
Research Article | DOI: https://doi.org/10.31579/2578-8949/021
*Corresponding Author: Prashansa Jaiswal, Department of Dermatology,Venereology and Leprology, ESIPGIMSR, Basaidarapur, New Delhi, India.
Citation: Sundeep Chowdhry MD, , Prashansa Jaiswal MD,Paschal D’ Souza MD, Tapan Kumar Dhali MD, Clinical Photography in Modern Era-Assets and Liabilities J.Dermatology and Dermatitis, DOI:10.31579/2578-8949/021
Copyright: © 2018 Sundeep Chowdhry et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 January 2018 | Accepted: 02 March 2018 | Published: 09 March 2018
Keywords: Clinical photography ,dermatological pathology ,digital photography
Background: Clinical photography has long been an important aspect in the management of dermatological pathology and has many applications in contemporary dermatology practice .With the continuous evolution of digital and smartphone technology, clinicians must maintain ethical and medico-legal standards.
Objective: This article reviews how dermatologists are utilising this technology in their clinical practice and what procedures they follow when taking clinical photographs of patients. It also discusses the ethical and legal considerations of clinical photography in dermatology.
Methods: A questionnaire based method was used to obtain information from a sample size of 100 dermatology doctors. Both personal and telephonic interviews were taken in regard to use of personal smartphones and digital equipment for photographing patients in their clinical practice. They responded pertaining to questions on consent for photography, applications of clinical photography, sharing and storage of images, security of devices and display of images taken by the patients themselves prior to consultation.
Results: All the dermatologists (100%) responded to the survey. Only thirty three (33%) dermatologists obtained verbal consent for photography from their patients prior to taking their photographs. The main reasons for taking photographs was to seek advice from their peers/consultant (68%). All dermatologists used their smartphone. Twenty three respondents (23%) had security enabled features in the equipment used for patient photography. Thirty (30%) dermatologists reported patients sharing images with them that they themselves had taken prior to the consultation.
Conclusion: In view of confidentiality one must practice orthopraxy in view of better patient care and concern.
Photography has been accepted for decades as a standard tool for documenting dermatologic conditions and as an adjunct to their treatment, in both medical practice and research. Clinical photography is the cornerstone of appropriate dermatological documentation in case reports, for monitoring patient’s therapeutic response in day to day practice, clinical trials and for research development. The emergence of low-cost easy-to-use digital imaging systems has made good-quality photography more accessible to practitioners.
Photography plays an important role in professional communications, practice development, and medico legal issues. With the realms of digital photography and its medical applications continuously expanding and becoming more and more sophisticated and readily accessible, it is necessary to strive so as to maintain, if not improve the medico-legal and ethical standards of the practitioners who employ it. Patient consent, confidentiality and privacy are of paramount importance and care should be taken to ensure they are not sacrificed for the sake of ease and convenience. This study aimed to elicit information on common aspects of clinical photography among dermatologists and discusses the ethical and legal issues related to this commonly used modern era technology.
This article reviews how dermatologists are utilising this technology in their clinical practice and what procedures they follow when taking clinical photographs of patients. It also discusses the ethical and legal considerations of clinical photography in dermatology.
A questionnaire based method was used to obtain information from a sample size of 100 dermatology doctors including consultants in government institutions and private practice and dermatology trainees/residents. Both personal and telephonic interviews were taken as per their availability in regard to use of personal smartphones and digital equipment for photographing patients in their clinical practice. They responded pertaining to questions on consent for photography, applications of clinical photography, sharing and storage of images, security of devices and display of images taken by the patients themselves prior to consultation.
All the dermatologists (100%) responded to the survey. Of these 45 (45%) were males while 55(55%) were females. Out of 100 surveyed, 73(73%) were dermatology trainee/residents while 27(27%) were consultants. Among consultants, six had experience of 1 to 5 years, 12 (12%) had experience of 6 to 10 years while 9 consultants had experience of more than 10 years. Seventy four (74%) were working in government institutions while 26(26%) dermatologists were in private practice. Out of 100 dermatologists, 65(65%) were interviewed personally while 35(35%) responded telephonically. Only thirty three (33%) dermatologists obtained verbal consent for photography from their patients prior to taking their photographs. Of the 100 dermatologists surveyed, majority 73 (73%) of them maintained privacy of patients photographs by hiding their identity mark(s) although no specific guidelines were followed in obscuring the identification marks.
