
Research Article | DOI: https://doi.org/10.31579/2690-8816/049
Associate Professor of Pharmacology, via Sant’ Andrea 32, 56126 Pisa, Italy.
*Corresponding Author: Gian Maria Pacifici, Associate Professor of Pharmacology, via Sant’Andrea 32, 56126 Pisa, Italy
Citation: Gian Maria Pacifici. (2022). clinical pharmacology of dobutamine in infants and children. Clinical Research Notes. 3(2); DOI: 10.31579/2690-8816/049
Copyright: © 2022 Gian Maria Pacifici. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, providedthe original work is properly cited.
Received: 22 November 2021 | Accepted: 23 December 2021 | Published: 24 January 2022
Keywords: dobutamine; dosing; effects; metabolism; pharmacokinetics; treatment infants; children
Dobutamine resembles dopamine structurally but possess a bulky aromatic substituent on the amino group. The pharmacological effects of dobutamine are due to direct interaction with α and β receptors. Dobutamine possess a centre of asymmetry, the (-) isomer of dobutamine is a potent α1 agonist and can cause marked pressor response. In contrast, (+) dobutamine is a potent α1 receptor antagonist which can block the effect of (-) dobutamine. Both isomers are full agonist at β receptors; the (+) isomer is a more potent β agonist than the (-) isomer by about 10-fold. Dobutamine is indicated for the short-term treatment of cardiac decompensation that may occur after cardiac surgery and dobutamine is used in the treatment of hypotension especially if related to myocardial dysfunction. Dobutamine is administered by continuous intravenous infusion and the initial dose is 5 µg/kg per min in infants and children. Some authors stated that dopamine is more effective than dobutamine in increasing blood pressure whereas other authors observed that dobutamine and dopamine produce similar pressure response. Dobutamine is methylated and is also conjugated with glucuronic acid. The elimination half-life of dobutamine is 25.6 min in infants and children but it ranges in a wide interval. The treatment of infants and children with dobutamine has been extensively studied and some authors observed that dobutamine increase the blood pressure and decreases vascular resistance. The aim of this study is to review the dobutamine dosing, effects, metabolism, pharmacokinetics, and treatment.
Mechanism of Action of Dobutamine
Dobutamine resembles dopamine structurally but possess a bulky aromatic substituent on the amino group. The pharmacological effects of dobutamine are due to direct interactions with α and β receptors; its actions do not appear to result from release of norepinephrine from symptomatic nerve endings, and they are not exerted by dopaminergic receptors. Dobutamine possess a centre of asymmetry; both enantiomer forms are present in the racemate and are used clinically. The (-) isomer of dobutamine is a potent α1 agonist and can cause marked pressor response. In contrast, (+) dobutamine is a potent α1 receptor antagonist which can block the effects of (-) dobutamine. Both isomers are full agonists at β receptors; the (+) isomer is a more potent β agonist than the (-) isomer by about 10-fold [1].
Cardiovascular Effects of Dobutamine
The cardiovascular effects of racemic dobutamine represent a composite of the distinct pharmacological properties of the (-) and (+) stereoimeres. Compared to isoproterenol, dobutamine has relatively more prominent inotropic than chronotropic effects on the heart. Although not completely unabsorbed, this useful selectivity may arise because peripheral resistance is relatively unchanged. Alternatively, cardiac α1 receptors may contribute to the inotropic effect. At equivalent inotropic doses, dobutamine enhances automaticity of the sinus node to a lesser extent than doe’s isoproterenol; however, enhancement of atrioventricular and intraventricular conduction is similar for both drugs [1].
Absorption, Distribution, Metabolism and Elimination of Dobutamine
Dobutamine has a half-life of about 2 min in adults; the major metabolites are conjugates of dobutamine and 3-O-methyldobutamine. The onset of effect is rapid. Steady-state concentrations generally are achieved within 10 min of initiation of the infusion by calibrated infusion pump. The rate of infusion required to increase cardiac output typically is between 2.5 and 10 µg/kg per min although higher infusions rates occasionally are required. The rate and duration of the infusion are determined by the clinical and hemodynamic responses of the patient [1].
