
Review Article | DOI: https://doi.org/10.31579/2768-0487/037
*Corresponding Author: Gian Maria Pacifici, Associate Professor of Pharmacology,via Sant’Andrea 32,56127 Pisa,Italy.
Citation: Gian M Pacifici. (2021) Clinical Pharmacology of Propranolol in Infants and Children. Journal of Clinical and Laboratory Research. 3(3); DOI:10.31579/2768-0487/037
Copyright: © 2021 Gian Maria Pacifici. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 July 2021 | Accepted: 07 August 2021 | Published: 18 August 2021
Keywords: propranolol; dosing; efficacy; safety; effects; adverse-effects; metabolism; pharmacokinetics; drug-interactions; prophylaxis; treatment; trials; placenta; breast-milk; infants; children
Propranolol is α nonselective β adrenergic receptor antagonist with equal affinity for β1 and β2 adrenergic receptors, lacks intrinsic sympathomimetic activity, and does not block α receptors. Propranolol is absorbed following oral administration and consists in two enantiomers, the (-) enantiomer is the active form and is cleared from the body more slowly than the inactive (+) enantiomer. Much of propranolol is metabolized in the liver and the metabolites of propranolol are 4-hydroxypropranolol, 5-hydroxypropanolol, N-desisopropranol, and propranolol β-D-glucuronide. The oral dose of propranolol hydrochloride is 250 to 750 µg/kg thrice-daily in infants and in children it is 200 to 500 µg/kg thrice-daily or 4 times-daily. Propranolol has been found efficacy and safe in infants and children but may induce adverse-effects. The elimination half-life of propranolol is about 15 hours in term and preterm infants and the distribution volume of propranolol is larger than the water volume. Propranolol interacts with drugs. Halofenate, phenytoin, phenobarbitone, rifampicin, and ethanol which affect the clearance of propranolol, and chlorpromazine and cimetidine inhibit the metabolism of propranolol. The prophylaxis, treatment, and trials with propranolol have been extensively studied in infants and children. Propranolol crosses the human placenta but it does not equilibrate between the maternal and foetal compartment and migrates into the beast-milk. The aim of this study is to review the published of propranolol dosing, efficacy and safety, effects, adverse-effects, metabolism, pharmacokinetics, interaction with drugs, prophylaxis, treatment and trials in infants and children and propranolol transfer across the human placenta and migration into the beast-milk.
The β adrenergic receptor antagonists are classified as non-subtype-selective (“first generation”) β1 selective (“second generation”), and non-subtype- or subtype-selective with additional cardiovascular action (“third generation”). These last drugs have additional cardiovascular properties (especially vasodilation) that seem unrelated to β blockage. Propranolol is α nonselective β adrenergic receptor antagonist with equal affinity for β1 and β2 adrenergic receptors, lacks intrinsic sympathomimetic activity, and does not block α receptors. Propranolol has membrane stabilizing activity, low lipid solubility, the extent of oral absorption is < 90>
Absorption distribution metabolism and excretion of propranolol
Propranolol is highly lipophilic and almost completely absorbed after oral administration. Much of the drug is metabolized by the liver during its first passage through the portal circulation and only about 25% reaches the systemic circulation. In addition, there is great interindividual variation in the presystemic clearance of propranolol by the liver; this contributes to enormous variability in plasma concentrations (about 20-fold) after oral administration of the drug and to the wide dosage range for clinical efficacy. The degree of hepatic extraction of propranolol declines as the dose increases. The bioavailability of propranolol may be increased by the concomitant ingestion of food during long-term administration of the drug. Propranolol readily enters the central nervous system. Approximately 90% of the drug in the circulation is bound to plasma proteins. It is extensively metabolized, with most metabolites appearing in the urine. One product of hepatic metabolism is 4-hydroxypropanolol which has some β adrenergic antagonist activity. Analysis of the distribution of propranolol, its clearance by the liver, and its activity is complicated by the stereospecificity of these processes. The (-) enantiomer of propranolol is the active form and it is cleared more slowly from the body than the inactive enantiomer. The clearance of propranolol may vary with the hepatic blood flow and liver disease and also may change during the administration of other drugs that affect the hepatic metabolism. For the treatment of hypertension and angina, the initial oral dose of propranolol generally is 40 to 80 mg daily in adults. For the treatment of angina, the dose may be increased at intervals of less than 1 week as indicated clinically. In hypertension, the full blood pressure response may not develop for several weeks. Propranolol may be administered intravenously for the management of life-threatening arrhythmias or to patients under anaesthesia. Under these circumstances, the usual dose is 1 to 3 mg, administered slowly with careful and frequent monitoring of blood pressure, electrocardiogram, and cardiac function. If bradycardia is excessive, atropine should be administered to increase heart rate. A change to oral therapy should be initiated as soon as possible [1].
