
Research Article | DOI: https://doi.org/10.31579/2578-8868/140
State Educational Institutional of Higher Professional Education” M. Gorky Donetsk National Medical University”, DCTMA, Donetsk.
*Corresponding Author: O.I. Lystratenko, State Educational Institutional of Higher Professional Education” M. Gorky Donetsk National Medical University”, DCTMA, Donetsk.
Citation: O.I. Lystratenko, A.M. Kardash, D.O. Lystratenko, V.P. Kardash. (2020) Clinical and Anatomical Rationale for the use of Fronto-Orbito-Zygomatic (foz) approach for the Surgical Treatment of Tumors of the Orbit and Cranioorbital Region. J. Neuroscience and Neurological Surgery. 7(1); DOI:10.31579/2578-8868/140
Copyright: © 2020 O.I. Lystratenko, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 10 October 2020 | Accepted: 17 October 2020 | Published: 23 October 2020
Keywords: orbital tumor; ptosis; fronto-orbito-zygomatic approach; subconjuctive approach; rhabdomyosarcoma.
The article discusses and analyzes the results of the treatment of 56 patients with tumors of the orbit, cranioorbital region, operated at the neurosurgery clinic DCTMA in Donetsk from 2015 to February 2020, with various surgical approaches.
Goals and objectives: coverage of clinical signs and symptoms, histology, diagnostic methods and treatment of patients operated on with tumors of the orbit and cranioorbital region for the period 2015-2020. The rationale for the use of front-orbit-zygomatic access as the optimal surgical access to tumors of the orbit and cranioorbital region of various localization, to perform radical organ-preserving surgery, with the maximum preservation of visual function, minimizing oculomotor disturbances, patient disability, good cosmetic effect in the postoperative period.
Materials and methods: we analyzed the clinical cases of 56 patients who underwent treatment in DCTMA with tumors of the orbit, cranioorbital region for the period from 2015 to March 2020.
Patients were operated on with different approaches - transcutaneous, subconjunctival, front-orbit-zygomatic, pterional, subfrontal. Surgical approaches were determined individually, depending on the location, size of the tumor, involvement in the process of the underlying structures of the orbit, adjacent anatomical areas (frontal, maxillary sinuses, cranial cavity, bones of the base of the skull). In 2 cases of lesions of the orbit by the tumor process a relapse of the tumor growth was obtained: one patient with aggressive adenocarcinoma, after 18 months, leading to orbital exenteration, and a 9-year-old child with rhabdomyosarcoma after non-radical removal of the tumor by subconjunctival approach. In all other cases, no relapses were noted; the operations were organ-preserving.
Conclusions: the results of treatment of patients with orbital tumors directly depend on the radical removal of the neoplasm, which is associated with the choice of surgical approach, the use of chemo-, radiation therapy in the postoperative period, depending on the histological response.
Advantages and versatility of FOZ - approach:
─ gives good visibility of all structures of the orbit, paraorbital regions, including the cranial region;
─ allows to perform organ-sparing operations to remove tumors of cranioorbital localization of any size;
─ provides radical removal of the neoplasm;
─ maximum preservation of vision function;
─ minimization of oculomotor disorders, patient disability;
─ good cosmetic effect.
Indications for front-orbit-zygomatic access:
─ large formations of orbit (more than 2.5-3 cm in diameter), with diffuse growth in the capsule, including a metastatic one;
─ osteomas of the walls of the orbit, meningiomas with intracranial, intraorbital growth, fibrous dysplasia of the bones of the skull base, causing compression of blood vessels and nerves, functional disorders of the eye;
─ tumors of the apical part of the orbit, including the optic nerve.
The disadvantages of the method are the technical complexity for ophthalmologist surgeons, by the routinism of the manipulation for neurosurgeon. In this regard, surgery of orbital tumors, cranioorbital localization, is subject to the competence of doctors of related specialties, including neurosurgeons.
Tumors of the orbit are a common pathology. Among all neoplasms of the organ of vision they account 23–25%. Almost all tumors observed in humans are found in orbita. The frequency of primary tumors is 94.5%, secondary and metastatic tumors occur in 5.5%.
