
Case Report | DOI: https://doi.org/10.31579/2578-8965/193
1 Obstetrician-Gynecologist. Pediatric Gynecology Section, British Hospital of Buenos Aires, Argentina.
2 Pediatrician, Pediatric Service, British Hospital of Buenos Aires, Argentina.
3 Pediatrics Resident, British Hospital of Buenos Aires.
4 Pathology Physician, British Hospital of Buenos Aires.
5 Chief of Pediatric Service, British Hospital of Buenos Aires, Argentina.
6 Chief of Pediatric Gynecology Section, British Hospital of Buenos Aires, Argentina.
*Corresponding Author: Othatz L, Obstetrician-Gynecologist. Pediatric Gynecology Section, British Hospital of Buenos Aires, Argentina.
Citation: Othatz L, Graziani MP, Azula ME, Toscano M, Rojo G, (2023), Clinical Features and Decision making of Congenital Vaginal Agenesis Combined with Cervical Aplasia: Case Report and Literature Review, J. Obstetrics Gynecology and Reproductive Sciences, 8(1) DOI:10.31579/2578-8965/193
Copyright: © 2023, Othatz L. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 December 2023 | Accepted: 28 December 2023 | Published: 08 January 2024
Keywords: vaginal atresia; cervical aplasia; hysterectomy; abdominal pain; kbg syndrome
Objective: To present the case of a teenage girl with vaginal agenesis and review current literature on recommended courses of action.
A 12-year-old girl with KBG genetic syndrome was admitted to the Pediatric Unit with recurrent acute abdominal pain, vomiting, dehydration, and primary amenorrhea. Physical examination revealed advanced pubertal development, and a negative swab test. Magnetic Resonance Imaging (MRI) showed complete vaginal agenesis, septated uterus with cervical aplasia, hematometra, and hematosalpinx. Open hysterectomy was decided upon due to acute abdominal pain and the risk of endometriosis and infection. She progressed favorably and was discharged two days after surgery.
Conclusion: Congenital complete vaginal agenesis with cervical aplasia is a rare obstructive malformation of the genital tract. Generally, hysterectomy is recommended due to the high risk of stenosis, infection, and adhesions. Vaginoplasty is an option when the patient is mature enough to undergo the procedure. Attempts to preserve the uterus and fertility in patients with complete cervical atresia have a small sample size. In this case, the decision to perform a hysterectomy was considered the most appropriate to suit her social circumstances.
Congenital complete vaginal atresia with cervical aplasia/agenesis is a rare obstructive malformation of the genital tract, classified as complete or partial atresia. (1) Cervical agenesis is a rare congenital Müllerian anomaly, with an incidence of 1:80,000 to 1:100,000 newborns. Its association with vaginal agenesis is even more uncommon, reported in 39% of cervical agenesis cases (2). Cervical or cervicovaginal agenesis typically presents around the age of menarche with primary amenorrhea and/or cyclic abdominal pain. In these cases, the endometrium functions normally, but menstrual blood lacks an outlet. Partial vaginal atresia cases may also present with hematocolpos. (3).
The condition may worsen with hematosalpinx and endometriosis if left undiagnosed. Early diagnosis and management are crucial in these cases to prevent disease progression (4,5,6).
The KBG Syndrome is a rare genetic disorder with approximately 59 reported cases worldwide. It is caused by a mutation in the ANKRD11 gene, inherited in an autosomal dominant manner, affecting neurodevelopment and characterized by macrodontia From the incisors, neurological delay, craniofacial anomalies, short stature, among other conditions (7). Little is known about gynecological malformations associated with the KBG syndrome.
We present a clinical case of a 12-year-old adolescent girl with non-evolving chronic encephalopathy and the KBG genetic syndrome, who sought emergency care for recurrent acute abdominal pain. She was admitted to the pediatric unit with vomiting and dehydration for intravenous hydration and diagnostic evaluation.
As a relevant background, she had several visits to the pediatric emergency department two months prior due to abdominal pain, vomiting, oral intolerance, and dehydration. The mother stated that for the past 6 months, the patient used to cry for a few days each month due to abdominal pain.
