
Research Article | DOI: https://doi.org/10.31579/2690-8794/116
*Corresponding Author: Gian Maria Pacifici,, Associate Professor of Pharmacology, via Sant’Andrea 32, 56127 Pisa, Italy.
Citation: Gian M. Pacifici, (2022) Clinical Pharmacology of Phenobarbital in Infants and Children, Clinical Medical Reviews and Reports. 4(3); DOI: 10.31579/2690-8794/116
Copyright: © 2022, Gian Maria Pacifici, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 November 2021 | Accepted: 16 December 2021 | Published: 07 January 2022
Keywords: phenobarbital; metabolism; pharmacokinetics treatment; trials; human brain; human placenta; breast-milk; infants, children
Phenobarbital inhibits seizures by potentiation of synaptic inhibition through an action on the GABAA receptor. Phenobarbital is an effective agent for generalized tonic-clonic focal-to-bilateral tonic-clonic and focal seizures. Phenobarbital may be administered orally or intravenously and following oral dosing phenobarbital is completely absorbed. In infants, seizures are controlled by an intravenous loading dose of 20 mg/kg followed by a maintenance dose of 4 mg/kg once-daily. In children, the treatment of all forms of epilepsy, except for typical absence seizures, consists in an oral phenobarbital and the status epilepticus is treated with intravenous phenobarbital and treatments consist in a loading dose followed by a maintenance dose. Phenobarbital induces several CYPs, UGT1A1, and CYP2B and CYP3A genes. In newborns and children, the elimination half-life is 46.9 hours and the distribution volume is 0.49 L/kg. In children with severe falciparum malaria and convulsions, the distribution volume is 0.79 L/kg. The treatment and trials with phenobarbital have been studied and phenobarbital interacts with drugs. Phenobarbital is transported into the human brain where reaches therapeutic concentrations and phenobarbital freely crosses the human placenta. Following therapeutic treatment with phenobarbital to lactating women, the concentrations of phenobarbital in the breast-milk are few µg/ml suggesting that phenobarbital poorly migrates into the breast-milk. The aim of this study is to review the published data of phenobarbital dosing, pharmacokinetics, treatment, and trials in infants and children, and the phenobarbital metabolism, phenobarbital transport in the human brain, placental transfer of phenobarbital, and phenobarbital migration into the breast-milk.
Phenobarbital was the first effective organic antiseizure agent. It has relatively low toxicity, is inexpensive, and is still one of the more effective and widely used antiseizure drugs [1].
The mechanism by which phenobarbital inhibits seizures likely involve potentiation of synaptic inhibition through an action on the GABAA receptor. Phenobarbital enhances responses to iontophoretically applied GABA in mouse cortical and spinal neurons, effects that are observed at therapeutically relevant concentrations of phenobarbital; in patch-clamp studies, phenobarbital increases the GABAA receptor-mediated current by increasing the duration of bursts of GABAA receptor-mediated currents without changing the frequency of bursts. At levels exceeding therapeutic concentrations, phenobarbital also limits its sustained repetitive firing; this may underline some of the antiseizure effects of higher concentrations of phenobarbital achieved during therapy of status epilepticus [1].
Phenobarbital is an effective agent for generalized tonic-clonic focal-to-bilateral tonic-clonic, tonic-clonic of unknown onset (generalized tonic-clonic), and focal seizures. Its efficacy, low toxicity, and low cost make it an important agent for these types of epilepsy. However, its sedative effect and its tendency to disturb behaviour in children have reduced its use as a primary agent. It is not effective for absence seizures [1]. Phenobarbital remains, over 100 years since it was the first introduced into clinical practice, perhaps the most widely used anticonvulsant in neonatology and it is still, for many, the first-line treatment for seizures in cooled and non-cooled infants [2]. Phenobarbital may improve outcomes in severely asphyxiated infants. Phenobarbital is administered by an intravenous infusion at a dose of 40 mg/kg over 1 hour, prior to onset of seizures. Phenobarbital may enhance the bile excretion in infants with cholestasis before technetium 99m-image display and analysis scanning. Phenobarbital is incompatible with: fat emulsion, hydralazine, hydrocortisone succinate, insulin, methadone, pancuronium, ranitidine, and vancomycin [3].
