
Case Report | DOI: https://doi.org/10.31579/2641-0427/025
1 Associate Professor in Orthopaedics, 2nd Orthopaedic Department Aristotle University of Thessaloniki, G. Gennimatas Hospital, Ethnikis Aminis 41, 54635, Thessaloniki, Greece.
2 Orthopaedic Surgeon, 2nd Orthopaedic Department Aristotle University of Thessaloniki, G. Gennimatas Hospital.
3 Professor in Orthopaedics, 1st Orthopaedic Department Aristotle University of Thessaloniki, G. Papanikolaou Hospital, Thessaloniki, Greece.
4 Professor in Orthopaedics, Chairman of the 2nd Orthopaedic Department Aristotle University of Thessaloniki, G. Gennimatas Hospital.
*Corresponding Author: Konstantinos Ditsios, Associate Professor in Orthopaedics, 2nd Orthopaedic Department Aristotle University of Thessaloniki, G. Gennimatas Hospital, Ethnikis Aminis 41, 54635, Thessaloniki, Greece.
Citation: Konstantinos Ditsios, Konstantinos Chitas, Triantafyllos Katsimentzas, Georgios Petsatodis and Pericles Papadopoulose (2021). Clavicular Chondrosarcoma: A Case Report. J. Orthopaedics and Surgical Sports Medicine, 4(1); DOI:10.31579/2641-0427/025
Copyright: © 2021 Konstantinos Ditsios, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 October 2021 | Accepted: 21 October 2021 | Published: 01 November 2021
Keywords: clavicle; chondrosarcoma; claviculectomy; reconstruction; osteosarcoma; pathological clavicular fracture; histologic diagnosis; vascularization
Background: Primary malignant tumors of the clavicle are very rare lesions, which may be easily misdiagnosed or even undiagnosed and not much can be found in literature about their treatment and prognosis. Among these lesions, chondrosarcomas percentage is considered 2%-8%, and due to their poor response to chemotherapy and radiotherapy, surgical excision with wide margins is the mainstay of treatment.
Case presentation: A 53-year-old man, with a large, painless mass on his left supraclavicular space was diagnosed with grade II clavicular chondrosarcoma after a needle biopsy. He was treated by surgical resection of the tumor with wide margins, and reconstruction of the deficit using a fibular autograft and a 3,5mm reconstruction plate. The result was excellent with adequate shoulder mobility and mild functional deficit of the upper extremity.
Conclusions: Primary malignant lesions of the clavicle are very rare and they often are misdiagnosed or even undiagnosed. Optimal treatment for these tumors is considered total or partial claviculectomy with satisfying functional and oncological outcomes.
Primary clavicular tumors are rare, consisting of less than 1% of all bone tumors [1,2]. Most of them are malignant and because of their rarity, there is low index of suspicion and often are underdiagnosed. The most common histologic diagnosis of clavicular tumors are myeloma, Ewing sarcoma, or osteosarcoma [14]. The literature pertaining to their diagnosis and treatment is poor, including, mostly, case reports and small case series [3]. Consequently, oncologists have limited experience in the management of these lesions and there are no standardized guidelines to follow. The main clinical symptoms are pain and local masses. Moreover, the pain will be more severe in the setting of a pathological clavicular fracture [15].
Among these lesions, chondrosarcomas percentage, has been reported in some studies, between 2% and 8% [4]. Chondrosarcomas comprise approximately one-third of all malignant bone tumors and 15% are located in the shoulder girdle [5]. They are more prevalent in adults than in children and more common in males and in people older than 40 years old. Their therapeutic outcomes differ by the clinical and histological grade, but their poor response to chemotherapy and radiation therapy lead to low 5-year survival rates. Surgical excision with wide margins is the mainstay of treatment for patients with localized disease [6]. Claviculectomy maintains a high incidence of surgical complications such as vascular injury, nerve damage and infections [21]. Although satisfying functional results have been reported after claviculectomy without reconstruction, many authors have suggested reconstruction with allograft or autograft, in order to restore the shape of the shoulder and protect the subclavian vessels and nerves [14, 21]. The aim of this article is to analyze the clinical and imaging features of a patient with a malignant clavicular tumor and to report the outcome of the surgical treatment. A brief review of the literature is also provided.
