
Research Article | DOI: https://doi.org/10.31579/2641-0419/511
1Faculty of medicine and pharmacy Marrakech
2Cardiology department. Avicenne Military Hospital
*Corresponding Author: Yassine Alfatihi, Faculty of medicine and pharmacy Marrakech
Citation: Yassine Alfatihi, Anas Zbitou, Hamid Jallal, Abdelmajid Bouzerda, (2025), Clinical and Angiographic Analysis of Thrombolyzed Patients: Observational Study in the Cardiology Department of Avicenne Military Hospital, Marrakech, J Clinical Cardiology and Cardiovascular Interventions, 8(13); DOI:10.31579/2641-0419/511
Copyright: © 2025, Yassine Alfatihi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 25 August 2025 | Accepted: 08 September 2025 | Published: 18 September 2025
Keywords: thrombolysis ; stemi: (st-elevation myocardial infarction); timi flow grade; cardiovascular risk factors; angiographic outcomes
This study provides a detailed description of the demographic, clinical, therapeutic, and angiographic characteristics of patients who received thrombolysis for ST-segment elevation myocardial infarction (STEMI). The analysis is based on a local prospective registry, with the aim of better understanding patient profiles and evaluating the effectiveness of this therapeutic strategy.
A clinical data registry was compiled between July 2024 and January 2025, including patients admitted with STEMI who underwent thrombolytic therapy. Collected data included sociodemographic characteristics, medical and cardiovascular history, clinical presentation on admission, time to treatment, thrombolysis modalities, angiographic findings, and potential complications.
The analysis highlights a predominance of cardiovascular risk factors, particularly smoking, hypertension, and diabetes. Clinically, the classical symptoms of myocardial infarction—chest pain, dyspnea, and sweating—were most frequently reported. Thrombolysis was administered in two main scenarios: as a primary strategy or as a rescue intervention, with variable success rates based on clinical and electrocardiographic criteria. Post-thrombolysis coronary angiography assessed lesion location and severity, arterial patency based on TIMI flow, and the need for complementary angioplasty.
This work sheds light on the local specificities of thrombolytic management of STEMI. The findings may help refine reperfusion strategies and adapt protocols according to patient profiles and organizational constraints.
Acute coronary syndromes (ACS), particularly ST-segment elevation myocardial infarction (STEMI), remain a major cause of cardiovascular mortality worldwide. Early reperfusion is the cornerstone of management, with primary percutaneous coronary intervention (PCI) considered the preferred strategy. However, in many regions where timely PCI is not feasible, thrombolysis remains a vital and accessible alternative.
The success of thrombolysis depends on patient characteristics, treatment delays, and healthcare resources. Local registries are essential to assess real-world outcomes and guide tailored strategies. This study analyzes a prospective registry of thrombolyzed STEMI patients at Avicenne Military Hospital, Marrakech, focusing on clinical profiles, angiographic results, and therapeutic effectiveness.
This was a descriptive observational study. Patients included were treated with thrombolysis between July 2024 and January 2025. Data collection focused on:
Data were analyzed descriptively.
A total of 30 patients were included.
