
Research Article | DOI: https://doi.org/10.31579/2637-8892/025
Department of Psychological Medicine, Zahraa University Hospital, Nigeria.
*Corresponding Author: Ahmed Shawki, Department of Psychological Medicine, Zahraa University Hospital, Nigeria.
Citation: Ahmed Shawki, Clinical practice of Headache: The Patient’s Education. J. Psychology and Mental Health Care 2(2); DOI: 10.31579/2637-8892/025
Copyright: © 2018 Ahmed Shawki. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 March 2018 | Accepted: 20 April 2018 | Published: 25 May 2018
Keywords: headache; referral; diagnostic imaging; anxiety; emergency medical services
Introduction: Headache is the commonest reason for neurology referrals, and the commonest neurological reason for patients attending Emergency Departments (EDs). An ethical approach to health care requires that patients be provided with informed choice about management. However researchers have not addressed patients’ concerns and choices in managing headache. This study aims to describe the views of patients, their fears, use of EDs, their perceived need for a scan and its outcome for them.
Methods: A qualitative study using semi-structured interviews with 19 adults aged 23-63, referred by Family Practitioners (FPs) to neurologists for primary headaches approximately two years previously. Audio-recorded interviews were transcribed and analysed thematically.
Results: Participants described fears about secondary organic causes for headache, like a brain tumor. They described their headaches as stressful, and leading to a vicious cycle of fear. Many believed they needed a brain scan and requested it. Participants reported relief of their fears after a scan, and in some cases relief of headache symptoms.
Discussion: UK FPs now have open access to brain scanning, which may relieve physical concerns. Interventions to address health-related anxiety may also help some consulters for headache.
In the diagnosis and management of patients, doctors are asked to respect four principles, to:- provide patients with informed choice (autonomy), cause no harm (non-malificence), do good (beneficence), and promote justice, which includes fair, cost-effective allocation of scarce resources [1]. The last principle is salient in most western countries where health care is funded as a public service. Guidelines for physicians tend to focus on management with medicines [2]. How to apply the principles to decisions like investigation and referral to specialists is under-investigated and challenging, particularly for doctors presented with headache.
It has been argued that scanning patients for headache, whether it is by computer tomography (CT) or magnetic resonance imaging (MRI) may do more harm than good [3]. Incidental findings are common, particularly with MRI, occurring in 2% of scans of people with no neurological symptoms [4]. When patients consult a primary care physician for an undifferentiated headache, the 1-year risk of a malignant brain tumour is 0.15%, rising to 0.28
Design
This qualitative study, which was nested in a prospective cohort study, sought to provide a detailed knowledge of the views and experiences of patients with headache who had been referred by their FP to a neurologist. Qualitative methods were ideally suited for such hitherto unexplored research topics as participants are able to raise what they personally regard as important aspects and concerns rather than these being specified in advance by the researcher. The South-East Multi-Centre Research Ethics Committee approved the study (MREC01/01/032). Informed consent was obtained from all participants.
Recruitment: Participants were recruited from a cohort of 48 adults (aged > 18 yrs) with headache who were prospectively recruited after they had been referred by their FP in the south of England to a neurologist for headache.[11] This mean age of participants in this sample was 41and 64% % were female. We slightly over-sampled men given their smaller numbers in the cohort and selected individuals with a similar age distribution as the cohort. These patients were approached by letter to participate in this interview study with a response slip. A follow-up phone call was made to non-responders.
Data collection: Semi-structured interviews undertaken by a researcher independent of the cohort study (LJ), lasted on average 45 minutes, and were conducted in a location of the participant's choice. A topic guide was used to frame the interviews. This was developed on the basis of themes identified from the literature and refined through open interviews.
The main themes covered were patients’ experience of having a headache disorder and its impact on their lives, including their fears and concerns; their use of hospital Emergency Departments, whether they had been referred for a scan, how this had occurred and how helpful this had been. Interviews were conducted on average two years after referral to a neurologist to provide a long term perspective. Participants were encouraged to talk freely and the interviewer probed and prompted responses as required. Information of the participants’ headache diagnosis was from the database of information collected for the cohort study in which these people had previously participated. [11].