Literature search
The literature search was performed electronically using PubMed database as search engine and the following key words were used: “propranolol dosing infants, children“, propranolol efficacy, safety infants, children”, “propranolol effects infants, children”, Propranolol adverse effects infants, children”, “propranolol metabolism”, “propranolol pharmacokinetics infants, children”, “propranolol drug interactions”, “propranolol prophylaxis infants, children”, “propranolol treatment infants, children”, “propranolol trials infants, children”, “propranolol placental transfer”, and “propranolol migration into the breast-milk”. In addition, the books: The Pharmacological Basis of Therapeutics [1], Neonatal Formulary [2], NEOFAX® by Young and Mangum [3], and The British National Formulary for Children [4] were consulted.
Administration schedules of propranolol hydrochloride to infants and children
Administration of propranolol hydrochloride to infants [2].
Oral treatment of neonatal thyrotoxicosis
Infants. Give: 250 to 750 µg/kg of propranolol hydrochloride thrice-daily to control symptoms with 1 drop of Lugol iodine® trice-daily to control the transient neonatal thyrotoxicosis.
Lugol iodine® is a British formulation.
Intravenous treatment of arrhythmia
Infants. Try 20 µg/kg by slow intravenous injection over 10 min with electrocardiogram monitoring and increase this dose in step to cumulative total of 100 µg/kg if necessary. Give the effective dose intravenous thrice-daily for maintenance. The same strategy may also work for the “spells” sometimes seen in severe Fallot tetralogy (with oxygen, morphine, and, if necessary, sodium bicarbonate, to correct serious acidosis). For sustained oral maintenance try 250 to 500 µg/kg thrice-daily, adjust the dose according to response to a maximum of 4 mg/kg daily.
Oral treatment of neonatal hypertension
Infants. Start with 250 µg/kg thrice-daily together with hydralazine and increase the dose if necessary to a maximum of 2 mg/kg per dose.
Oral treatment of infantile haemangioma
Infants. The target dose for treatment is 1 to 3 mg/kg daily in 3 divided doses. Begin with the lowest possible dose and titrate upwards according to the response; many haemangioma will respond to even small doses. This is the best done under supervision especially in younger infants.
Propranolol is used for the treatment of tachycardia and hypertension. The preferred therapy for supraventricular tachycardia when is associated with Wolff-Parkinson-White syndrome. Other uses are the palliation of tetralogy of Fallot and hypertrophic obstructive cardiomyopathy, and adjunctive treatment of neonatal thyrotoxicosis. Propranolol is incompatible with most cephalosporins and penicillins [3].
Administration of propranolol hydrochloride to children
Oral administration for hyperthyroidism with autonomic symptoms
Children. Give initially 200 to 500 µg/kg thrice-daily, adjust the dose according to the response; increase the dose if necessary up to 1 mg/kg thrice-daily (maximum dose = 40 mg thrice-daily).
Intravenous administration for hyperthyroidism with autonomic symptoms
Children. Give initially 20 to 50 µg/kg thrice-daily or 4 times-daily (maximum per dose = 5 mg), adjust the dose according to the response, to be given over 10 min.