Oral absorption of phenobarbital is complete but somewhat slow; peak concentrations in plasm occur several hours after a single dose. It is 40 to 60% bound to plasma proteins and bound to a similar extent in the tissues, including brain. Up to 25% of a dose is eliminated by pH-dependent renal excretion of the unchanged drug; the remainder is inactivated by hepatic microsomal enzymes, principally CYP2C9, with minor metabolism by CYP2C19 and CYP2E1. Phenobarbital induces UGT enzymes as well as the CYP2C19 and CYP2E1 subfamilies. Drug metabolized by these enzymes can be more rapidly degraded when co-administered with phenobarbital; importantly. Oral contraceptives are metabolized by CYP3A4. The elimination half-life of phenobarbital varies widely, 50 to 140hours in adults and 40 to 70 hours in children younger than 5 years of age, often longer in infants. Phenobarbital’s duration of effect usually exceeds 6 to 12 hours in nontolerant patients [1].
During long-term therapy in adults, the plasma concentrations of phenobarbital averages 10 µg/ml per daily dose of 1 mg/kg; in children, the value is 5 to 7 µg/ml per 1 mg/kg. Although a precise relationship between therapeutic results and concentration of drug in plasma does not exist, plasma concentrations of 15 to 35 µg/ml are usually recommended for control of seizures. The relationship between plasma concentration of phenobarbital and adverse-effects varies in the development of tolerance. Sedation, nystagmus, and ataxia usually are absent at concentrations below 30 µg/ml during long-term therapy, but adverse-effects may be apparent for several days at lower concentrations when therapy is initiated or whenever the dosage is increased. Concentrations more than 60 µg/ml may be associated with marked intoxication in the nontolerant individual. Because significant behavioural toxicity may be present despite the absence of overt signs of toxicity, the tendency to maintain patients, particularly children, on excessively high doses of phenobarbital should be resisted. The plasma phenobarbital concentrations should be increased above 30 to 40 µg/ml only if the increment is adequately tolerated and only if contributes significantly to control of seizures [1].
The literature search was performed electronically using PubMed database as search engine and the following key words were used: “phenobarbital dosing infants, children“, “phenobarbital metabolism”, “phenobarbital pharmacokinetics infants, children”, “phenobarbital treatment infants, children”, “phenobarbital trials infants, children”, “phenobarbital drug interactions”, “phenobarbital human brain”, “phenobarbital placental transfer”, and “phenobarbital breast-milk”. In addition, the books: The Pharmacological Basis of Therapeutics [1], Neonatal Formulary [2], NEOFAX® by Young and Mangum [3], and The British National Formulary for Children [4] have been consulted.
Administration schedules of phenobarbital to infants and children
Administration to infants [2]
Give 20 mg/kg as a slow intravenous loading dose over 20 min to control seizures (once any biochemical disturbance, such has hypoglycaemia, has been excluded or treated) followed by 4 mg/kg once-daily by intravenous or intramuscular injection or by mouth (when a higher dose may be needed). Increase this to 5 mg/kg once-daily if treatment is needed for more than 2 weeks. While higher loading dose have been used, these can cause respiratory depression in the preterm infant and can cause prolonged sedation in infants undergoing therapeutic hypothermia.
Administration to children [4]
Oral treatment of all forms of epilepsy except typical absence seizures
Children aged 1 month to 11 years. Give initially 1 to 1.5 mg/kg twice-daily, and ten increase the dose in steps of 2 mg/kg daily as required; the maintenance dose is 2.5 to 4 mg/kg once-daily or twice-daily.
Children aged 12 to 17 years. Give: 60 to 180 mg once-daily.
Slow intravenous injection for the treatment of the status epilepticus
Children aged 1 month to 11 years. Give initially 20 mg/kg, the dose should be administered at a rate no faster than 1 mg/min, and then give 2.5 to 5 mg/kg once-daily or twice-daily.
Children aged 12 to 17 years. Give initially 20 mg/kg (maximum dose = 1 gram), the dose should be administered at a rate no faster than 1 mg/min, and then 300 mg twice-daily.