The patient had not yet experienced menarche, and within this context, the pediatric gynecologist performed an abdominal-pelvic physical examination, revealing pubertal development at Tanner stage 4 for breast and genitalia, normal insert urethral meatus, absence of vaginal opening, and a negative swab test.
An abdominal ultrasound (US) (Figure 1) was performed, and she was evaluated by pediatric surgery, which ordered a computed tomography (CT) scan showing an incomplete septate uterus, hematometra, and hematosalpinx. No differentiation between the cervix and uterus was found, and no vaginal cavity was observed. A Müllerian anomaly was suspected, prompting a magnetic resonance imaging (MRI) for further details.
The MRI revealed bilateral ureteropelvic calyceal ectasia, an enlarged uterus with endometrial cavity distension and the presence of a septum, a 22mm hematometra, with no recognizable external cervix (Figure 2A). The vagina was not visible (Figures 2B, 2C, 2D, and 2E). Other findings included dilated Fallopian tubes (hematosalpinx), normal bilateral ovaries, and superficial endometriosis.
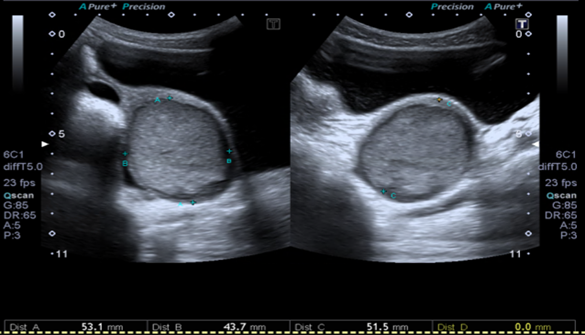
Figure 1: Gynecological Pelvic Ultrasound: In the left iliac fossa, an irregular and heterogeneous image with echoes and vascularity measuring 53 x 44 x 51 mm.
The day before surgery, the patient had a fever with a recorded temperature of 38°C. The parents provided their consent for the surgery, including the option of a hysterectomy if deemed necessary.
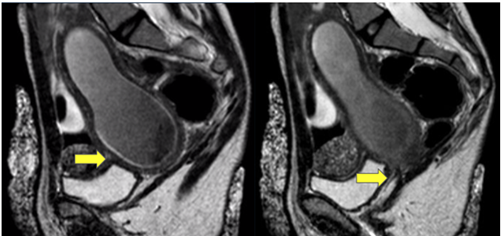
Figure 2. Magnetic Resonance Imaging (RMI)
Figure 2A: The yellow arrow indicates an enlarged uterus with hematometra. The anteverted uterus measures 100 x 32 x 59 mm, with the endometrium divided by a 90° angle indentation, creating two cavities (incomplete septate uterus).
Figure 2B: No external opening, hematometra. The vagina is not visible, showing a hyperintense fibrous image in T1 and T2, suggesting a vaginal remnant (hypoplastic vagina).
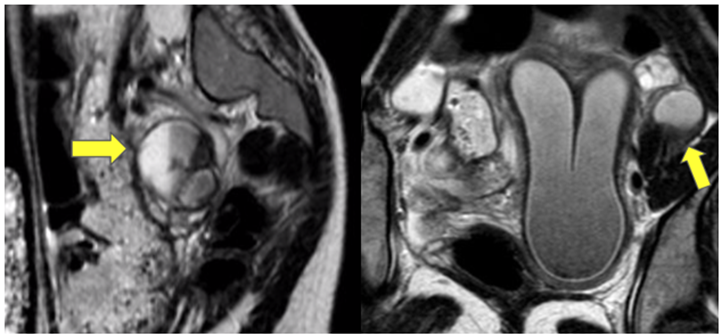
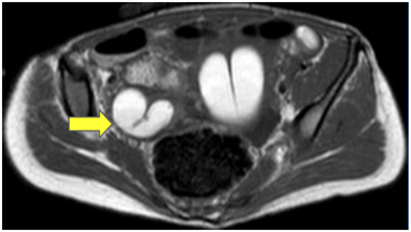
Figures 2C, 2D, 2E: Both adnexal regions show hematosalpinx (39 x 27 mm on the right and 47 x 26 mm on the left). Ovaries appear normal, and there is thickening of the peritoneal tissue, likely superficial endometriosis.
