
Case Report | DOI: https://doi.org/10.31579/2690-1919/282
1 The State Budgetary Institution of Higher Professional Education «Voronezh State Medical University named after N.N. Burdenko» of the Ministry of Public Health of the Russian Federation, Voronezh, Russia
2 Limited Liability Company "Sudareva Clinic», Voronezh, Russia
3 The State Budgetary Institution of Higher Professional Education «Voronezh State Medical University named after N.N. Burdenko» of the Ministry of Public Health of the Russian Federation, Voronezh, Russia
4 The State Budgetary Institution of Higher Professional Education «Voronezh State Medical University named after N.N. Burdenko» of the Ministry of Public Health of the Russian Federation, Voronezh, Russia
5 The State Budgetary Institution of Higher Professional Education «Voronezh State Medical University named after N.N. Burdenko» of the Ministry of Public Health of the Russian Federation, Voronezh, Russia
*Corresponding Author: Elena. V. Vusataya. The State Budgetary Institution of Higher Professional Education Voronezh State Medical University named after N.N. Burdenko of the Ministry of Public Health of the Russian Federation, Voronezh, Russia.
Citation: Elena. V. Vusataya, Roman G. Pomogalov, Olga I. Oleinik, Andrei V. Sushenko, Oksana P. Krasnikova. (2022). Clinical case: second mandibular premolar with three root canals, J. Clinical Research and Reports, 11(5) DOI:10.31579/2690-1919/282
Copyright: © 2022 Elena. V. Vusataya. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 31 August 2022 | Accepted: 19 September 2022 | Published: 29 September 2022
Keywords: second lower premolar; clinical case; endodontic treatment; root canal anatomy
The effectiveness and success of endodontic treatment depends on the doctor's professionalism and knowledge of the anatomy and morphology of root canals. The equipment that is at the disposal of the dentist is also of great importance. At the moment, it is difficult to imagine the diagnosis of complex endodontic pathology without the use of cone-beam computed tomography. Diagnostic radiographs in different projections are important for getting an idea of the number of existing root canals, but do not always give a complete picture of the anatomy and morphology of root canals. Magnifying devices (binoculars and dental microscope) are also very helpful for competent treatment in modern dentistry in general and endodontics in particular. Premolars of the mandible are among the most difficult teeth for endodontic treatment due to a sufficient number of variations in internal morphology, the presence of additional root canals, apical deltas and lateral canals.
The goal of endodontic treatment is always to clean the root canal of pathogenic microbes and infected pulp, prevent the formation of toxic products and protect the periapical tissue. The presence of root canal variability increases the complexity of endodontic treatment. The complex anatomy of the root canals, the presence of additional channels, unnoticed by the dentist, can cause the failure of endodontic treatment [1]. A wide variety of variations of anatomy in relation to the number and shape of roots and root canals are presented in literary sources [2, 3]. For several decades, this topic has been the subject of many experimental and clinical studies. Lack of knowledge about anatomical variants can lead to untreated canal space, which can potentially lead to failure of endodontic treatment [4]. Premolars of the mandible often have a complex anatomy that cannot be clearly detected on two-dimensional periapical radiographs [5]. With the advent of high-precision technologies, cone-beam (CBCT) and X-ray computed microtomography, as well as the use of various degrees of magnification (binoculars, operating microscope) in clinical practice have significantly expanded the understanding of the complexity of the structure of the root canal system. According to various studies, there is more and more information that the numerous channels inside the root together represent a very complex system consisting of the main, additional channels, lateral branches and the apical delta [6]. In addition, it is generally recognized and proven that the structure of roots and channels can vary greatly in different races, within the same population group, and even in a single person. Anatomical variations in the root canal system of the second premolar of the mandible are known. For example, Vertucci found that the second lower premolar has 1 root, 1 oval or round channel in 97.5% and a channel bifurcating at the apex in 2.5% [7]. Other authors, according to Grigoriev S.S., 2019, admit that other variations may sometimes occur [8]. For example, two channels ending with one apical opening (4%), or two independent channels (4%), as well as a two-root tooth. Variations in anatomy were demonstrated by the research of B. Willershausen and co-authors in 2009. It has been shown that the probability of root canal curvature in the premolars of the human mandible has a sigmoid line, that there is a tendency to increase the curvature of the root canal length in the range from 9 to 12 mm and that in the premolars of the mandible one can expect a large deviation from the original channel path by 9 mm from the cement-enamel joint [9]. Xuan Yu and co-authors (2012) examined the upper and lower premolars in the Chinese population. All 178 mandibular second premolars had one root. Of these, 97.2% of the teeth had one channel and 2.2% had two. The prevalence of C-shaped channels was 0.6%. All 178 second premolars of the mandible were single–rooted and the canal configurations of these teeth according to the Vertucci classification were most often type I (173 teeth, 97.2%), type II was found in one tooth (0.55%) and type V - in three teeth (1.7%). Only one tooth had a C-shaped configuration (0.55%). In both the first and second premolars of the mandible, having morphology type V or type VIII, bifurcation of the canal was found in the mid-apical part of the root, where 87% and 75% of the variations of the canal system occur in the first and second premolars of the mandible, respectively [10].