Induction of CYPs and UGTs by phenobarbital
A distal gene fragment, of about 2000 kb in CYP2B1, CYP2B2, and CYP2B10, has been shown to be a phenobarbital-responsive enhancer independent of proximal promoter elements. This fragment contains several binding sites for proteins and several functional elements, including an NF-1 site, and, therefore, has been designated as a phenobarbital-responsive unit [5]. Patients co-medicated with phenobarbital had significantly lower plasma clozapine levels than those of the controls (232+104 versus 356+138 ng/ml, P-value < 0>
Pharmacokinetics of phenobarbital in newborns and infants maintained on extracorporeal membrane oxygenation with phenobarbital
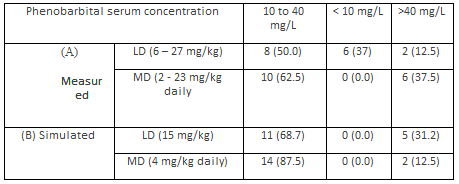
Pokorná et al. [13] studied the pharmacokinetics of phenobarbital in 7 newborns and 9 infants. Table 1 summarizes the demographic characteristics of subjects included in the study, table 2 shows the administration schedules of phenobarbital, and table 3 provides the pharmacokinetic parameters of phenobarbital.
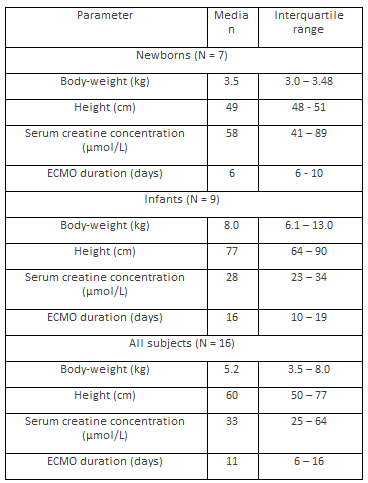
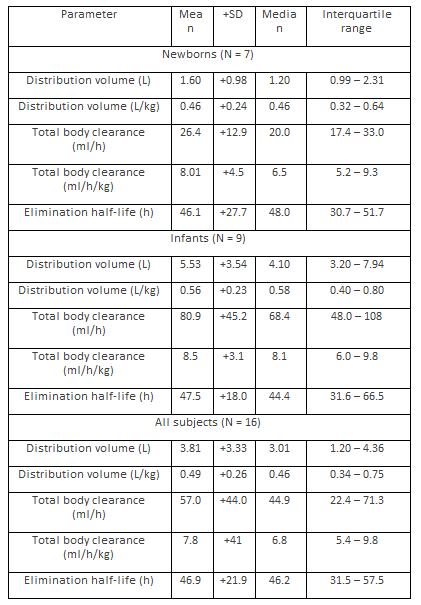
This table shows that the pharmacokinetic parameters obtained in newborns are not significantly different from those obtained in infants probably because the wide variability of the pharmacokinetic parameters.
Shellhaas et al. [14] investigated the pharmacokinetics of phenobarbital in 39 infants with neonatal encephalopathy. Twenty infants had hypothermia and 19 infants were normthermic. Table 4 summarizes the demographic characteristics of infants included in the study and table 5 shows the pharmacokinetics of phenobarbital obtained in these infants. Phenobarbital was administered as a loading dose followed by a maintenance dose. After loading phenobarbital doses of up 35 mg/kg, seven infants were treated with 2.5 mg/kg maintenance dosing twice-daily, while the remaining infants received 1.5 mg/kg maintenance dosing twice-daily.
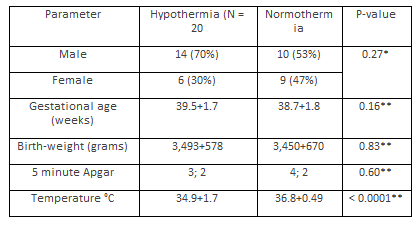
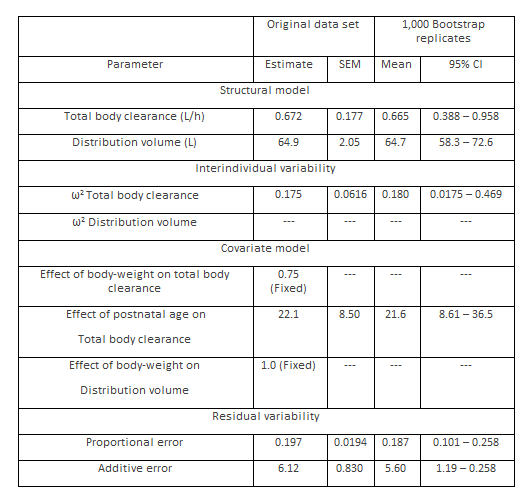
This table shows that the distribution volume is larger than the water volume and there is a remarkable interindividual variability of the total body clearance and the distribution volume. The comparison of the total body clearance and the distribution volume, obtained in these infants, with those obtained in infants maintained on extracorporeal membrane oxygenation (see table 3) is difficult because of the different diseases in these infants and the different expression units of pharmacokinetic parameters.