As it turned out, their diagnosis is a big problem not only for the ophthalmologist. Due to the anatomical proximity of the orbit to the cranial cavities and paranasal sinuses tumors of the orbit are very diverse, as they can arise from different anatomical structures of the orbit. In this regard not only oculists, but also ENT- doctors, maxillofacial surgeons and neurosurgeons can be involved in the diagnosis establishing and delivery of the surgical care of patients with orbital tumors.
For the effectiveness of diagnosis, we have introduced and use the mandatory algorithm for examining a patient with suspecsion on orbital neoplasm, with individual characteristics for each patient:
─ ophthalmological examination, ophthalmoscopy;
─ X-ray of the orbit and skull;
─ Ultrasound of the orbit, as a screening study;
─ CT scan with intravenous contrast, MRI, to clarify the prevalence of the process;
─ examination of an ENT doctor, neurologist;
─ general clinical blood tests;
─ fine needle aspiration biopsy of tumor tissue and subsequent cytological, histological study of the obtained material.
In the article, we examined the results of the treatment of 56 patients operated on with tumors of the orbit, cranioorbital region, and performed the analyzing the surgical approaches depending on the location and nature of the process. We have identified and justified indications for FOZ – approach in case of neoplasms of this localization.
Materials and methods.
For the period from 2015 to March 2020 in Donetsk Neurosurgical Clinic we operated on 56 patients with tumors of the orbit of various localization and histostructure.
Among the patients, 15 men (26.8%) and 17 women (73.2%) aged 2 to 79 years. Among them, 10 (17.9%) children - 4 boys and 6 girls.
The main symptoms of orbit tumors are: unilateral ptosis, exophthalmos, diplopia, progressive decrease in vision in one eye, eye pain.
All patients were examined according to the above mentioned algorithm.
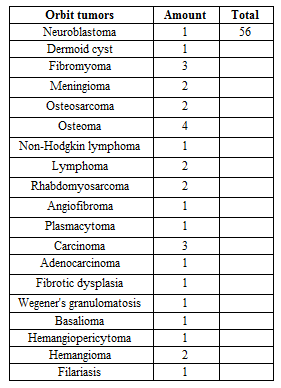
Table 1: According to histological analysis, we distributed the clinical cases.
Orbital tumors are various according location:
- associated with the apical part of the orbit;
- not associated with the apical part of the orbit;
- with intracranial growth,
- with growth in the paranasal sinuses.
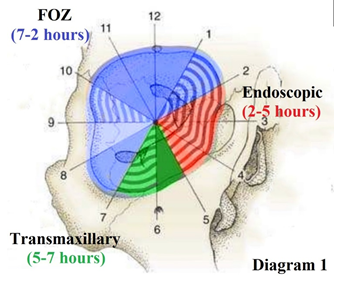
Diagram 1: Depending on the location of the tumor, different surgical approaches should be preferred, which is displayed in a pie chart
Optimal surgical approach should be minimally traumatic, as convenient as possible for visualization and manipulation, and contribute to achieving a high degree of radicalism, good functional outcomes and cosmetic results [5].
The principles of orbit microsurgery, until now, have not undergone significant changes and are actively used in modern cranioorbital approaches - supra-orbital, FOZ, lateral orbitotomy.
To remove an orbit tumor, cranioorbital localization, we pay special attention to organ-preserving operations using FOZ approach, which provides an optimal surgical access and minimizes damage to orbit structures.
Anatomical and topographic substantiation of FOZ approach (description):
1. Cosmetic skin incision along the edge of the scalp (Figure. 1).
2. To preserve the integrity of the anatomical structures, to prevent atrophy of the temporal muscle in the postoperative period, the muscle should be crossed 1.5 cm below its attachment to the bone with preservation of the muscle cuff. In the future, the muscle is stitched with a muscle cuff, which allows to restore its function, to avoid atrophy and consequently a cosmetic defect (Figure. 1).
3. Craniotomy is providing with 2 burr holes (BH), one of which is performed in a key point - at the junction of the alisphenoid and the zygomatic process of the frontal bone (Figure. 2).
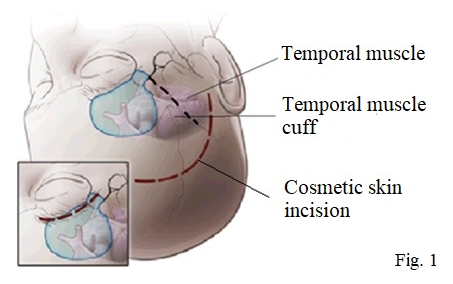
Figure 1: Cosmetic incisions of soft tissues by FOZ approach.