Data analysis: Interviews were audio-recorded and transcribed verbatim. Data were entered into NVivo 9 a computerized qualitative analysis package. FN read each transcript line-by-line and generated codes through open coding. These codes were then categorized thematically and relationships between themes were identified through a process of constant comparison, with particular reference to explanations for patients’ decision making and the beliefs and experiences of ‘deviant cases’. LR, AN and MM reviewed the codes and categories and discussed emerging interpretations.
Sample Characteristics
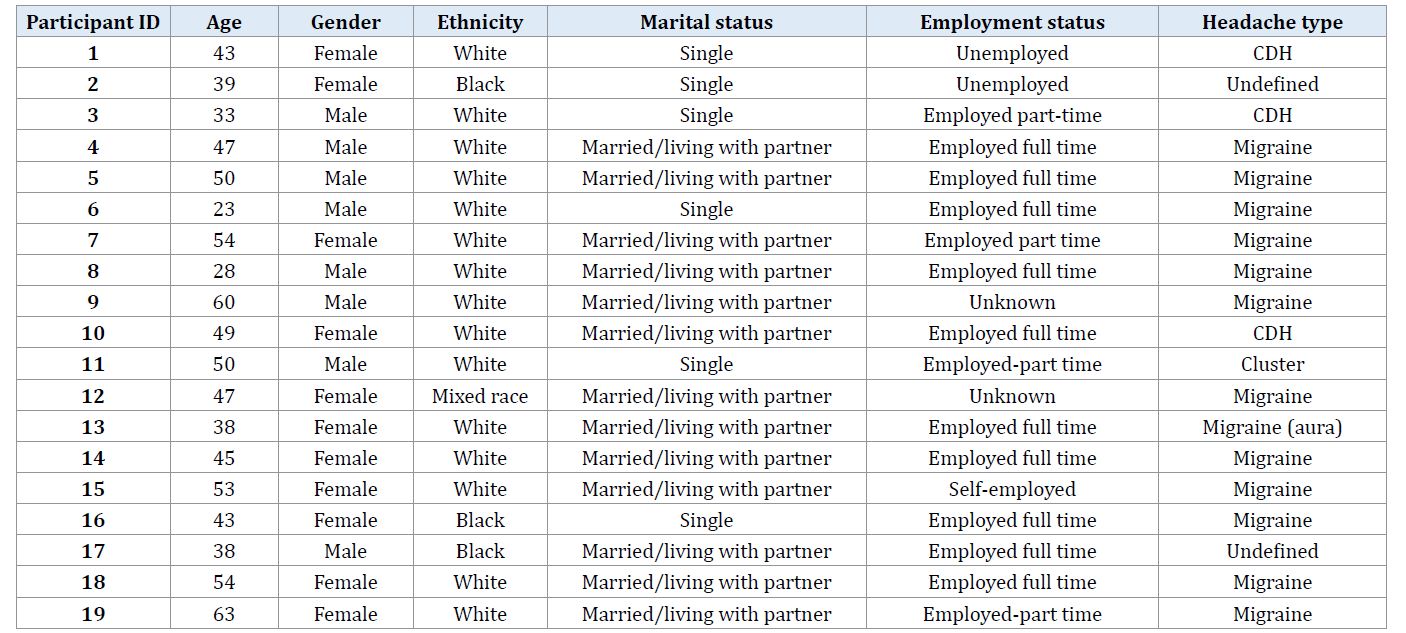
A total of 19 people comprising 8 men and 11 women were interviewed (Table 1). Thirteen had been categorized as having migraine, three chronic daily headaches and three as ‘other headache’.
Analysis of the transcripts provided insights into patients’ fears about the cause of their headache and the implications that this had for their use of different health care services. Three key themes were identified. These were: headache-related fears and use of emergency departments; perceived need for a scan; and the outcome of a scan in terms of perceived reassurance. Quotations are presented to illustrate themes.
Headache-related fears and use of Emergency Departments
Patients generally identified fear about what their headache might mean as a key issue prompting service use. One patient mentioned her worry and anxiety reaching up to a point: ‘It’s a, what’s called a tipping point really I think, you know if you think of catastrophe theory that something will grow up to that point and suddenly it will tip.’ (P.12, Female, 47).
For 3/19 participants, severe headaches made them resort to Emergency Department (ED) visits to a hospital after they had seen the FP. One said: ‘the one that was really frightening I ended up in X Hospital because it developed into what I thought that I might have been having a heart attack, because I was so worried about the headache’. (P.5, Male, 50).