The main reasons for actively taking clinical photographs of patients given by the dermatologists was to seek advice from their peers/consultant (68%) and for monitoring the treatment/ disease (60%). This included comparison of the pre and post treatment scenario of the disease process. Rest 40(40%) gave reasons to share their experience / knowledge with their colleagues, 24(24% undertook photography) for primarily teaching purposes and 16(16%) solely used the same with the intent of research publications (Figure. 1)
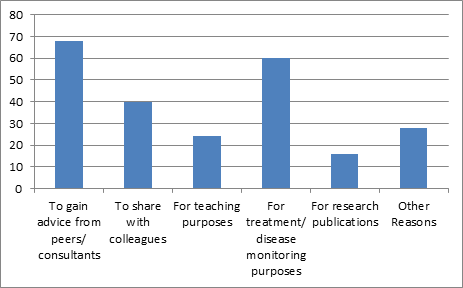
Twenty eight (28%) gave other reasons for clinical photography in which recall was the most common followed by intent to maintain records. Dermatology trainees/residents took photographs mainly to gain advice from peers while consultants took them for teaching purposes. Of those surveyed, 38% (38) reported texting or sending images through email to their colleagues for advice or opinion. A mere twenty two (22%) respondents reported routine disclosure to the patient about the identity of the third party with whom their image would be potentially shared in future. On sharing clinical photographs with third party, forty eight (48%) respondents reported being inconsistent with patient disclosure regarding the identity of the third party with whom the images were eventually shared.
All those surveyed (100%) reported using only their smartphone for taking clinical photographs of patients. Of these, 88 dermatologists (88%) reported storing over 100 images of patients on their personal smartphones, sixty five (65%) of which had more than 200 patients’ images stored in the memory of their smartphones. In addition, 70% of respondents also reported the use of personal digital camera in consultation process. Only twenty three respondents (23%) reported having security enabled features in the equipment that they used for patient photography. Thirty (30%) dermatologists reported that they had experienced patients sharing images with them that they themselves had taken prior to the consultation.
Photography provides a unique opportunity to document the patient's initial presentation which represents a baseline and to ascertain progresses in the condition subsequent to treatment. Photographs taken over a period of time, or at specific end points, provide an undisputable medical record that enables clear communication with patients regarding their clinical improvement or deterioration and provides the practitioners with permanent documentation of the efficacy of treatment modality.
An archive of clinical images documenting their work including various rare entities can be a valuable asset for dermatologist. It needs no justification that for professional publications or presentations, photography is indispensable. If practice includes aesthetic procedures, clinical photography demonstrating the results can be used in marketing and promotional materials or even simply arranged in a sequential order in a binder to show prospective patients [1] who are inquisitive and concerned about the progress of the disease and merits of the treatment protocol.
In contemporary medical practice patient autonomy is widely regarded as a primary ethical principle. All patients are entitled to the fundamental right so as to know what will eventually happen to their clinical photographs subsequent to disease management [2,3].In the modern world wherein patient are becoming increasingly educated and motivated not only to be actively involved in their treatment but also continually and periodically monitor the progress ,it becomes necessary to relook at issues of documentation of clinical photography[2]. The doctrine of informed consent is the cornerstone of the patient–clinician therapeutic partnership and encompasses both ethical concepts and legal requirements [4]. Consent may be obtained in several ways. It may be express or implied consent [5]. Express consent refers to consent that is clearly and unmistakably stated, and can be obtained either in writing, verbally or any other form where the consent is clearly communicated [6]. It is globally accepted that express written consent is required for complex or complicated treatments and major interventions. It has been argued that taking clinical photograph of patients although not a treatment can have an indirect constructive effect on treatment by aiding in diagnosis. Hence, the need for photographic consent could be considered analogous to the widely accepted requirement of written patient consent for treatment such as that employed commonly for surgical procedures [5].
Though conversely, it could be argued that there is an element of implied consent in the case of clinical photography. The patient who is presenting himself or herself willingly for an appointment and provides/elaborates all physical information, including photographs which when later assorted by clinician in due course of time for their consultation can be considered as part of the patient’s composite medical record [7]. Maintenance of medical records is a routine practice in interest of the patient and does not require explicit consent from the patient. Consent to keep medical records is implied by the patient simply by seeking an attending their appointment and attending the clinicians clinic[4,7] .Further, if patients willingly position themselves for a photograph, it can be argued that the patient has given implied consent for the photograph. Implied consent is usually reserved for routine treatment and procedures that facilitate pathological investigations such as phlebotomy[2].It can be argued that in current dermatology practice photography has become a routine aspect of management where the actions of the patient clearly imply consent for his/her clinical photograph, if the need so arises.
Clinicians should have a sound understanding of the requirements of valid informed consent. Although there has not been any case of legal action related to consent regarding clinical photography in India but in 2010 a Malaysian court heard the legal case of a colorectal surgeon who had taken clinical photos preoperatively and postoperatively. The surgeon had intended to use the patient’s photographs as an aid to haemorrhoid patient education; but, due to the lack of informed consent the surgeon’s actions were viewed by the court as an invasion of the patient’s privacy and it subsequently awarded damages in favour of the patient [8].
