
Research Article | DOI: https://doi.org/10.31579/2578-8868/302
*Corresponding Author: Giulio Perrotta. Istituto per lo Studio delle Psicoterapie (ISP), Rome, Italy.
Citation: Giulio Perrotta, (2024), Clinical application of the “Perrotta-Guerrieri Psychological Care for Ostomy Patients” (PCOP) protocol and integrated questionnaire on adult ostomy patients, J. Neuroscience and Neurological Surgery, 15(2); DOI:10.31579/2578-8868/302
Copyright: © 2024, Giulio Perrotta. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 12 February 2024 | Accepted: 28 February 2024 | Published: 07 March 2024
Keywords: colostomy; quality of life; body image after surgery; ostomy; altered body image; impact of ostomy; Ileostomy; Urostomy; pcop; perrotta-guerrieri psychological care for ostomy patients
Background. Much attention is paid in the literature to the psychological profiles associated with ostomies, but until 2022 there was a lack of a psychoclinic instrument that was able to investigate all 9 individual subjective functions possibly impaired by the ostomate condition and the degree of impairment. For this reason, "Perrotta-Guerrieri Psychological Care for Ostomy Patients" (PCOP) was developed for all clinical phases, in 45 items with an L1-5 response scale, for the study of quality of life in the ostomized patient, which was also able to offer from the therapist a holistic understanding of the problem in all its phases (pre-operative, operative, postoperative, follow-up), integrating a patient-specific clinical intervention protocol. Materials and Methods. Clinical interview and battery of psychometric questionnaires. Results. Of 58 patients (M: 57.3 years), divided into two groups (CG and Cg) of equal distribution, the group in which the protocol was applied (CG) achieved quantifiable benefits to the extent of 50-75% individually and 97% in the total group. Conclusions. PCOP is a psychoclinical tool that can offer therapists the opportunity to explore the issue of patient quality of life and best focus on the most appropriate and targeted clinical intervention.
Perrotta-Guerrieri Psychological Care for Ostomy Patients (PCOP). Perrotta-Guerrieri Psychological Care for Ostomy Patients Model (PCOP-M). Perrotta-Guerrieri Psychological Care for Ostomy Patients Questionnaire (PCOP-Q1).
The term "ostomy" means "opening" and denotes the result of a surgical procedure that involves attaching a section of the intestines or urinary tract to the skin, thus allowing organic material (feces and urine) to leak outward. The placement involves a substantial change in the person's body plan and fecal and urinary elimination function, involving not only his or her physical integrity but also, more importantly, his or her psychological integrity; therefore, the role of the psychologist should be central in all phases of the health care intervention (preoperative, operative, postoperative, and follow-up). [1-4]
There are several criteria for classifying ostomies, based on packaging, duration, structure, and motivation [5-8]; based on the geographic region of location, for simplicity, they are distinguished into ileostomies [9-11], colostomies [9, 12], and urostomies [9, 13-14]
In the literature, special attention is given to psychological profiles, as ostomy can significantly impair all dimensions of quality of life (physical, psychological, social, economic, and spiritual) in individuals who have not been adequately prepared for the change or who suffer from one or more complications during the grafting and healing phase, or who do not reach a degree of maturity of acceptance of their health condition. Ostomy patients are subject to significant negative psychological impacts, affecting their quality of life in all aspects (physical, psychological, social, economic, and spiritual), especially if they are not properly constructed or if there are complications during the recovery phase. Placing the focus only on managing the physical dimension will hardly allow the person to integrate the ostomy into his or her life. [15-37]
The concept of "quality of life" is therefore central to applied psychology. According to the definition provided by WHO in 1998, it should be understood as "the total of the subjective perceptions that individuals have of their place in life about the cultural context and value system in which they live and about their own goals, standards and interests". Quality of life is thus seen as a multidimensional concept that includes positive and negative perceptions concerning physical, emotional, social, cognitive and spiritual dimensions. Because of this importance, clinical attention in the field of psychology is particularly focused on clinical intervention to restore the patient's quality of life if he or she perceives it to have deteriorated. [38-65] For this reason, there are questionnaires in the literature that address this profile, and among the most cited are the Health-Related Quality of Life Self-Assessment Test (HRQOL), the Short Form Health Survey (SF-36), the WHO Quality of Life (WHOQOL), and the Stoma-Qol, [66] but none of these are able to investigate in a single psychometric instrument all 9 individual subjective functions possibly impaired by the stoma condition as does the "Perrotta-Guerrieri Psychological Care for Ostomy Patients" (PCOP), developed in 2022. [67] Based on this publication, the experiment depicted here was developed.