Oral treatment of thyrotoxicosis
Children. Give initially 250 to 500 µg/kg thrice-daily, adjust the dose according to the response; increase the dose if necessary up to 1 mg/kg thrice-daily (maximum dose = 40 mg thrice-daily).
Intravenous treatment of thyrotoxicosis
Children. Give initially 25 to 50 µg/kg thrice-daily or 4 times-daily (maximum per dose = 5 mg), adjust the dose according to the response, to be given over 10 min.
Oral treatment of thyrotoxic crisis
Children. Give initially 250 to 500 µg/kg thrice-daily or 4 times-daily, adjust the dose according to the response.
Intravenous treatment of thyrotoxic crisis
Children. Give initially 20 to 50 µg/kg thrice-daily or 4 times-daily (maximum per dose = 5 mg), adjust the dose according to the response, to be given over 10 min.
Oral treatment of hypertension
Children aged 1 month to 11 years. Give initially 0.25 to 1 mg/kg thrice-daily, and then increase the dose to 5 mg/kg in divided doses, the dose should be increased at weekly intervals.
Children aged 12 to 17 years. Give initially 80 mg twice-daily, and then increase the dose if necessary up to 160 to 320 mg daily, the dose should be increased at weekly intervals, slow-release preparations may be used for once-daily administration.
Oral prophylaxis of migraine
Children aged 2 to 11 years. Give initially 200 to 500 µg/kg twice-daily; usual dose is 10 to 20 mg twice-daily (maximum per dose = 2 mg/kg twice-daily).
Children aged 12 to 17 years. Give initially 20 to 40 mg twice-daily; usual dose is 40 to 80 mg twice-daily (maximum per dose = 120 mg, maximum dose = 4 mg/kg daily).
Oral treatment of arrhythmias
Children. Give: 250 to 500 µg/kg trice-daily or 4 times-daily (maximum dose = 1 mg/kg 4 times-daily), adjust the dose according to the response (maximum dose = 160 mg daily).
Intravenous treatment of arrhythmias
Children. Give: 25 to 50 µg/kg, and then 25 to 50 µg/kg thrice-daily or 4 times-daily if required, and the electrocardiogram monitoring is required.
Oral treatment of tetralogy of Fallot
Children aged 1 month to 11 years. Give 0.25 to 1 mg/kg thrice-daily or 4 times-daily (maximum dose = 5 mg/kg daily).
Intravenous treatment of tetralogy of Fallot
Children aged 1 month to 11 years. Give initially 15 to 20 µg/kg (maximum per dose = 100 µg/kg), higher doses are rarely necessary; and then 15 to 20 µg/kg thrice-daily or 4 times-daily if required, the electrocardiogram monitoring is required with the administration.
Efficacy and safety of propranolol in infants and children
Propranolol administered at a dose of 3.6 mg/kg daily is safe and successfully treats infants with supraventricular arrhythmias [5]. Propranolol is well tolerated with minimal adverse-effects in children with portal hypertension [6]. Propranolol is efficacy and safe in infants younger than 5 weeks and older than 5 months with infantile haemangioma [7]. Oral propranolol given at a dose of 2 mg/kg daily is a safe and effective treatment for infantile haemangiomas [8]. Oral propranolol administered at a dose of 2 mg/kg daily is well-tolerated and is an effective treatment for infantile haemangiomas [9]. Oral propranolol given at a dose of 3 mg/kg daily shows a consistent, rapid, and therapeutic effect of superficial infantile haemangiomas without significant adverse-effects [10]. Propranolol administered topically in 1% ointment has a beneficial effect on superficial haemangiomas of the skin and the treatment is well tolerated without adverse-effects [11]. Topical propranolol is safer than oral propranolol though may be less effective. Topical propranolol may be more suitable for infants with small superficial haemangiomas [12].