Risk factors
Clinical findings
Additional investigations

Figure 1: Echocardiography showed reduced LVEF
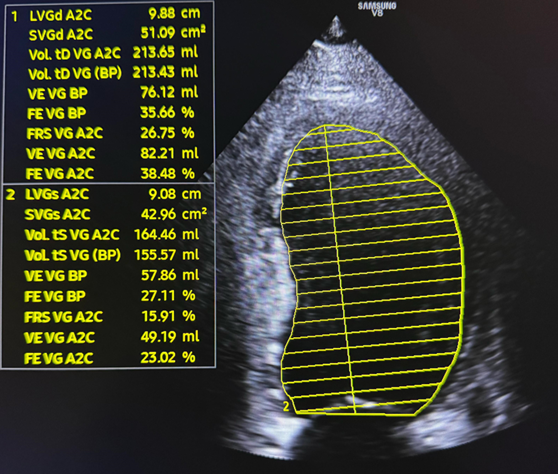
Figure 2: Echocardiography showed reduced LVEF
Therapeutic approach
Thrombolysis efficacy

Figure 3: ECG showing ST-segment elevation
The Role of Thrombolysis in Contemporary STEMI Management
The management of STEMI relies on rapid reperfusion to salvage myocardium and improve survival. The 2023 ESC guidelines and the 2021 AHA/ACC chest pain guidelines recommend primary percutaneous coronary intervention (PCI) as the treatment of choice when performed within 120 minutes of first medical contact [6,7]. However, fibrinolysis remains a validated and life-saving strategy in regions where access to PCI is limited or delayed, especially in rural or resource-limited healthcare systems. The CAPTIM trial demonstrated comparable outcomes between pre-hospital fibrinolysis and primary PCI when performed within 2 hours of symptom onset [4]. Our findings confirm that thrombolysis continues to play a pivotal role in our setting, functioning as an initial reperfusion strategy integrated into a pharmaco-invasive approach.
Predictors of Thrombolysis Success and Failure
Patient profiles and treatment delays strongly influence thrombolysis outcomes. Large registries, including FAST-MI (France) and GRACE (international), have demonstrated that older age, diabetes, hypertension, and renal dysfunction are associated with lower rates of successful reperfusion and higher mortality [8,9]. Similarly, the NRMI (National Registry of Myocardial Infarction, USA) highlighted the prognostic importance of early symptom recognition and prompt intervention [11]. In our series, the predominance of elderly patients with multiple cardiovascular risk factors likely explains the modest ST-segment resolution rates and frequent need for complementary PCI.
The symptom-to-needle time is another critical factor. Evidence from the CAPTIM and STREAM trials showed that fibrinolysis within 2–3 hours of symptom onset significantly increases the probability of achieving TIMI 3 flow and reduces 30-day mortality [4,10]. Conversely, delayed thrombolysis (>6 hours) has been associated with higher rates of mechanical complications and mortality, as confirmed by the landmark ISIS-2 trial [12]. In our registry, most patients were treated within acceptable time frames, likely contributing to the relatively high angiographic success rate (90%).
Comparison with International Registries
The angiographic results of our cohort are consistent with international data. We observed TIMI 3 flow in 60% of patients, similar to findings from the FAST-MI registry (55–65%) [8] and an Indian cohort reporting 37–60% [3]. The GUSTO-I trial, which included over 40,000 patients, reported TIMI 3 flow restoration in approximately 54% of fibrinolysis-treated patients [13]. These comparisons reinforce the external validity of our results, despite differences in healthcare infrastructure.
Pharmaco-Invasive Strategy and Its Benefits
Evidence supports a pharmaco-invasive strategy, in which fibrinolysis is followed by early PCI (2–24 hours) or rescue PCI if reperfusion is incomplete. The STREAM trial demonstrated that this approach reduces mortality, reinfarction, and heart failure compared with fibrinolysis alone [10]. The TRANSFER-AMI trial confirmed that routine early PCI following successful fibrinolysis significantly improves outcomes compared with standard conservative management [14]. In our cohort, all patients underwent coronary angiography, and secondary PCI was performed whenever indicated, consistent with these recommendations.
Prognostic Tools for Risk Stratification
Risk stratification is essential to guide therapy and optimize outcomes. The TIMI Risk Index, which incorporates age, blood pressure, and heart rate, has been validated as a predictor of early mortality [5]. The GRACE risk score, integrating additional variables (Killip class, creatinine, and troponins), has proven superior for predicting in-hospital and long-term outcomes [9]. Implementing these scores in daily practice could help identify high-risk patients requiring early transfer to PCI-capable centers and closer post-discharge monitoring.
Clinical Implications
This study has typical limitations of a local registry: small sample size, lack of long-term outcomes, and missing prognostic biomarkers. Multicenter studies would help validate these results.
Our findings highlight the clinical profiles, treatment modalities, and angiographic outcomes of thrombolyzed patients. These insights could help improve management strategies in resource-limited settings and serve as a foundation for future multicenter studies.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