The main objective of the research, based on the results of the literature and this study, is to demonstrate the clinical utility of PCOP, on the participants of the selected population sample and to try to answer the following profiles: 1) ontological, i.e., whether the reality under investigation exists objectively (and thus whether it is possible to determine the clinical utility of the protocol); 2) epistemological, i.e., whether the reality under investigation is knowable (and whether it is possible to determine the degree to which the patient's quality of life is impaired by applying the questionnaire attached to the protocol) 3) methodological, i.e., whether the reality under consideration is measurable (and whether it is possible to graduate the intervention based on the level of impairment); 4) axiological, i.e., whether the reality under consideration is worthy of study (and thus whether, through the protocol, the structured clinical intervention has greater effectiveness than other approaches).
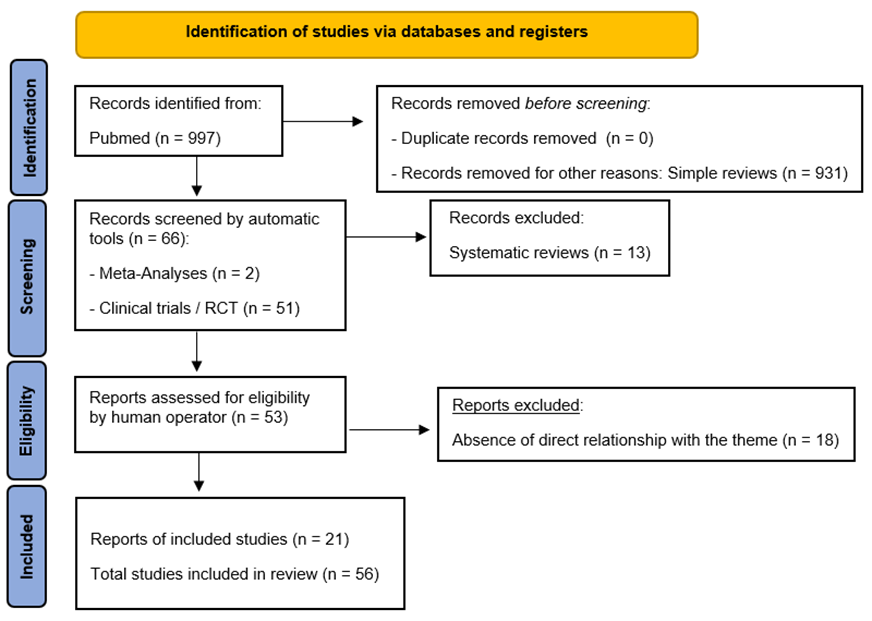
With a specific search on Pubmed, using the terminological indicators of "ostomy" and "psychology," 56 useful results were selected. No limit was placed on the year of publication, until the completion date of the study (January 2024). [Figure 1]
Figure 1. PRISMA flow diagram template. Matthew J Page et al. BMJ 2021; 372:bmj.n71.