Pharmacokinetics of phenobarbital in children with severe falciparum malaria and convulsions
Kokwaro et al. [15] studied the pharmacokinetics of phenobarbital in 12 children, aged 7 to 62 months, with severe falciparum malaria and convulsions. Phenobarbital was administered as a loading dose followed by a maintenance dose. The intravenous loading dose was 15 mg/kg followed by a maintenance dose of 5 mg/kg 24 and 48 hours later.
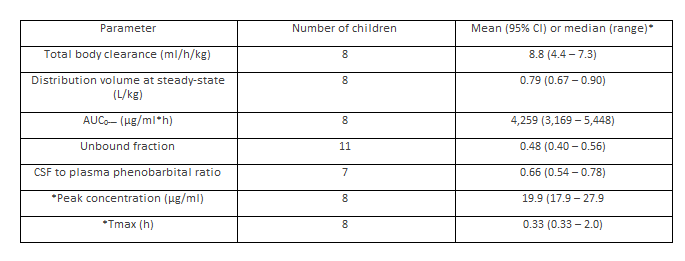
This tale shows that the distribution volume is similar to the water volume, phenobarbital is transported into the cerebrospinal fluid in significant amounts, and there is a remarkable interindividual variability in the pharmacokinetic parameter. The comparison of total body clearance and distribution volume with those obtained in infants (for infants see tables 3 and 5) is difficult because of the different diseases in infants and children and the different units of expression the pharmacokinetic parameters.
Treatment of infants and children with phenobarbital
Among infants with neonatal opioid withdrawal syndrome receiving morphine and secondary therapy, those treated with phenobarbital, had shorter length of hospital stay and shorter morphine treatment duration [16]. Intravenous administered phenobarbital controls seizures in 77% of both term and preterm newborns [17]. The mortality-rate caused by intracerebral haemorrhage in infants is significantly lower in the phenobarbital-treated group (8.0%) than in the control group (84.8%, P-value < 0>
Trials with phenobarbital conducted in infants and children
Phenobarbital is more effective than levetiracetam for the treatment of neonatal seizures [25]. Levetiracetam achieves better control than phenobarbitone for neonatal seizures when used as first-line antiepileptic drug and is not associated with adverse drug reactions [26]. Phenobarbital is associated with more adverse-effects than levetiracetam and the two drugs were equally but incompletely effective in treating electrographically confirmed seizures in neonates following cardiac surgery [27]. The significant difference (P-value < 0>
Interaction of phenobarbital with drugs
Phenobarbital has a great impact on the pharmacokinetics of tacrolimus over time in paediatric and adult patients. Phenobarbital can reduce the pharmacokinetic parameters of tacrolimus more effectively than intravenous phenobarbital [29]. After discontinuation of phenobarbital effective tacrolimus trough levels are increased [30]. Phenobarbital leads to a remarkable reduction in the plasma concentration of dolutegravir in a dose-dependent manner [31]. Phenobarbital co-administration with midazolam significantly increased midazolam clearance [32]. Tipranavir-ritonavir is a substrate of CYP3A4 and phenobarbital is an inductor of this CYP and phenobarbital decreases the plasma concentration of tipranavir-ritonavir [33]. Phenobarbital reduces the plasma concentration of chloramphenicol [34]. Phenobarbital lowers the plasma concentration of warfarin and reduces the half-life of warfarin [35]. Phenobarbital decreases the plasma concentration of warfarin antagonising the anticoagulant effect of warfarin [36].