While clinical photography facilitates improved patient care, the escalation and rampant emergence of smartphone and digital photography and its subsequent use by clinicians has led to a relaxation in informed consent practices. In order for consent to be fully informed, clinicians must discuss their proposed use of clinical photographs with patients. Prior to providing their consent, patients should have an understanding of how their image may potentially be used in the future not only for their treatment but also for soliciting advice from a third party and even for education and/or for publication[4] .It may be argued that in order to provide full disclosure on the use of the patient’s image, clinicians must also ensure that the patient is informed about (i) exactly who will be allowed to view the photograph; (ii) if and how the images will be identified and how the patient’s personal identity will be protected; (iii) how the images will be stored, and (iv) how long the clinician plans to retain them and lastly (v) if there are plans for developing further copies which will be made and distributed.11When photographs are taken in the absence of fully informed consent, it can be reasonably argued that the patient’s right to privacy has been violated by the treating practitioner[5].
Of all forms of medical documentation, clinical photographs have the greatest potential to cause mental distress to the patient. Some patients who consult dermatologists have put in substantial efforts to hide or masquerade the very disease for which they have presented themselves for the treatment [5,8].It is observed in clinical practice that patients exhibit inhibition to expose and reveal lesions on genitalia. Though the disease is a cause of grave concern and anxiety for the patient on one hand but on the other hand he/she is reluctant not only to reveal but also to show photograph of the same. Similar condition may be encountered in patients of vitiligo on exposed parts which are concealed with use of camouflaging agents and these patients do not want to expose their vitiliginous skin even to treating dermatologist, Medical images of patients can usually be taken in such a way so as to avoid their identification by other viewers but at times in dermatology this is often becomes difficult. Skin lesions on the face can make it impossible to avoid the inclusion of the patient’s eyes in the clinical photograph of the face. Also inclusion of the surrounding facial anatomy and structures is important as it has relevance to plan the medical and surgical management of the existing disease/pathology. Unique tattoos, scars and body piercings also present challenges to the protection of patient anonymity [9].
Communication networks allow the increasingly swift and easy distribution of information between users. In recent times there has been growing concern from the community regarding the safety of data transfer and sharing[4] .With regard to clinical images of patients, clinicians should ensure the images are protected and avoid distributing them to parties who are not involved with the decision making process on the patients’ treatment and care. It is widely accepted that doctors have both an ethical and a legal duty not to disclose personal information about their patients to third parties without the patients’ consent or any legal authority to do so.
It has become common practice for dermatology registrars to e-mail or text (via multimedia message services) images to peers for their opinion and review. Patients who consent to the sharing of their image between clinicians so as to aid or confirm their diagnosis should be given assurance that their confidentiality will be preserved in the process of telecommunication exchange. The clinicians receiving images for a second opinion are bound by the same ethical and legal regulations as those taking the images initially [7].
Storage of images on digital cameras and smartphones compromise their protection if extra security measures are not put into place. Most digital cameras do not have the option of a security pin number. To ensure the protection of the images, they should be stored on digital cameras for short periods only. Downloading images onto a computer or data storage device with password or pin protection soon after they have been captured is one solution. Although this may become laborious for clinicians who take numerous images, a routine practice of regular downloading should be initiated.
With the increasingly widespread availability and affordability of digital technology, patients are more and more commonly presenting to for consultation with images of their skin lesions that they themselves have taken prior to their visit. Photographs taken by patients can be helpful for the diagnosis of dermatoses that may be transient, recurrent or in anatomical areas which the patients do not want to exhibit openly the clinician [10] .If patients share their images with a clinician there is an element of implied consent; however, should the clinician want copies of the image, informed consent on how the image will be used and further processed/analysed should still be obtained, as described above.
A significant disadvantage of seeking medical option and diagnosis merely on basis of clinical photography through whatsapp and digital forums is that it can often generate wrong opinions and misdiagnosis in absence of real patient. This spreads virally to the detriment of the patient and novice dermatologists. Hence improper photography has the potential to do more harm than good.
There is a shift towards photographic consent being obtained verbally from the patient rather than in written format. Indeed, current technology allows the clinician to take multiple images of a patient during a consultation in less time than it would take to administer a formal written consent document. Failing to take the time to obtain and document informed patient consent for photography may leave the practitioner open to legal liability and paucity of time will not be a valid excuse in court of law. In view of confidentiality one must practice orthopraxy in view of better patient care and concern. Taking a consistent and careful approach so as to obtain valid informed consent from patients, maintaining adequate medical records and providing secure systems for data storage assists the clinicians to ensure patient confidentiality and maintain a sound patient–clinician therapeutic partnership along with protecting practitioners from possible disciplinary and legal action
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