The protocol of integrated psychological intervention for ostomate patients (PCOP) provides a specific active procedure consisting of actions aimed at the patient's intake, management, and clinical care; based on the phase in which the intake takes place (preoperative, operative, postoperative or follow-up), the protocol establishes precise clinical actions using the strategic approach in patient care and establishes certain psychometric tools to support the therapist and a precise schedule of therapeutic sessions, with techniques and strategies that also draw from cognitive-behavioral, constructivist, psychodynamic and humanistic approaches. [67]
<>. [67]
The method consists of applying the PCOP protocol, and using the PCOP-Q1 questionnaire, according to the patient's clinical stage, then comparing it with the group of patients who did not utilise the protocol. The phases of the research were divided as follows: 1) selection of the population sample, according to the parameters indicated in the following paragraph; 2) clinical interview, with each population group and protocol application; 3) administration of the psychometric tests; 4) PCOP-Q1 administration, 2 weeks after ostomy surgery and re-administration after the continuous cycle of psychotherapeutic sessions.; 5) data processing following administration and comparison of data obtained.
Inclusion criteria for the second clinical group (Cg) are: 1) age between 21 and 70 years; 2) defined sexual gender (male/female) and of Italian nationality; 3) need for definitive ostomy implantation, for clinical reasons; 4) declaration of non-submission to the PCOP protocol, following surgical pathway in a health care facility in the Italian System; and 5) absence of psychopathological diagnosis or known neurological and neurodegenerative disorders at the time of study participation. Exclusion criteria for the clinical group (Cg) are: 1) age less than 21 years and older than 70 years; 2) undefined sexual gender (transsexual and nonbinary) or nationality other than Italian; 3) need for non-definitive ostomy implantation, for clinical reasons; 4) declaration of non-submission to the PCOP protocol; 5) presence of psychopathological diagnoses or known neurological and neurodegenerative disorders at the time of study participation, of at least one of the two partners.
The selected setting, taking into account the protracted pandemic period, is the online platform via Skype and Video call WhatsApp, both for the clinical interview and for the administration. The present research work was carried out from September 2021 to January 2024.
The selected first population clinical sample (CG), which meets the requirements, is 29 partecipants, divided into 6 subgroups [Table 1]:
| Age | Male | Female | Total |
| 21-30 | 1 | 1 | 2 |
| 31-40 | 3 | 3 | 6 |
| 41-50 | 4 | 5 | 9 |
| 51-60 | 4 | 3 | 7 |
| 61-70 | 2 | 3 | 5 |
| Total | 14 (48%) | 15 (52%) | 29 (100%) |
Table 1: Population sample (numerousness) - CG.
The selected first population clinical sample (CG), which meets the requirements, is 29 partecipants, divided into 6 subgroups [Table 2]:
| Age | Male | Female | Total |
| 21-30 | 1 | 2 | 3 |
| 31-40 | 3 | 2 | 5 |
| 41-50 | 3 | 5 | 8 |
| 51-60 | 5 | 5 | 10 |
| 61-70 | 2 | 1 | 3 |
| Total | 14 (48%) | 15 (52%) | 29 (100%) |
The total population sample is 58 participants (M: 57.3 years).
Table 2: Population sample (numerousness) - Cg.
After the selection of the chosen population sample (first phase), we proceeded with the clinical interviews (second phase), from which the first significant data emerged:
The next phases of the research focused on the administration of PCOP-Q1 and the application of PCOP protocol steps. In particular [Tables 3-4]:
Test
|
CG |
Cg |
Δ CG/Cg |
M±DS |
P |
PCOP-Q1 (before) |
100% |
100% |
0% | CG = 177.6±21.1 Cg = 178.3±20.8 |
< 0> |
PCOP-Q1 (after) |
100% |
100% |
0% | CG = 83.1±16.3 Cg = 95.6±16.7 |
< 0> |
Table 3: S.P.S.S., T-test for tests and CG/Cg differential (descriptive)
Test
|
Groups |
CG (n/%) |
Cg (n/%) |
P |
PCOP-Q1 | 1 (21-30 y) | 2 (6.9%) | 3 (10.3%) | < 0> |
| 2 (31-40 y) | 6 (20.7%) | 5 (17.2%) | < 0> | |
| 3 (41-50 y) | 9 (31.1%) | 8 (27.7%) | < 0> | |
| 4 (51-60 y) | 7 (24.1%) | 10 (34.5%) | < 0> | |
| 5 (61-70 y) | 5 (17.2%) | 3 (10.3%) | < 0> |
Table 4: S.P.S.S., T-test for tests and groups.