Therapeutic Uses of Dopamine
Dobutamine is indicated for the short-term treatment of cardiac decompensation that may occur after cardiac surgery or in patients with congestive heart failure or acute myocardial infarction. Dobutamine increases cardiac output and stroke volume in such patients usually without a marked increase in heart rate. Alterations in blood pressure or peripheral resistance usually are minor, although some patients may have marked increases in blood pressure or heart rate. An infusion of dobutamine in combination with echocardiography is useful in the non-invasive assessment of patients with coronary artery disease [1]. Deciding to use an inotrope and then choosing the right inotrope requires an understanding not only the physiological and pathological processes occurring in the infant but also of how various inotropes work. Whilst dopamine appears to result in a better blood pressure, dobutamine seems to be better at improving systematic blood flow, and there is a growing consensus that, although it is harder to measure, cardiac output and systemic tissue perfusion usually matter more than blood pressure. Milrinone could be tried if dobutamine proves ineffective, although there also may be an argument for using adrenaline or norepinephrine [2]. Dobutamine is used in the treatment of hypoperfusion especially if related to myocardial dysfunction. Monitor continuously the heart rate and intra-arterial blood pressure and observe the intravenous site for signs of extravasation. Dobutamine may cause hypotension if the infant is hypovolemic. The volume loading is recommended before starting dobutamine therapy, tachycardia occurs at high dosage, and arrhythmias, hypertension, and cutaneous vasodilation may occur. Increases myocardial oxygen consumption and tissue ischemia occurs with infiltration. Dobutamine is incompatible with acyclovir, alteplase, aminophylline, cefepime, bumetanide, diazepam, digoxin, furosemide, ibuprofen, lysine, indomethacin, micafungin, phenytoin, phenobarbitone, piperacillin-tazobactam, and sodium bicarbonate [3].
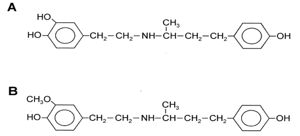
(A) Molecular structure of dobutamine (molecular weight = 301.38 grams/mole)
(B) Molecular structure of 3-O-methyldobutamine (molecular weight = 315.4 grams/mole)
Literature Search
The literature search was performed electronically using PubMed database as search engine and the following key words were used: “dobutamine dosing infants, children”, “dobutamine effects infants, children”, “dobutamine adverse-effects infants, children”, “dobutamine metabolism”, “dobutamine pharmacokinetics infants, children”, and “dobutamine treatment infants, children”. In addition, the books: The pharmacological Basis of Therapeutics [1], Neonatal Formulary [2], NEOFAX® by Young and Mangum [3], and The British National Formulary for Children [4] are consulted.
Administration Schedules of Dobutamine to Infants and Children
Intravenous administration to infants [4]
Treatment of inotropic support in low cardiac states, after cardiac surgery, cardiomyopathies, and shock
Infants
Give initially 5 µg/kg per min by continuous intravenous infusion, and then adjust the dose according to the response to 2 to 20 µg/kg per min, doses as low as 0.5 to 1 µg/kg per min have been used.
Treatment of inotropic support in low cardiac states, after cardiac surgery, cardiomyopathies, and shock
Children
Give initially 5 µg/kg per min by continuous intravenous infusion, and then adjust the dose according to the response to 2 to 20 µg/kg per min, doses as low as 0.5 to 1 µg/kg have been used.
Effects of Dobutamine in Infants and Children
Dopamine and dobutamine both increase the systemic blood pressure, though dopamine is more effective in very-low-birth weight infants [5]. Dopamine is more effective than dobutamine in the short term treatment of systemic hypotension in preterm infants [6]. Dopamine is more effective than dobutamine in rising and maintaining mean arterial pressure above 30 mm Hg; however dopamine does not increase left ventricular output [7]. Isoprenaline is more effective than dobutamine in raising cardiac index due to the increase in heart rate. Moreover, dobutamine decreases systemic vascular resistances and obviates the need for administration of a vasodilator [8]. Dobutamine and dopamine are equipotent inotropes in young children and dopamine at doses > 7 µg/kg per min causes pulmonary vasoconstriction an effect mediated by α adrenergic receptors [9]. Dobutamine infused at a dose of 3.80+0.45 µg/kg per min causes myocardial ischemia in patients with coronary artery disease [10]. Dobutamine, infused at a dose of 7 µg/kg per min, increases the left ventricular stroke volume in response to inotropic stimulation [11]. After coronary artery bypass surgery, dobutamine increases the systemic and regional blood flows and decreases systemic and regional oxygen extraction [12]. Dobutamine increases gastric mucosal perfusion but does not alter hepatocytic clearance in patients with septic shock [13]. Dobutamine is used to increase cardiac output in infants and children with circulatory failure [14]. Dobutamine is a useful drug in the pharmacologic management of children with shock especially in children aged > 12 months with cardiogenic shock not complicated by severe hypotension [15]. Dobutamine effectively improves systolic function in critically ill children [16]. Dobutamine increases the cardiac index only by increasing heart rate [17].