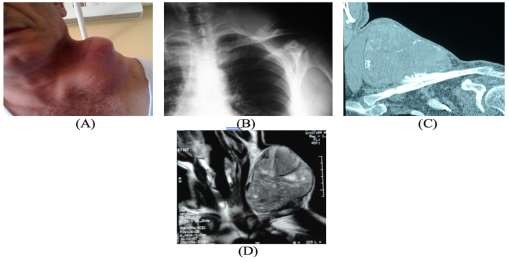
A 53-year-old male, with no significant medical history, was referred to the orthopedic department of our hospital due to a sizeable, painless mass (Figure 1-A) on his left supraclavicular space. According to the patient, this mass first appeared ten years ago and had been gradually growing ever since.
The main complaint of the patient was the rapid growth rate of the mass during the last few months. Clinical examination revealed elicitation of mild pain during shoulder movements. Neurovascular disruption was not recognized. Radiographic evaluation (Figure 1-B) showed a lesion with spotted calcifications arising from the middle third of the clavicle, disrupting the cortex of the bone and expanding to the surrounding soft tissues. Initial laboratory data, which included standard biochemical testing, C-reactive protein and erythrocyte sedimentation rate were within normal range. Due to the characteristics of the lesion further imaging examination was performed, which included enhanced CT (Figure 1-C) and MRI (Figure 1-D). The advanced imaging control helped us to define the size of the lesion, the disruption of the surrounding soft tissues and the relation with the neurovascular structures. From the clinical and imaging work-up a malignant bone tumor was suspected, hence the patient was subjected to CT-guided needle biopsy. Histological examination of the samples revealed a Grade II chondrosarcoma.
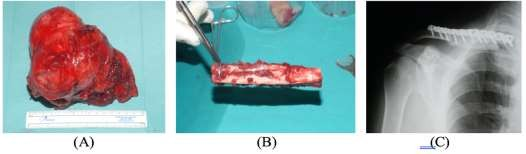
After the establishment of the diagnosis, staging of the disease was imperative in order to choose an appropriate treatment. Chest CT, upper and lower abdomen CT and bone scan revealed no metastatic disease. After a tumor board meeting, operative treatment was decided and we proceeded to wide marginal excision of the tumor (Figure 2-A). The bone deficit of the clavicle was restored using a non-vascularized fibular autograft (Figure 2-B) of approximately 13cm and was fixated with a 3,5mm reconstruction plate (Figure 2-C).
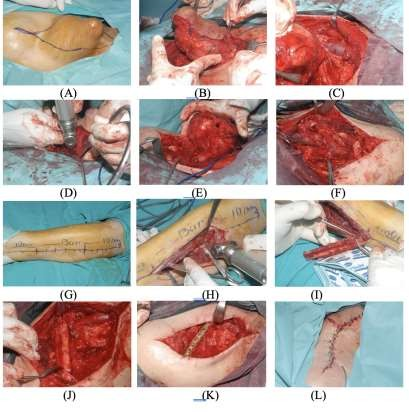
An illustrative surgical diagram is depicted in (Figure 3), (A-L). The histological analysis of the tumor concluded that it was a clear cell myoepithelial carcinoma. Chemotherapy and radiation therapy were not performed, as these types of treatment have poor effect on chondrosarcomas.
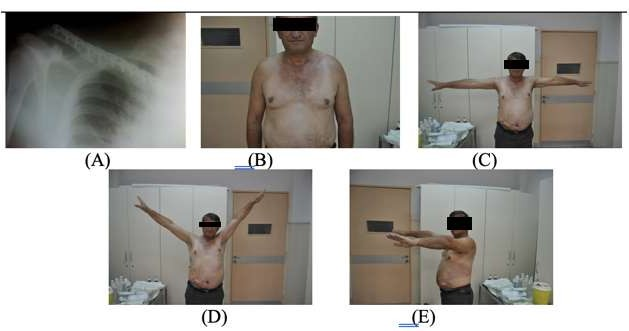
Post-operative rehabilitation was smooth and no complications were recognized, except from a superficial infection of the wound. At one year follow up there were no signs of the disease or major functional deficits of the upper extremity (Figure 4).