Effects of propranolol in infants and children
Oral propranolol inhibits angiogenesis via down-regulating the expression of vascular endothelial growth factor in infantile haemangioma derived stem cell [13]. Early effects of propranolol are attributable to vasoconstriction due to decreased release of nitric oxide and long-term effects are characterized by induction of apoptosis in proliferating endothelial cells which results in tumour regression [14]. Oral propranolol is highly effective and safe in the treatment of periocular capillary haemangiomas in infants [15]. Propranolol treatment improves heart failure scores, shorts lengths of hospital stay, lowers plasma renin activities, and corrects the diastolic ventricular function [16]. Propranolol eliminates symptoms attributed to idiopathic hypertrophic subaortic stenosis in all children and abolished hypoxemic spells in 12 of 17 (70.6%) children. Oral propranolol is an excellent drug for use in paediatric patients with different types of cardiac disease [17]. Propranolol is able to cross the blood-brain-barrier and induces the formation-rate of nitric oxide and/or H2O2 in the hypothalamus [18].
Adverse-effects caused by propranolol in infants and children
When used on very preterm infants, propranolol hydrochloride may have some temporary effects on the vital functions of these infants; however no serious adverse-effects are detected that may affect the physical and mental development in the long run [19]. Intolerable adverse-effects are rare in infants with haemangioma who are treated with propranolol. Predictive factors for intolerable adverse-effects include younger age and lower body-weight [20]. Six of 35 infants (17.1%) who were treated with oral propranolol underwent retinopathy of prematurity intervention, as opposed to 14 of 36 (38.9%) control infants [21]. An 18 month old boy presented caries in the upper central incisors following the use of propranolol solution for the treatment of an infantile haemangioma [22].
Metabolism of propranolol in human liver microsomes
Propranolol is converted into 4-hydroxy-, 5-hydroxy-propranolol, and N-desisopropranol whereas 7-hydroxypropranolol appears in trace amounts [23]. The formation of propranolol 5-hydroxylation as well as 4-hydroxylation is mainly catalysed by CYP2D6 and the formation of N-desisopropranol is catalysed by CYP1A2 in human liver microsomes [23].


P-value for correlation *P-value < 0>
This table shows that the side-chain N-desisopropylation of both propranolol enantiomers is mediated mainly by the CYP1A subfamily and to some extent by CYP2D6, whereas the ring 4-hydroxilation of the enantiomers is mediated almost exclusively by CYP2D6. The contribution of S-mephenytoin 4’-hydroxylase (CYP2C19) to the N-desisopropylation of propranolol enantiomers appears to be of negligible importance in human liver microsomes.
The glucuronidation of R- and S-propranolol is catalysed by at least 3 UGT isoforms: UGT1A9, UGT2B4 and UGT2B7. UGT1A9 shows remarkable stereoselectivity in Vmax and CLint values of R-propranolol < S>

Metabolism of propranolol in human subjects
The oral clearance of propranolol is significantly higher in men (65.7+7.7 ml/min/kg) than in women (40.2+6.2 ml/min/kg), P-value < 0>
Pharmacokinetics of propranolol in term and preterm infants
Filippi et al. [28] studied the pharmacokinetics of propranolol in 36 term and preterm infants who were suffering from congenital heart disease (N = 1), hypertrophic obstructive cardiomyopathy (N = 2), supraventricular tachycardia (N = 3), neonatal thyrotoxicosis (N = 4), Fallot tetralogy (N = 5), infantile haemangioma (N = 15), and to control hypotension (N = 6). The infants had postmenstrual and postnatal ages of 27.8+4.0 weeks and 66.5+20.1 days, respectively, and weighed 1,014+710 grams. Propranolol was administered orally at a dose of 0.5 mg/kg 4 times-daily to 28 infants and at a dose of 0.25 mg/kg 4 times-daily to 8 infants with extremely low postmenstrual age.
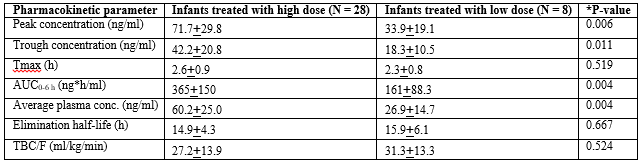
Tmax = time to reach the peak concentration. TBC/F = apparent total body oral clearance. F = oral bioavailability. *Student t test for umpired data.