Common or Very Common Adverse-Effects Caused By Dobutamine in Infants and Children [4]
Arrhythmias, bronchospasm, chest pain, dyspnoea, eosinophilia, fever, localised inflammation, ischemic heart disease, nausea, palpitations, platelet aggregation inhibition (on prolonged administration), skin reactions, urinary urgency, and vasoconstrictions.
Uncommon adverse-effects caused by dobutamine in infants and children [4]
Myocardial infarction.
Rare or very rare adverse-effects caused by dobutamine in infants and children [4]
Atrioventricular block, cardiac arrest, coronary vasospasm, hypertension, hypokalaemia, and hypotension.
Adverse-effects caused by dobutamine in infants and children whose frequency is not known [4]
Anxiety, cardiomyopathy, feeling hot, headache, myoclonus, paraesthesia, and tremor.
Metabolism of dobutamine
Dobutamine is O-methylated at position 3 [18] and dobutamine is conjugated with glucuronic acid in 4 positions [19].
Pharmacokinetics of dobutamine in infants and children
Schwartz et al. [20] studied the pharmacokinetics in 27 infants and children, aged 0.13 to 26.6 years (mean 5.2) and weighing 3.7 to 73.2 kg (mean 18.7), dobutamine was intravenously infused at a dose of 1 to 25 µg/kg per min, and the duration of infusion was 1.87+0.29 days (range, 0.2 to 5.5)
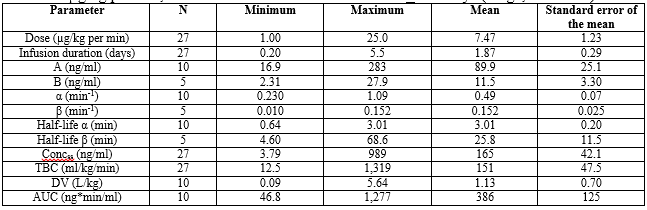
α and β are the first order rate constant of distribution and elimination, and A and B are the intercepts at time t = 0, respectively. Concss = dobutamine concentration at steady-state, TBC = total body clearance. DV = distribution volume.
This table shows that β is greater than α. Dobutamine is rapidly distributed and rapidly eliminated, the distribution volume is similar to the water volume, and there is a remarkable interindividual of the pharmacokinetic parameters. Such variability may be accounted by the wide variation of the demographic parameters of subjects.
Treatment of infants and children with dobutamine
Dobutamine is particularly suited to treatment of haemodynamic insufficiency caused by increased peripheral vascular resistance and myocardial dysfunction in preterm infants [21]. The prevalence of dopamine or dobutamine use is 4.9% in preterm or low-birth-weight infants and 25.1% in very-low-birth-weight infants [22]. Both dopamine and dobutamine have comparative efficacy in certain disease states with immature myocardium but there is advantages in using dobutamine [23]. Infants treated with dopamine and dobutamine have a higher cardiac output and heart rate than infants treated with dopamine alone [24]. Low doses of dobutamine stress echocardiography is feasible and safe in older children [25]. Low doses of dobutamine stress echocardiography may be useful for detecting and following cardiac dysfunction in children at risk for cardiac hemosiderosis [26].
Dobutamine resembles dopamine structurally but possess a bulky aromatic substituent on the amino group. The pharmacological effects of dobutamine are due to direct interactions with α and β receptors. Dobutamine possess a centre of asymmetry; both enantiomer forms are present in the racemate and are used clinically. The (-) isomer of dobutamine is a potent α1 agonist and can cause marked pressor response. In contrast, (+) dobutamine is a potent α1 receptor antagonist which can block the effects of (-) dobutamine. Both isomers are full agonist at β receptors; the (+) isomer is a more potent β agonist than the (-) isomer by about 10-fold. Dobutamine is indicated for the short-term treatment of cardiac decompensation that may occur after cardiac surgery, in patients with congestive heart failure, or in patients with acute myocardial infarction. Dobutamine increases cardiac output and stroke volume in such patients, usually without a marked increase in the heart rate [1]. Whilst dopamine appears to result in a better blood pressure, dobutamine seems to be better at improving systematic blood flow, and there is a growing consensus that, although it is harder to measure, cardiac output and systemic tissue perfusion usually matter more than blood pressure [2]. Dobutamine is used in the treatment of hypoperfusion especially if related to myocardial dysfunction [3]. Dobutamine is administered by continuous intravenous infusion and the initial dosage of dobutamine is 5 µg/kg per min, and the dose is adjusted according the response to 2 to 20 µg/kg per min in both infants and children [2, 4]. The effects of dobutamine have been described in infants and children [5-17]. Dopamine is more effective than dobutamine in increasing arterial blood pressure in infants [5-7]. Isoprenaline is more effective than dobutamine in rising and maintaining arterial pressure > 30 mm Hg, but dobutamine decreases systemic vascular resistance and obviates the need for administration of a vasodilator [8]. Dobutamine and dopamine are equipotent inotropes and dopamine