The present study showed that with the use of the PCOP protocol and the PCOP-Q1 questionnaire, it is possible to improve the focus on the emotional and interpersonal problems of ostomate patients, centering therapeutic goals and fostering a more humanistic approach.
In the first clinical group (CG), those who scored greater than 50% of the total on the PCOP-Q1 in the first administration were 68/68 (100%); this figure is quite alarming, as it suggests that the psychological preparedness of these patients is severely inadequate and that an instructional plan needs to be put in place for patients before they can face the consequence of surgery. After the course of psychotherapeutic sessions, according to the protocol, data from the re-administration of the questionnaire showed a marked improvement in the psychological approach to ostomy persistence, but the data still show that early intervention could have brought greater benefits. The same argument should be made for the second clinical group (Cg), which has the same peculiarities, with markedly greater subjective data and therefore more alarming.
The use of the PCOP protocol and the PCOP-Q1 questionnaire is strongly recommended in the clinical setting, as their technical input concretely helps the therapist [71-72] in fostering the effectiveness of psychotherapeutic intervention and patients in improving their degree of acceptance by improving their quality of life.
The present study, however, has both structural and functional limitations that, in the opinion of the writer, do not affect the quality of the results obtained, but should be taken into consideration for future research to avoid analytical bias. Structurally, the design of the study involves the use of an unvalidated questionnaire, as there is no questionnaire in the literature capable of investigating all the areas (9 in total) studied by the PCOP-Q1; it was felt, therefore, that it could not be validated in the absence of a questionnaire capable of guaranteeing the correct comparisons, however, in the psychotherapeutic sessions provided by the protocol, as demonstrated in this study, it has demonstrated all its efficiency and effectiveness as a tool. Functionally, the study recruited 58 adult subjects who were permanently ostomized, and recruitment followed the inclusion and exclusion criteria, but there may be a selection bias related to the fact that the physical and mechanical characteristics of the ostomies were not taken into account; however, this bias was ruled out by the investigator who felt for this study not to consider these variables because the number of participants was too small to investigate this aspect in depth.
In the future, therefore, we will try to investigate the technical features even further, introducing in detail the issue of the validation process of the questionnaire used.
In conclusion, Perrotta-Guerrieri Psychological Care for Ostomy Patients" (PCOP) protocol and the integrated questionnaire (PCOP-Q1) can be considered tools that facilitate the process of acceptance of the adult ostomy patient on a definitive basis, helping the therapist to center the psychotherapeutic intervention strategically. However, these tools cannot be considered exclusive but rather must be complementary to the early educational and training intervention to be offered to the patient to help him or her in the difficult process of psychophysical healing.
This work received no external funding.
Ethics statement: All participants were assured of compliance with the ethical requirements of the Charter of Human Rights, the Declaration of Helsinki in its most up-to-date version, the Oviedo Convention, the guidelines of the National Bioethics Committee, the standards of "Good Clinical Practice" (GCP) in the most recent version, the national and international codes of ethics of reference, as well as the fundamental principles of state law and international laws according to the updated guidelines on observation studies and clinical trial studies.
Informed Consent Statement: Subjects who gave regular informed consent agreements were recruited; moreover, these subjects requested and obtained from GP, as the sole examiner and project manager, not to meet the other study collaborators, thus remaining completely anonymous.
Data Availability Statement: The subjects who participated in the study requested and obtained that GP be the sole examiner during the therapeutic sessions and that all other authors be aware of the participant's data in an exclusively anonymous form.
Acknowledgements: The author who contributed to the work is 1. The author has read and approved the final manuscript.
Conflicts of Interest: The authors declare no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