This table shows that all pharmacokinetics parameters of propranolol, except for the Tmax, the elimination half-life, and the apparent total body clearance are different according to the two doses.

Tmax = time to reach the peak concentration. TBC/F = apparent total body oral clearance. F = oral bioavailability.
This table shows that the pharmacokinetic parameters of propranolol are not different in the three groups of infants. The difference among groups was tested by Analysis of variance (ANOVA).
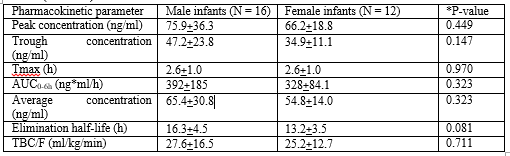
Tmax = time to reach the peak concentration. TBC/F = apparent total body oral clearance. F = oral bioavailability. *Student t test for umpired data.
This table shows that the pharmacokinetic parameters of propranolol are not different according to the sex.
Takechi et al. [29] investigated the pharmacokinetics of propranolol in 32 infants and young children (9 males and 23 females) suffering from infantile haemangioma. Subjects had mean postmenstrual, postnatal ages, and body-weight of 374 days (range, 317 to 437), 113 days (range, 53 to 150), and 6,115 grams (range, 3,150 to 8,710), respectively. Propranolol was administered orally at an initial dose of 0.5 mg/kg twice-daily and then the dose was increased to 3 mg/kg daily and the treatment lasted for 24 weeks.
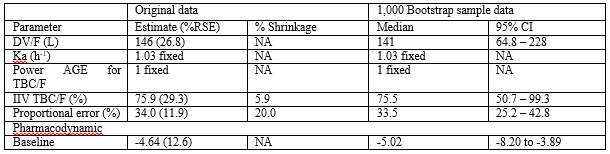
DV = apparent distribution volume. Ka = absorption rate constant. TBC = apparent total body clearance. F = oral bioavailability. Power AGE for TBC/F = power exponent of age for TBC/F. %RSE = %relative standard error. Baseline indicates the intercept coefficient of logistic regression. NA = not applicable.
This table shows that the distribution volume is larger than the water volume, propranolol is rapidly absorbed following oral administration, and there is a remarkable interindividual variability of the total body clearance. This variability is accounted by a wide variability in the demographic characteristics of subjects enrolled in the study.
Interaction of propranolol with drugs
Blood concentration of lithium is increased when it is co-administered with propranolol [30]. There is a correlation between in-vitro drug dissolution and in-vivo plasma concentration of propranolol when it is co-administered with paracetamol [31]. The absorption, protein binding, and metabolism of propranolol is affected by the co-administration of other drugs. Halofenate, phenytoin, phenobarbitone, rifampicin and ethanol affect the clearance of propranolol and chlorpromazine and cimetidine inhibit the metabolism of propranolol [32]. Although the propranolol and nifedipine alone are significantly more effective than placebo, their combination provides an even greater improvement (P-value < 0>
Prophylaxis with propranolol in infants and children
Prophylactic oral propranolol is effective in preventing severe retinopathy of prematurity in premature infants [36]. Prophylaxis with propranolol is efficacy in controlling the progression of retinopathy of prematurity in preterm infants [37]. Prophylactic propranolol, in the prescribed dose of 1 mg/kg daily, shows a decreasing trend in all outcomes of retinopathy of prematurity [38]. The use of propranolol prevents the occurrence of cyanotic spells in preoperative infants with the tetralogy of Fallot [39]. Propranolol is useful for preventing the first and recurrent variceal bleeding in cirrhotic children [40]. Topiramate and propranolol have the same efficiency in preventing migraine headaches [41]. Prophylaxis with propranolol reduces monthly headache frequency up to 3.73+6.11 and 3.34+5.95 after 4 and 8 weeks, respectively [42].