given at doses > 7 µg/kg per min causes vasoconstriction, an effect mediated by α adrenergic receptors [9]. Dobutamine infused at a dose of 3.80 µg/kg per min causes myocardial ischemia in patients with coronary artery disease [10]. And dobutamine infused at a dose of 7 µg/kg per min increases the left ventricular stroke volume in response to inotropic stimulation [11]. After coronary artery bypass surgery, dobutamine increases the systemic and regional blood flows and decreases systemic and regional oxygen extraction [12]. Dobutamine increases gastric mucosal perfusion but does not alter hepatocytic clearance in patients with septic shock [13]. Dobutamine increases cardiac output in infants and children with circulatory failure [14], and dobutamine is used in the pharmacological management of children with cardiogenic shock not complicated by severe hypotension [15]. Dobutamine effectively improves systolic function in critically ill children [16], and dobutamine increases the cardiac index in children only by increasing heart rate [17]. Dobutamine may cause adverse effects which are classified as common or very common, uncommon, and rare or very rare [4]. Dobutamine is methylated [18] and it is also conjugated with glucuronic acid [19]. Following continuous intravenous infusion, the distribution half-life is 3.01 min, the elimination half-life is 25.8 min, and the distribution volume is 1.13 L/kg, suggesting that dobutamine is rapidly distributed, is rapidly eliminated, and the distribution volume is similar to the water volume [20]. The treatment on infants and children with dobutamine has been studied [21-26]. Dobutamine is used in the treatment of haemodynamic insufficiency caused by increased peripheral vascular resistance and myocardial dysfunction in preterm infants [21]. The prevalence of dopamine or dobutamine use is 4.9% in preterm infants and 21.1% in very-low-birth-weight infants [22]. Both dopamine and dobutamine have comparative efficacy in disease states with immature myocardium but dobutamine has some advantages [23]. Infants treated with dopamine and dobutamine have a higher cardiac output and heart rate than infants treated with dopamine alone [24]. Low doses of dobutamine may be useful for detecting cardiac dysfunction in children at risk for cardiac hemosiderosis [25, 26].
In conclusion, dobutamine resembles dopamine structurally but possess a bulky aromatic substituent on the amino group. The pharmacological effects of dobutamine are due to direct interactions with α and β receptors. Dobutamine possess a centre of asymmetry; both enantiomer forms are present in the racemate and are used clinically. The (-) isomer of dobutamine is a potent α1 agonist and can cause marked pressor response. In contrast, (+) dobutamine is a potent α1 receptor antagonist which can block the effects of (-) dobutamine, both isomers are full agonists at β receptors, and the (+) isomer is a potent β agonist than the (-) isomer by about 10-fold. Dobutamine is used in the short treatment of cardiac decompensation that may occur after cardiac surgery in infants with congestive heart failure or acute myocardial infarction. Dobutamine is also used in the treatment of hypoperfusion especially if related to myocardial dysfunction. Dobutamine is administered by continuous intravenous infusion, and the initial dosage of dobutamine is 5 µg/kg per min in infants and children. The effects of dobutamine in infants and children have been extensively studied and consist in increasing the systemic blood pressure, the left ventricular stroke volume, and the cardiac output. Some authors stated that dopamine is more effective than dobutamine in the treatment of systemic hypotension whereas other authors observed that dobutamine and dopamine are equipotent inotropes. Dobutamine is methylated and it is also conjugated with glucuronic acid. The pharmacokinetics of dobutamine have been studied in infants and children following continuous intravenous infusion. Dobutamine rapidly distributes, it is rapidly eliminated, and the distribution volume is similar to the water volume. The treatment of infants and children with dobutamine has been extensively studied; dobutamine is used in the treatment of hemodynamic insufficiency, increase cardiac output, and low doses of dobutamine are useful in the treatment of cardiac dysfunction. The aim of this study is the review the clinical pharmacology of dobutamine in infants and children.
The authors declare no conflicts of financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employments, gifts, and honoraria.
This article is a review and drugs have not been administered to men or animals.
The author thanks Dr. Patrizia Ciucci and Dr. Francesco Varricchio, of the Medical Library of the University of Pisa, for retrieving the scientific literature.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
