
Research Article | DOI: https://doi.org/10.31579/2692-9406/095
1 Hematology and Blood Transfusion Department, Federal Teaching Hospital, Ido-Ekiti, Nigeria.
2 Department of Medical Laboratory Science, University of Benin, Benin City, Nigeria.
3 Department of Medical Laboratory Science, Afe Babalola University, Ado-Ekiti, Nigeria.
4 Hematology and Blood Transfusion Department, Federal Medical Centre, Owo, Nigeria.5 Department of Medical Laboratory Science, Achievers University, Owo, Nigeria.
*Corresponding Author: Esan Ayodele Jacob, Hematology and Blood Transfusion Department, Federal Teaching Hospital, Ido-Ekiti, Nigeria.
Citation: Esan A Jacob, E. O. Osime, Ogunbusuyi B Esther, O Kelvin, Oyedele E Titilayo. (2022). Classification of Absolute Cd4+ T Lymphocytes Count in Immunological, Virological and Erythropoietic Growth Factor among HIV Infected Patients. Biomedical Research and Clinical Reviews. 6(2); DOI: 10.31579/2692-9406/095
Copyright: © 2022 Esan Ayodele Jacob, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 October 2021 | Accepted: 31 December 2021 | Published: 19 January 2022
Keywords: immunological; virological; erythropoietin; hiv-infected; art/art-naïve
Background: HIV-infection resulted in CD4+ T-cell depletion which is accompanied by an increase in CD8+ T-cells resulting in an inverted CD4/CD8 ratio. Low CD4/CD8 ratio has been identified as a hallmark of inmmunosenescence and a surrogate of mortality in HIV infected patients especially in ART-naïve patients
Aim: Classification of absolute CD4+ T-lymphocytes count in immunological, virological and erythropoietic growth factor among HIV infected patients
Methodology: One hundred samples each was collected from HIV positive subjects on ART and HIV positive subjects ART naïve. Six milliliters of whole blood was collected from each consented subject, 3ml was dispensed into 5ml K2EDTA bottle for immediate analysis of absolute CD4 count, CD8 count, total white cell count and HIV screening. The remaining 3ml of blood was dispensed into plain bottle; serum was extracted for the analysis of erythropoietin and viral load
Results: Mean values of CD8, CD4/CD8, EPO and TWBC in CD4 <200 were significantly (p<0.05) lower compared to CD4 >500 and CD4 200-499. Mean values of VL in CD4 <200 were significantly (p<0.05) higher compared to CD4 >500 and CD4 200-499 among HIV subjects on ART and ART-naïve
Conclusion: Immunological and erythropoetic growth factor assessed in this study were decline while viral load was increasing as HIV infection progresses with depletion in absolute CD4 count, this study shows the efficacy of ART on the treated subjects. However, based on this study, absolute CD8 T cells count, CD4/CD8 ratio and erythropoietin can be used as surrogate makers to ascertain pathogenesis in HIV-infected subjects.
EPO= Erythropoietin,
VL= Viral load,
CD4= Cluster of differentiation 4,
CD8= Cluster of differentiation 8,
TWBC= Total white
Human immunodeficiency virus (HIV) infection is characterized by gradual CD4 depletion, CD8 expansion, and immune activation. Acute HIV infection causes initial activation and robust expansion of CD8 T cells (Mudd and Lederman, 2014). CD4+ T lymphocytes are helper lymphocytes, they excrete cytokines that can activate other immune cells. CD8 lymphocytes are cytotoxic, they directly destroy virus-infected cells and remain inactivated when there is no foreign antigen. During the course of illness among patients with human immunodeficiency virus (HIV) infection, CD4+ T-cell counts and viral load are traditionally monitored in order to assess response to therapeutic intervention. However, CD8+ T-cell counts may predict prognosis independently of CD4+ T-cell counts, overstimulation of CD8 response and its elevated count has been associated with accelerated HIV disease progression. Following successful antiretroviral therapy (ART), CD4 counts tend to remain above 200 cells/m3 in almost 99.2% of patients (Gale et al., 2013). Despite the successful restoration of CD4 counts and HIV suppression following ART, immune activation tends to persist, and CD8 counts seldom normalize (Helleberg et al., 2015). There is an emerging consensus that persistent immune activation and inflammation are due to residual HIV replication and microbial translocation that contributes to CD8 expansion (Cassol et al., 2010). CD4/CD8 ratio is a characteristic feature of HIV infection. ART restore the CD4/CD8 ratio, but the ratio rarely exceeds one, particularly in the event of delayed therapeutic intervention (Serrano-Villar et al., 2014). Failure to achieve normalization of the CD4/CD8 ratio has been attributed to persistence of high CD8 T-cell counts. This persistently low CD4/CD8 ratio has been demonstrated to reflect persistent innate and adaptive immune activation in HIV-infected patients. Moreover, it has recently been shown that a low CD4/CD8 ratio inversely correlates with the risk of morbidity and mortality, monitoring CD4/CD8 ratio in patients receiving ART may be useful to identify a subset of patients at much higher risk of non AIDS-defining cancer who may thus require a more intensive strategy of prevention or screening (Hema et al., 2016). It has been reported there is low level of erythropoietin (EPO) response in HIV infection which is secondary to the elevation of immunosuppression and inflammation, this suggested that HIV suppresses the production of erythropoietin (Esan et al., 2020; Gatukui et al., 2014). The aim of this study was to classified absolute CD4+ T lymphocytes count in immunological, virological and erythropoietic growth factor among HIV infected patients.