Transport of phenobarbital into the human brain
In 10 patients, a significant correlation is found between brain and plasma of phenobarbital concentrations and the mean brain to plasma phenobarbital ratio is 0.91+0.08 [37]. In 12 epileptic patients undergoing temporal lobectomy, a significant correlation (P-value < 0>
Transfer of phenobarbital across the human placenta
The placental transfer of phenobarbital was investigated in 35 mother-infant pairs at birth. The drug was administered prenatally to the mothers for maternal epilepsy (group A, N = 5), gestational hypertension and preeclampsia (group B, N = 20) and prophylaxis of intraventricular haemorrhage in premature deliveries (group C, N = 10). The phenobarbital levels in arterial cord blood were 100+2.8% in group A, 89+21% in group B and 77+16% in group C with respect to the levels observed in the mothers. The most important factor influencing the transplacental passage was the duration of maternal treatment in the infant of group A (r = 0.80, P-value < 0 xss=removed xss=removed>
Migration of phenobarbital into the breast-milk
In lactating women taking phenobarbital for 3 days, the average breast-milk concentrations at 23 hours after the last dose are as follows: 90 mg daily in 4 women, 0.85 µg/ml (range, 0.8 to 1.0); 150 mg daily in 2 women, 1.25 µg/ml (range, 1.0 to 1.5); 225 mg daily in 2 women, 5.2 µg/ml (range, 2.7 to 5.0). The breast-milk phenobarbital concentrations are fairly constant during the day, averaging from 5.6 to 6.0 µg/ml at 9 am, 10 am and 8 pm in one lactating woman between days 3 and 7 postpartum. In the others, the phenobarbital concentrations averages to 7.3, 7.8, and 8.8 µg/ml at 6 am, 10 am and 8 pm, respectively, between days 5 and 11 postpartum [45]. A breast-milk phenobarbital concentration of 2.7 µg/ml is found 16 hours after the last dose in a lactating mother taking 30 mg of phenobarbital 4 times-daily from 3.5 to 6 days postpartum [46]. Eight phenobarbital breast-milk concentrations were measured between the days 3 and 32 postpartum at unstated times after the dose in an unstated number of nursing women who were taking phenobarbital and other anticonvulsants in unstated dosages. Phenobarbital breast-milk concentration averages to 10.4 µg/ml (range, 0.5 to 33), while the maternal serum concentration averages to 19.3 µg/ml [47]. Breast-milk samples were obtained during the first week postpartum from 4 lactating women who were taking phenobarbital. Their phenobarbital dosages ranged from 30 to 150 mg daily in 3 divided doses and the breast-milk samples were obtained 2 to 3 hours after the dose. Breast-milk concentration of phenobarbital ranged from 4.5 µg/ml in a woman taking 30 mg daily of phenobarbital to 7.6 µg/ml in a woman taking 150 mg daily. Phenobarbital concentration in breast-milk is less than that in simultaneous maternal serum samples in all cases [48].
Phenobarbital inhibits seizures by potentiation of synaptic inhibition through an action on GABAA. In patch-clamp studies, phenobarbital increase the GABAA receptor-mediated current by increasing the duration of burst of GABAA. Phenobarbital treats generalized tonic-clonic focal-to-bilateral tonic-clonic and focal seizures. Phenobarbital may be administered orally or intravenously, the oral absorption is complete, and peak plasma concentration occurs several hours after an oral dose [1]. In infants, the seizures are controlled with phenobarbital intravenous loading dose of 20 mg/kg followed by a maintenance dose of 4 mg/kg once-daily [2]. In children, all forms of epilepsy, except for typical absence seizures, are treated with oral phenobarbital and the status epilepticus is treated with intravenous phenobarbital, treatments consist in a loading dose followed by a maintenance dose, and phenobarbital dose increases with child age [4]. Phenobarbital induces several forms of CYPs and UGT1A and CYP2B and CYP3A genes [5-12]. Phenobarbital induces CYP2B1, CYP2B2, and CYP2B2 [5], phenobarbital induces the metabolism of clozapine increasing the formation-rate of N-oxide clozapine and demethylation pathway [6], and phenobarbital induces CYP2B and CYP3A genes [7]. In human liver slices, phenobarbital induces CYP2B6 and CYP3A4 mRNA and apoprotein [8]. In co-cultured HepG2, phenobarbital induces the expression of CYP2C and CYP3A family genes [9], and phenobarbital induces UGT1A1 [10-12]. The pharmacokinetics of phenobarbital have been studied in newborns and infant; the elimination half-life, the total body clearance, and the distribution volume of phenobarbital are about 47 hours, 57 ml/h, and about 0.5 L/kg, respectively [13]. In children with neonatal encephalopathy, the total body clearance and the distribution volume are 0.672 L/h and 64.9 L, respectively [14]. In children with severe falciparum malaria and convulsions, the total body clearance and the distribution volume are 8.8 ml/h/kg and 0.79 L/kg, respectively [15]. The comparison of the total body clearance and the distribution volume between infants and children is difficult because of the different diseases in infants and children and the different units of expression the pharmacokinetic parameters. The treatment of infants and children with phenobarbital has been extensively studied [16-24]. Phenobarbital treats the opioid withdrawal syndrome in newborns and this treatment provides a shorter hospitalization duration and shorter morphine treatment duration [16], intravenous phenobarbital controls seizures in the majority of newborns [17], and phenobarbital decreases the mortality-rate in preterm infants with intracerebral haemorrhage [18]. A phenobarbital loading dose of 15 mg/kg followed by a maintenance dose of 6 mg/kg once-daily controls convulsions in infants [19], an intravenous loading dose of phenobarbital of 15 to 20 mg/kg followed by a maintenance dose of 5 mg/kg once-daily controls seizures in infants [20], and phenobarbital decreases the incidence of neonatal hyperbilirubinemia [21]. Phenobarbital manages seizures in infants and children but phenobarbital my causes poisoning and phenobarbital should be administered with caution to avoid toxicity [22], phenobarbital controls the seizures in infants and children [23, 24]. The trials with phenobarbital have been conducted in infants and children [25-28]. Phenobarbital is more effective than levetiracetam for the control of neonatal seizures [25], in contrast with this finding, levetiracetam may control neonatal seizures more effectively than phenobarbital [26, 27], and phenobarbital is more effective than placebo in the control of febrile seizures in children [29]. The interaction of phenobarbital with drugs has been extensively reported [29-36]. Phenobarbital reduces the pharmacokinetic parameters of tacrolimus [29, 30], increases the midazolam clearance [30], reduces the plasma concentration of dolutegravir in a dose-dependent manner [31], phenobarbital increases the midazolam clearance [32], induces the CYP3A4 and this enzyme metabolizes tipranavir-ritonavir thus phenobarbital decreases the plasma concentration of tipranavir-ritonavir [33], phenobarbital reduces the plasma concentration of chloramphenicol [34], and lowers the plasma concentration of warfarin antagonising the anticoagulant effect of warfarin [35, 36]. The transport of phenobarbital into the human brain has been extensively studied [37-41]. The brain to plasma phenobarbital ratio is 0.91+0.08 [37], and it is 0.46+0.12 [38], a good correlation has been found between the plasma and brain [39, 40], phenobarbital is rapidly and uniformly transported into the brain [40], and the transport of phenobarbital into the newborn brain occurs rapidly and depends on brain lesion [41]. These results indicate that phenobarbital is transported into the human brain rapidly and the brain concentration of phenobarbital in brain equilibrates with that in plasma. Phenobarbital freely crosses the human placenta; the major factors influencing the transfer-rate of phenobarbital are the duration of maternal treatment, the gestational age, and the pH in the arterial umbilical cord [42], the umbilical cord to maternal concentration ratio of phenobarbital is 0.97+0.04 [43], and phenobarbital equilibrates between umbilical cord and maternal plasma [44]. These findings suggest that phenobarbital freely crosses the human placenta. The migration of phenobarbital into the breast-milk has been extensively studied [45-48]. Following therapeutic treatment with phenobarbital to lactating mothers, phenobarbital achieves concentrations of few µg/ml in the breast-milk indicating that phenobarbital poorly migrates into the breast-milk, and the concentrations of phenobarbital in the breast-milk are lower than the maternal ones [48].
In conclusion, phenobarbital is an effective gent for treatment of the generalized tonic-clonic focal-to-bilateral tonic-clonic and focal seizures. Phenobarbital may be administered orally of intravenously, and following oral dosing, phenobarbital is complete absorbed. The treatment of infants with seizures consists in an intravenous loading dose of 20 mg/kg followed by a maintenance dose of 4 mg/kg once-daily. The treatment of children with all forms of epilepsy, except for the typical absence seizures, consists in oral phenobarbital and the status epilepticus is treated with intravenous phenobarbital, and treatments consist in a loading dose followed by a maintenance dose, and phenobarbital dosage varies according to the child age. Phenobarbital induces different CYPs and UGT1A1 and CYP2B and CYP3A genes. The phenobarbital elimination half-life is about 47 hours in infants and no results are available for children. The treatment and trials with phenobarbital have been studied in infants and children. Phenobarbital interacts with drugs. The transport of phenobarbital into the human brain, the transfer of phenobarbital across the human placenta, and the migration of phenobarbital into the breast-milk have been extensively studied. The aim of this investigation is to review the clinical pharmacology of phenobarbital in infants and children.
The authors declare no conflicts of financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employments, gifts, and honoraria. This article is a review and drugs have not been administered to men or animals.
The author thanks Dr. Patrizia Ciucci and Dr. Francesco Varricchio, of the Medical Library of the University of Pisa, for retrieving the scientific literature.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