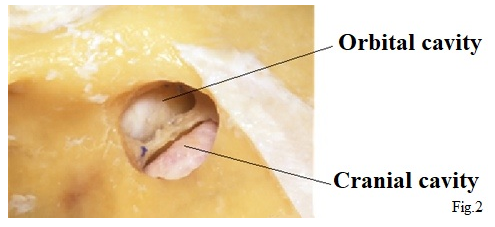
Figure 2: Burr hole in a key point.
The second - depending on the prevalence of the orbital process in the cranial cavity (to correct the size of the cranial part of the bone flap). The bone cut line was to the supraorbital foramen (for localization of tumors from 7 to 12 hours according to Diagram 1) or after the supraorbital foramen (for localization of tumors from 7 to 2 hours - marked by blue on the Diagram 1), including the apical part of the orbit, along the bone suture of zygomatic process. A fragment of a bone flap is freely removed, since the roof of the orbit is of very thin, is trepanning along the bone suture, within the anatomical borders (Figure. 3,4,5) [28].
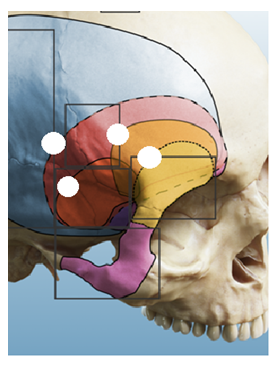
Figure 3: Sizes of the trepanation window of the cranial part.

Figure 4: Bone flap by FOZ approach.
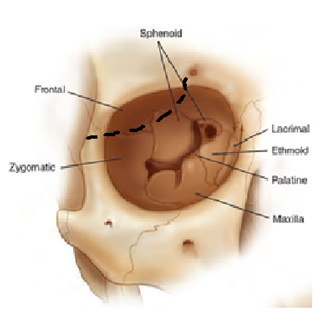
Figure 5: The seven constituent bones of the orbit: zygomatic, frontal, sphenoid, lacrimal, ethmoid, palatine, maxilla.
3. The bone window by such trepanation allows to examine all the structures of the orbit large enough to remove a tumor of the orbit of any location (from 1 to 7 hours, marked in blue in diagram 1) and sizes, with minimal damage to the structures of the orbit. (figure. 6,7). High radicalism with microsurgical removal of diffusely growing tumors is achieved using an ultrasonic aspirator, cold plasma, diathermocoagulation.
This approach allows to get the tumors in three different ways:
1) laterally through the space between the superior oblique muscle;
2) medially between the levator palpebrae superioris muscle and the superior rectus muscle;
3) laterally through the gap medially limited by the levator palpebrae superioris muscle, and the superior rectus muscle and the lateral rectus muscle.
The last of the three options was the most convenient and safe for approaching the optic nerve [27].
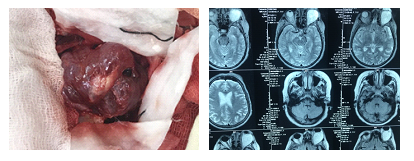
Figure 6: Bone window from which the tumor swells, next to the CT scan of this patient.
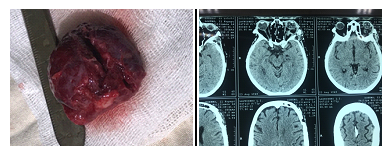
Figure 7: Remote tumor from the intermuscular funnel 4.0 x 4.5 x 4.0 cm, next to the patient’s CT scan after surgery.
4. After microsurgical removal of the orbit tumor, the bone flap is put on the place, fixed by two titanium bridges, without violating the anatomical integrity of the orbit. (Figure. 8.9) [28].
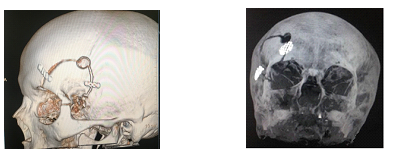
Figure 8 Fixation of the bone flap Figure. 9 Restored the integrity
with titanium bridges. of the orbit wall.