In the context of acute abdominal pain and the risk of endometriosis and infection, an open hysterectomy was decided upon. A Pfannenstiel incision/laparotomy was performed, with a detailed examination of the abdominal and pelvic cavity.

Figure 3A: Incomplete septate uterus.

Figure 3B: Uterus with hematosalpinx.
A bicornuate uterus with hematosalpinx and adhesions of the left fallopian tube to the posterior aspect of the uterus was found. Absence of cervix and vaginal cavity (Figure 3A, 3B, 3C, 3D).

Figure 3C: Cervical aplasia.
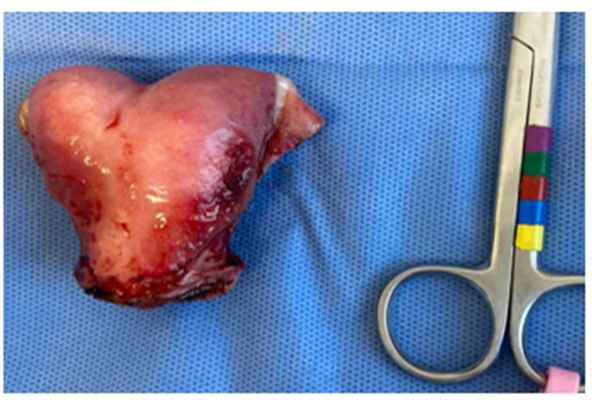
Figure 3D: Size of the bicornuate uterus.

Figure 3E: Cut and section, Macroscopy of the uterus.
The uterus and fallopian tubes were resected. The patient progressed favorably. She did not require analgesics on the day following the surgery and was discharged 48 hours later. Histology confirms a partially septate uterus with two cavities and hematosalpinx.
Histology:

Figure 4A: Myometrium composed of short fascicles, lined by inactive endometrial mucosa with small and regular glands, and congestive vessels.

Figure 4B: Uterine septum composed of smooth muscle and fibrous tissue, lined by endometrial mucosa with identical characteristics to the mucosa of the rest of the cavity.
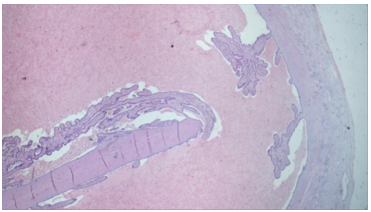
Figure 4C: Uterine tube with dilated lumen containing hematic content, flattened folds, and thin, congested wall.
Cervicovaginal agenesis is a rare congenital anomaly of the female genital tract. Only a few isolated cases and case series have been reported in the literature, with fewer than 200 cases published (8). While clinical history and physical examination are crucial in these cases, pelvic imaging should be considered to understand the exact anatomical anomaly. Magnetic resonance imaging (MRI) is considered the gold standard for diagnosis, as well as for detecting associated renal tract abnormalities (9). The most common symptom is primary amenorrhea with cyclic abdominal pain and/or chronic pelvic pain, palpable mass in the abdomen, and urinary symptoms. This symptomatology should lead to consideration of a gynecological problem. Müllerian anomalies tend to be asymptomatic until puberty, and sometimes their expression depends on the type of anomaly. Specifically in this clinical case, the KBG syndrome complicates the diagnosis due to intellectual disability and the rare nature of the pathology. This condition is not trivial and should be considered, along with the family, when deciding on therapeutic alternatives (hysterectomy versus tracheloplasty + vaginoplasty).
According to the literature, most publications recommend hysterectomy for cervical agenesis, complete cervical and vaginal atresia, due to the high risk of cervical stenosis, adhesions, pelvic inflammatory disease, and endometriosis, even when the cervix is open. Vaginoplasty is recommended in late adolescence or early adulthood when the patient is mature enough to accept the procedure (4,6,10). For patients with obstruction of the external cervical orifice, cervicovaginal anastomosis may offer an alternative treatment to preserve menstruation and even fertility. However, experience in cervicovaginal anastomosis reconstruction is limited, and there is still much to be investigated, such as evaluating successful surgery outcomes, maintaining the cervical canal, or preventing vaginal and cervical stenosis (2,11).