Continuous headache also led relatives to act on the patient’s behalf. One said: ‘it was like a continuous thing every weekend…my parents would take me up the hospital, thinking there was something wrong, and what it was, was migraine.’ (P.6, Male, 23).
Perceived need for a scan
Worry about a serious medical problem led ten participants to ask their doctor for a brain scan. Altogether eight of these patients received a scan subsequently. Before the scan, these patients described consistent fear of a possible physical cause, mainly a brain tumour. Patients described their headache as not reducing after advice given by their FP, and believed they needed to persist to get their doctor to arrange scan.
‘...I wanted to be treated. I wanted somebody to tell me that I wasn’t gonna have a brain tumour and fall down dead.’ ‘...But I actually found I had to push for a scan, I had to insist on it almost, and yet that was the thing that had been the most worrying right from the very beginning... I had to insist on something, something physical being done.’ (P13, Female, 38).
These patients generally explained that they had been referred for a scan for peace of mind: ‘Yes because I got so worried because it had gone on for so long and they said we’ll send you for one for peace of mind, we’re saying we know there’s no problem up there, but for peace of mind for you we’ll send you for one.’ (P.7, Female, 54)
An additional three participants who had been referred and seen a neurologist reported having brain scans that were initiated at the request of a neurologist, rather than themselves.
The outcome of a scan in terms of perceived reassurance
Following the scan, 6/8 of the participants who reported asking for a scan, stated that their anxiety, stress, and worry had reduced considerably, and described themselves as ‘relaxing a bit’. Three of these patients reported that normal results from the scan reduced their headache symptoms also: ‘But I think I had the scan to put my mind at rest. I knew that there was nothing serious about it. But perhaps even that may have made the fact that it’s tailed off, you know, sort of eased it on its way sort of thing.’ (P19, Female, 63).
After the scan one participant reported the headaches diminished to such an extent they were no longer consulting their doctor.
Summary of main findings
We found most people with headache who were referred for a scan described fears about a physical cause for their headaches, in particular a brain tumor. Patients believed they had needed to put pressure on their doctors to get a referral for a scan. They typically described feeling relieved after a normal scan, with one reporting alleviation of headache symptoms altogether. After a scan most felt they had the confidence to use other strategies to manage their headache.
Strengths and limitations of this study
This qualitative study consisted of interviews with men and women recruited from a large cohort of patients who had been referred for headaches about two years earlier [11]. It is one of few qualitative studies to explore patients’ ideas and experiences about headache [13]. It is the only one we know to explore patients’ views about their role in decision-making about referral and investigation by a neurologist. It was not large, and no participants reported scans leading to incidental findings which might potentially increase their anxiety.
Relationship to other studies
We previously interviewed FPs to determine their views of reasons for referral, and found they felt patients pressured for a scan mostly because of fears of an organic cause [12]. Some of our participants described a cycle of worry which included visits to the ED. Headache is a common neurological reason for ED visits, which is something health services planners are seeking to reduce owing to their high cost. After scanning our participants reported their fears were reduced, and sometimes their headache symptoms too. These findings add depth to evidence from a trial which found that scans do not on average increase patients’ fears [14]. In this trial the fears of those scanned were reduced after 3 months [14]. Health services for patients who were randomized to no scan cost more, as those denied scans were more likely to have visited another neurologist, with up to a third being given a scan later [14].
It has been suggested that up to a third of patients referred to neurologists, particularly those with headache have symptoms unexplained by organic disease [15], with an implication that addressing health anxiety is important also. Some of the participants in this study described health anxiety, and some resorted to visiting the hospital on an emergency basis. There is evidence that, in addition to conventional therapy, relaxation, behavioural and cognitive-behavioural management may help people with headache and migraine, particularly when it is associated with anxiety [2,16,17].
Implications for clinical practice and research
If doctors wish to respect patient autonomy, our evidence suggests some patients choose a scan. Communication about the likelihood of negative results, false positives results and cost, would also contribute to informed consent. Our participants were interviewed an average of two years after referral to a neurologist. They reported a negative result had helped relieve their fears, and move on to self-management. Open access to brain scanning for doctors working in primary care may reduce anxiety, reduce cost and increase access to neurologists for other patients. More research is required to determine whether patients with health-anxiety, who are additionally offered relaxation and cognitive-behavioural can reduce headache and improve quality of life. We are currently exploring this by means of a trial (NIHR PB-PG-0610-22373).
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