Subconjunctival approach by cantotomy. It is a less traumatic modern approach. It is used to remove tumors of the orbit in the lower medial, lower lateral surgical angles. This approach is not effective when the orbit tumors are located in the area of the intramuscular funnel, and can be used to remove hemangiomas, encapsulated neoplasms, less than 2.5 cm in size, and an open diffuse tumor biopsy. It does not quite meet all the requirements of modern oncology.
When it this refers to radical removal of the tumor with minimization of traction and damage to the structures of the orbit, leading to oculomotor disturbances, preservation of the organ of vision, one should resort to FOZ approach that meets all of above mentioned requirements.
FOZ approach in our opinion is the most ideal, universal for removing tumors of the orbit of various locations: the optic nerve canal, intermuscular funnel, lacrimal gland tumors, lateral, lower lateral orbit, osteoma of the orbit walls, meningiomas and diffuse orbit tumors of large sizes, including those spreading intracranially.
This approach is an alternative:
- 1. The technique of combined orbitotomy proposed by S. McCord in 1978.
The essence of a method consists in performing ordinary orbitotomy without dissecting of external periororbitis at the first stage. At the second stage, a conjunctival incision is made along the meridian of 9 or 3 hours, the medial rectus muscle is stitched with a ligature and cut off from the attachment site. For the remaining tendon of the medial rectus muscle the eye is fixed and displaced outwards. The absence of an outer wall allows to sharply take eye aside, which opens access to the top of the orbit.
- 2. Subconjunctival less traumatic approach is used to remove tumors of the orbit of the lower medial, lower lateral surgical angles. This approach is not effective when the orbit tumors are located in the area of the intramuscular funnel; it can be used to remove hemangiomas, encapsulated neoplasms, less than 2.0 cm in size, and open biopsy of the diffuse tumor.
Clinical case. The child is 2.5 years old.
In neurological status: ptosis, diplopia, pain syndrome, exophthalmos, visual impairment. Symptomatology increased in the above-noted order duaring 1 year. Patient was operated on with FOZ-approach. In the postoperative period - regression of the described symptoms. The histological response is hemangiopericytoma.
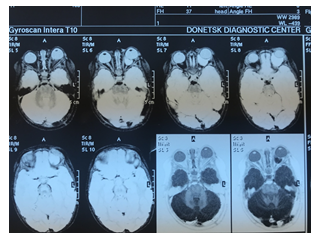
Figure 10: Tumor of the right orbit.
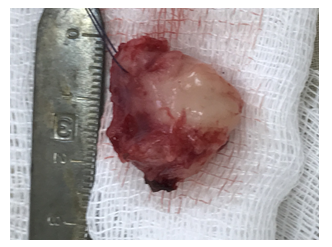
Figure 11: Remoted tumor node.
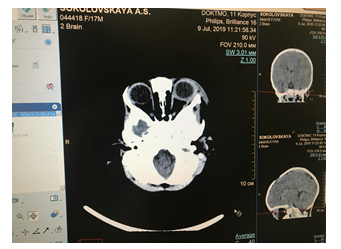
Figure 12: CT scan after surgery. The tumor was removed, compression of the optic nerve was eliminated, regression of exophthalmos.
1. Tumors of the orbit are common diseases. The main symptoms of the orbital tumors are - unilateral ptosis, exophthalmos, diplopia, pain syndrome, progressive visual impairment in one eye. With the exclusion of endocrine pathology, a diagnostic algorithm should be performed to identify or exclude the tumors:
- Ultrasound of the eye, as a screening study;
- CT with intravenous contrast, MRI, to clarify the prevalence of the process;
- ophthalmological examination, ENT specialist, neurologist.
2. The results of the treatment of patients with orbital tumors directly depend on the radicalism of the neoplasm removal, which is associated with the choice of surgical approach, the use of chemo-, radiation therapy in the postoperative period, depending on the histological response. In our opinion, the most universal method for removing orbital tumors of various localization and sizes is FOZ approach which provides the implementation of radical organ-preserving surgery, with the maximum preservation of visual function, minimizing oculomotor disturbances, and patient disability, despite its technical complexity for surgeons ophthalmologists. In this regard, surgery of orbital tumors and cranioorbital region is a subject to the competence not only ophthalmologists but also neurosurgeons.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