According to Dietrich J et al., out of more than 19 patients with clinical characteristics of congenital complete vaginal atresia combined with cervical aplasia, 13 underwent hysterectomy (2 of them with subsequent vaginoplasty), tracheloplasty plus vaginoplasty were performed in six patients, four of whom had complications (adhesions, stenosis, pelvic inflammation), three of them required a second vaginoplasty, and one underwent hysterectomy two years later due to recurrent pelvic inflammation (6).
Embryologically, only 2% to 7% of patients with partial or total vaginal aplasia have active endometrium in uterine structures. Sporadic cases of vaginal atresia combined with a functional uterine anomaly have been described, but the coincidence of a septate uterus has not been reported, even though it comprises approximately 53.7% to 55% of all female genital anomalies (10). Only one case of vaginal atresia combined with asymmetric septate uterus was published in 2018 by Tian-Tian H. Additionally, this case is unique because no obstructive gynecological malformation was described in the KBG syndrome, and, according to the literature, this is the second case of septate uterus with cervical aplasia and complete vaginal agenesis.
Our case highlights that Müllerian duct anomalies should be considered in the differential diagnosis of cyclic abdominal pain, especially in patients with primary amenorrhea, fully estrogenized, who cannot communicate their symptoms. Early diagnosis and management are crucial in these cases to prevent disease progression.
Gynecological teams have attempted to preserve the uterus and fertility in patients with complete cervical atresia, but the sample size has been small (3,9). More high-quality, controlled multicenter clinical trials with longer follow-up are needed for further evaluation.
A digital search on PubMed was conducted to identify articles published from the year 2000 to the present reporting cases of complete vaginal atresia with cervical aplasia (Table 1). The following search terms were used: "Vaginal atresia," "Vaginal aplasia," "Vaginal agenesis," "Cervical atresia," "Cervical agenesis," or "Cervical aplasia." Inclusion criteria were as follows: (a) Patients diagnosed with congenital complete vaginal atresia accompanied by cervical aplasia who underwent surgery for the first time and preserved their uteri; (b) primary outcomes were vaginal or cervical stenosis, pelvic inflammation; if a second surgical treatment was required, the length and width of the new vagina. Results were summarized in the following table:
Author (year) | Age of presentation (years) | Clinic presentation | Examination finding | Imaging (USD/MRI) | Management | Outcome |
|---|---|---|---|---|---|---|
Mei, et al (1) (2021) | Median age 14 N=19 | Periodic abdominal pain, pelvic mass Primary amenorrhea | No vaginal introitus | MRI Complete vaginal atresia and cervical aplasia | 13 hysterectomy (2 posterior vaginoplasty) 6 Tracheloplasty + vaginoplasty | 6 Tracheloplasty + vaginoplasty: 4 stenosis 2 PID 3 Second vaginoplasty 1 Hysterectomy |
Kavita Kohiual et al (8) (2021) | 13 | Acute abdominal pain, Primary amenorrhea | Blind vaginal pouch | US/MRI: Hematometra/ hematosalpinx | Cervicovaginoplasty And neovagina with McIndoe technique | Resumed normal menstrual cycles |
Meena et al (11) (2018) | 13 | Primary amenorrhea Cyclic abdominal pain history of vaginoplasty | blind vaginal | MRI: Leftsided uterine horn with hematometra, left endometriotic cyst, absent cervix | Laparoscopy excision of bilateral uterine horn | - |
Bagga et al(12) (2018) | 18 | Primary amenorrhea and cyclical abdominal pain; history of vaginoplasty | Blind vaginal pouch | MRI: Leftsided uterine horn with hematometra, left endometriotic cyst, absent cervix | Uterine horn-vaginal anastomosis by abdominoperineal approach | Resumed regular menstruation |
| Tian-Tian Han(9), et al (2018) | 23 | Dispareunia, abdominal pain, previous vaginoplasty | Abdominal pain | US: Asymmetric septate uterus MRI: distended endometrial cavity | Hysteroscopy Diagnosis and vaginal stent | - |