The purpose of this study is to present a clinical case with a complex anatomy of the lower second premolar.
A clinical case. The patient, a man, 43 years old, without concomitant somatic diseases, sought dental help. Clinical examination revealed deep caries on the 45th tooth. According to the treatment plan, the patient was shown the replacement of the missing 46 tooth, the patient refused implantation, so they decided to replace the missing defect with a non-removable bridge prosthesis supported by 45 and 47. Since the amount of dentin to the pulp chamber after excision of carious tissues was less than 0.4 mm, and the cold test (RoekoEndo-Frost, Coltene) provoked the development of pain for 20 seconds. it was decided to carry out endodontic treatment of the 45th tooth. In addition, during the analysis of the radiograph, the presence of an area of X-ray translucency (carious cavity) was identified, the bottom of which bordered the pulp chamber (Figure 1).
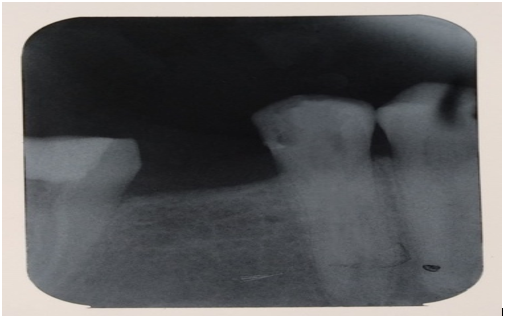
Figure 1: Sighting radiograph of the second premolar of the lower jaw before treatment.
During the first visit after anesthesia and isolation, access to the root canals was formed, the mouth of the third canal could not be detected, after chemo-mechanical treatment, the treated root canals were filled with calcium hydroxide. For better visualization, it was decided to continue the treatment of the 45th tooth using the PRIMALABOMED surgical operating microscope (Labo America Inc., USA) with preliminary CBCT examination. Axial, coronal and sagittal sections of CBCT (CS 9300, Carestream Dental) (internal software version 3.5.15.0 at 5 cm x 5 cm, 85 kV, 8 mA, 20 s, 985 mGr • cm2) revealed the presence of three channels (Figure 2-3).
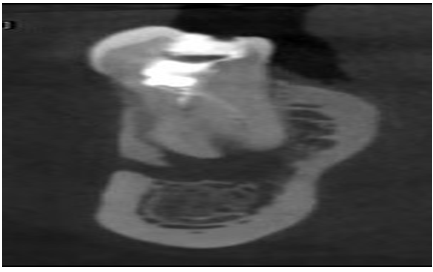
Figure 2: Coronal CBCT section: visualization of two roots.
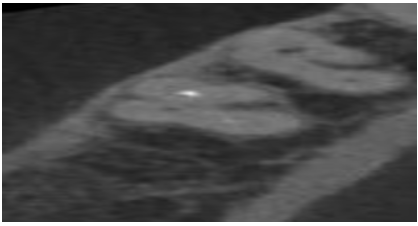
Figure 3: Axial CBCT section: visualization of three root canals.
The working length was determined using the Root PII apex locator (DENJOY DENTAL Co. LTD., China) and was supported by radiography. The channels were cleaned and formed using Profile (Dentsply Mallifer, Switzerland) to a final size of 30.04. Irrigation of the channels was carried out with 3% sodium hypochlorite and 17
The second premolar of the mandible is one of the most difficult teeth for endodontic treatment due to variations in internal morphology, additional root canals, apical deltas and lateral canals. Diagnostic radiographs in different projections are important for getting an idea of the number of existing root canals. As a rule, in premolars of the lower jaw with three channels, the upper half of the root is wider than usual, with little or no narrowing. Root canals may not be visible on radiographs and may look unusual. A sudden change in radiographic density and a sudden narrowing of the root canal space usually indicates the presence of an additional canal. Therefore, when carefully interpreting the periodontal space, many assume the presence of an additional root or channel. The use of binoculars, fiber-optic illumination to observe anatomical landmarks in the pulp chamber, sodium hypochlorite bubbling in additional channels, and dyes, for example methylene blue, can be useful when detecting additional channels.
The authors declare that there is no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
