostic criteria being a thickening of the wall of 3.5mm [13], peri-vesicular fluid and gas in the wall [14]. CT has been shown to have good specificity, allowing to rule out cholecystitis [15]. The hepatobiliary iminodiacetic acid (HIDA) scan also known as cholescintigraphy which has been mentioned in several studies, is used to study the dynamics of bile flow [1]. It is a time-consuming exam and is not an exam of choice for diagnosis in the emergency department.
Histopathology, on all the AAC, three were perforated (13%) and nine were necrotic (39%), similar results were found in the literature, with necrotic AAC representing (28-63%) in outpatients. Ryu et al. [16] found the same rate of perforation 13% with 68% of necrotic cholecystitis.
This study faces limitations primarily from the small sample size, which is inherent to the relative rarity of the disease. Additionally, since we included only patient which an histopathological confirmation, we may have excluded patients for whom conservative management of AAC was opted. This approach could have led to the exclusion of more polymorbid patients.
In this study, we had no mortality reported at 30 days, which is in line with what was found in other studies, only Savoca et al [9] reported death in the specific subgroup of patients from ICU. This supports the already-mentioned hypothesis that AAC is not a fatal disease in itself but is made more deadly by the difficulty and delay in diagnosis and the severe co-morbidities of ICU patients [2,10,16].
In this study we found that acalculous cholecystitis in outpatients does not exhibit the high mortality rate previously attributed to it, aligning with findings from prior studies. However, it is more frequent in poly-morbid patients with cardiovascular risk factors, but can also occur in healthy patients. We highlighted that this diagnosis should not be underestimated in particularly in the emergency department. Clinical setting and presentation are roughly standard and should provide an opportunity for prompt treatment. Regardless of the sample size this study provides a good sample of the European cohort presenting with AAC and provides support for surgical management to avoid complication due to AAC (perforation and necrosis) and favorable post-operative outcome.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