Acosta Leon J, et al(10) (2017) | 14 | Primary amenorrhea Cyclic pelvic pain | Small vaginal pouch | MRI: Absence of cervix and proximal vagina | 2 steps treatment: -Vaginoplasty (Yong-Monti technique)/MP -posterior uterus anastomosis | Regular menstrual cycles |
Mishra et al(13) (20216) | 16 | Primary amenorrhea Cyclic pelvic pain | Per Abdomen –deep tenderness | MRI: Hematometra /Hematosalpinx Absence of cervix and vagina | Laparotomy vaginoplasty (McIndoe method) uterovaginal anastomosis by neocervix | Regular menstrual cycles |
Jeon et al(14) (2016) | 2 cases (12/ 17) | Primary amenorrhea Cyclic pelvic pain | Blind vagina | MRI: Hematometra, Absence of cervix and vagina | Laparoscopy transvaginal uterovaginal anastomosis | Regular menstruation |
Kisku, et al(15) (2014) | Median age15 N=18 | Primary amenorrhea, Cyclic pelvic pain | Absent vaginal/ small vaginal pouch | - | Laparotomy and sigmoid neovaginoplasty utero-coloneovaginoplasty | Complications; one colon anastomotic leak, two patients developed chocolate cysts, one recurrent pelvic collection, one asymptomatic neovaginal prolapse |
Gasim et al(5) (2013) | 14 | Primary amenorrhea, Cyclic abdominal pain | Abdominopelvic mass up to xiphisternum | US: Blind upper vagina, bicornuate uterus with right hematometra | Laparotomy, hysterectomy, excision of left rudimentary horn and right salpingo-oophorectomy | - |
Kriplani et al(16) (2012) | Mean age: 15.2 N=14 | Primary amenorrhea Cyclic abdominal pain | - | - | laparoscopic assisted uterovaginal anastomosis | Successful; except one patient had restenosis, hysterectomy required |
Jain and Sircar(17) (2011) | 18 | Primary amenorrhea Cyclic abdominal pain | Absent Vagina | US: Cervical and vaginal agenesis, uterus, and right ovary normal. A 10 cm×10 cm endometriotic cyst in left ovary | Laparoscopic hysterectomy and neovagina creation by Vecchietti technique | - |
Raudrant el al (18) (2008) | 13 | Primary amenorrhea and cyclic pelvic pain | Blind vaginal pouch | US: Absence of the cervix with two rudimentary horns and a right hematometra | Laparoscopic uterovaginal anastomosis | Regular menstruation |
Fedele et al(3) (2008) | Mean age 14 N=12 | Primary amenorrhea and cyclic pelvic pain | Absent vagina/ Blind pouch | US/MRI Hematometra, hematosalpinx | Laparoscopically assisted uterovestibular anastomosis was performed in all patients. F | Regular menstrual cycles |
Gurbuz et al (19) (2005) | 15 | Primary amenorrhea, cyclic abdominal pain | Partial vaginal agenesis | US: Hematometra and absent cervix | Laparotomy and uterovaginal anastomosis | Resumed regular menstruation |
Grimbizis et al (20) (2004) | 15 | Primary amenorrhea Cyclic abdominal pain | - | US: Uteri corpus and both ovaries were normal | Laparotomy and end-to-end cervicocervical anastomosis | Regular menstruation |
Table 1: Previous Reported Cases of Cervicovagina Agenesia
Congenital complete vaginal atresia with cervical aplasia/agenesis is a rare obstructive malformation of the genital tract. The most common symptom is primary amenorrhea with cyclic abdominal pain and/or chronic pelvic pain, along with a palpable abdominopelvic mass.
The clinical presentation of this pathology, in conjunction with the KBG syndrome, complicates the diagnosis due to intellectual disability and the rare nature of the condition. This intellectual disability is considered an additional factor when deciding on the best therapeutic alternative, given the extensive evidence of complications associated with surgical reconstruction.
Although technical advancements favor reconstructive surgery for cervicovaginal agenesis, it is important to remember that these complex procedures are not without complications, which may lead to the recurrence of hematometra and, ultimately, necessitate hysterectomy. In this case, the decision to proceed with a hysterectomy was deemed the most appropriate given her social circumstances.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