Treatment with propranolol in infants and children
Propranolol reduces the recurrence of supraventricular tachycardia in 70% of infants [43]. There is no difference in supraventricular tachycardia recurrence in infants treated with digoxin or propranolol [44]. Propranolol treatment, but not digoxin and diuretics alone, effectively reduce clinical symptoms of heart failure in infants with congenital heart disease [45]. Propranolol is effective in treating hypoxemic spells in 80% of infants with teratology of Fallot and the effectiveness is greater with large doses of propranolol [46]. Propranolol treatment is safety and efficacy in infantile haemangioma and a higher response-rate can be gained with early treatment and a prolonged course of therapy [47]. Propranolol is a useful and safe treatment option for severe or complicated infantile haemangioma achieves a rapid and significant reduction in haemangioma size, and no adverse-effects are observed [48]. Propranolol administered at doses of 1.5 or 2 mg/kg daily, given in divided doses, with stepwise escalation is safe and effective for treating proliferating infantile haemangioma [49]. Propranolol administered orally at doses of 2 to 3 mg/kg daily has a consistent, rapid, and therapeutic effect, leading to considerable shortening of the natural course of infantile haemangiomas with good clinical tolerance [50].
Trials with propranolol in infants and children
Preterm newborns with retinopathy of prematurity, especially in stage 2 retinopathy of prematurity, were given oral propranolol and have a reduced risk of disease progression [51]. Oral propranolol in early stages of retinopathy of prematurity prevents the disease progression and reduces the need for invasive rescue therapy with laser or bevacizumab [52]. A trial showed that propranolol is effective at a dose of 3 mg/kg daily for 6 months in the treatment of infantile haemangioma [53]. Propranolol administered orally at a dose of 2 mg/kg daily reduces the volume, colour, and elevation of focal and segmental infantile haemangioma in infants and children [54]. Propranolol is efficacious in patients with infantile haemangioma. The most pronounced response is seen in the first 8 weeks and in infants aged 6 months or younger. A decline in heart-rate > 20% is an early marker of response to propranolol [55].
Transfer of propranolol across the human placenta
With recirculation of the fetal and maternal compartments propranolol rapidly equilibrated in the two perfusion circuits at 35% of the initial level in the maternal circuit [56]. The ratios of cord plasma to simultaneous maternal plasma levels of propranolol and its major metabolites are: propranolol 0.32+0.17, propranolol glucuronide 0.86+0.36, 4-hydroxypropranolol 1.4+1.0, 4-hydroxypropranolol β-D-glucuronide 0.71+0.45, and naphthoxylactic acid 3.0+1.6 [57]. The maternal concentration of propranolol is approximately four times that of the umbilical circulation [58].
Migration of propranolol into the breast-milk
In a woman taking 10 mg thrice-daily of propranolol, the peak of propranolol in the breast-milk is 30 µg/L at 2 hours after the dose [59]. Five postpartum women taking 40 mg twice-daily have average breast-milk concentration of propranolol 30 µg/L at 2 hours after the dose [60]. The concentration of propranolol in the breast-milk is 110 to 120 µg/L in two women 3 hours after an oral dose of 160 mg [61]. A hypertensive woman was treated throughout pregnancy with propranolol 40 mg daily, the breast-milk to plasma ratio is < 1>
Propranolol is α nonselective β adrenergic receptor antagonist with equal affinity for β1 and β2 adrenergic receptors, lacks sympathomimetic activity, and does not block α receptors. Propranolol may be administered orally or intravenously, the oral absorption-rate is < 90>
In conclusion, propranolol is α nonselective β adrenergic receptor antagonist with equal affinity for β1 and β2 adrenergic receptors, lacks intrinsic sympathomimetic activity, and does not block α receptors. Propranolol may be administered orally or intravenously, the extent of oral absorption is < 90>
The authors declare no conflicts of financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employments, gifts, and honoraria.
This article is a review and drugs have not been administered to men or animals.
The author thanks Dr. Patrizia Ciucci and Dr. Francesco Varricchio, of the Medical Library of the University of Pisa, for retrieving the scientific literature.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