Clavicle is an unusual bone with distinctive characteristics. It is the first bone to ossify and the only long bone that lies on the horizontal axis. It ossifies through intramembranous ossification, from three ossification centers: two primary centers (a medial and a lateral) for the body and a secondary center for the sternal end. It lacks a medullary cavity and it has poor vascularization [3,4]. According to these characteristics, clavicle is considered more of a flat bone rather than a long one, and thus, it is an uncommon site for malignant tumors [3,4].
Primary clavicular tumors and tumorous lesions are uncommon. The incidence of these tumors is between 0,45% and 1,1% of all bone tumors and it is the forth site for tumor appearance in thoracic skeleton [3,4]. A review of primary shoulder tumors (194 cases), published by Cleeman et al, showed that clavicle was affected only in 6% of the cases [7]. In most cases, these lesions are more likely to be malignant than benign.
Chondrosarcomas are malignant cartilage-forming tumors, which occur mainly in pelvis, femur, humerus and scapula [1]. There are various subtypes of chondrosarcomas, each with different histopathology and clinical behavior. Most of them are conventional central (75%) and conventional peripheral (10%), while other types include periosteal (1% of all CS), dedifferentiated (10% of all CS), mesenchymal (<2>
Clavicle is less likely to be the origin of chondrosarcoma [9]. A review of primary clavicular tumors (206 cases), published by Ren et al, reported that the incidence of chondrosarcoma was approximately 5% [4]. The literature pertaining to their treatment is poor, limited only in case reports and small case series, and as a result, standard guidelines have not been established. A small review of current bibliography has shown that surgical resection is commonly accepted in these cases as the optimal treatment, but it has not been clarified whether the reconstruction or not of the bone deficit has a significant impact on the functional and oncological outcome. Nota et al, in their study, reported excellent functional results after partial scapulectomy or claviculectomy, in 20 cases of primary chondrosarcoma [10]. In an another retrospective review, Li et al reported very good functional results after total claviculectomy in 9 cases with primary malignancy [11]. Similar oncological and functional results have been reported by Krishnan et al [12] and Radhakrishnan et al [13] in their studies, regarding partial or total claviculectomy in cases of malignancy. Rossi et al, studying six cases of clavicular malignant tumors, also advocate partial or complete cleidectomy, reporting adequate functional results [3]. In another perspective, Li et al proved that there was no advantage of allograft reconstruction over no reconstruction in terms of functional outcome, comparing two group of patients that were submitted to total or subtotal claviculectomy with or without allograft reconstruction [14]. Furthermore, Liu et al, in another retrospective review including 20 patients, concluded that reconstruction of clavicle defect after excision of a malignant tumor is not recommended [15]. Although good results after claviculectomy without reconstruction have been reported others suggest reconstruction using allografts and vascularized or non-vascularized autografts [16–19]. There are even reports of using bone cement prostheses or other novel prostheses in order to maintain the shoulder contour and functionality, with satisfying results [20,21]. In our case, partial cleidectomy was performed followed by reconstruction using a fibular autograft. The final outcome was excellent and we agree with other authors that clavicle reconstruction is advisable in order to preserve the functions of the upper extremity and protect neighboring neurovascular structures [8].
Clavicular malignant tumors are rare lesions with poor prognosis. Due to their infrequency, there is low index of suspicion and often these lesions are misdiagnosed. Resection and reconstruction procedures can be performed for local tumor control, pain control and good functional outcomes. Amputation and disarticulation can also be performed in rare cases. Current literature reports same functional outcomes after claviculectomy, with vs without reconstruction. This case report confirmed that partial claviculectomy with reconstruction, using a non-vascularized fibula autograft, offers good oncological outcomes without major functional deficits of the upper extremity.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