Study Design
This study was carried out at Federal Teaching Hospital, Ido Ekiti, Nigeria. One hundred samples each was collected from HIV positive subjects on ART and HIV positive subjects ART naïve. Each of these groups was classified into three stages of HIV infection using their CD4 values according to Centers for Disease Control as follows: Stage-1 CD4 ≥ 500 cells/uL, Stage-2: CD4 200 – 499 cells/uL and Stage-3: CD4 lessthen 200 cells/uL. Consented subjects were re-screened for HIV infection for the purpose of the study to confirm their HIV status using serial algorithm method. Patient’s consent was sort for through an informed consent form and ethical approval was obtained from Federal Teaching Hospital, Ido-Ekiti.
SAMPLE COLLECTION AND SAMPLE PREPARATION
Six milliliters (6ml) of whole blood was collected from each consented subject, 3ml was dispensed into 5ml K2EDTA bottle for immediate analysis of absolute CD4 count, CD8 count, total white cell count and HIV screening. The remaining 3ml of blood was dispensed into plain bottle, allowed to clot and centrifuged at 2500 revolution per minute for 5minutes to extract the serum into another plain bottles, stored at -400C for the analysis of erythropoietin and viral load
Methodology
Hiv Screening Test
Human immunodeficiency virus was diagnosed using serial algorithm method. Determine HIV-1/2 (Abbott Diagnostic Division, Belgium/Luxemburg), Uni-Gold HIV Kit (Trinity Biotech, Wicklow Bay, Ireland) and Chembio HIV ½ Stat-PakTM Assay. Patients reactive to antibody screening tests were considered positive and recruited into the study; the test was carried out according to the manufacturer’s instruction.
Analysis of CD4 and CD8 Count Using Flow Cytometry (Cyflow Counter)
Research samples for CD4 and CD8 count was prepared and run on the Partec cyflow counter (Partec flow cytometer, GMBH, Munster, Germany) according to the manual instructions.
Total White Blood Cell Count Haematology Analyzer
Total white blood cell count was analyzed using Haematology Analyzer (Sysmex XN 350 five parts) following Manufacture’s instruction.
Viral Load Analysis
Extracted plasma from K2EDTA sample was used to estimate HIV-RNA viral load analysis using polymerase chain reaction (PCR), the procedure was follow as describe in the manual.
Erythropoietin
Erythropoietin (EPO) was estimated using enzyme-linked immunosorbent assay (ELISA) kit, the procedure was followed as described in the manual ALPCO (2018).
Table 1
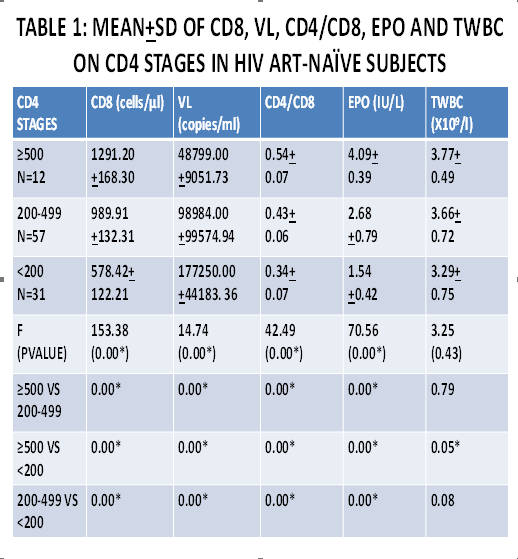
Table 2
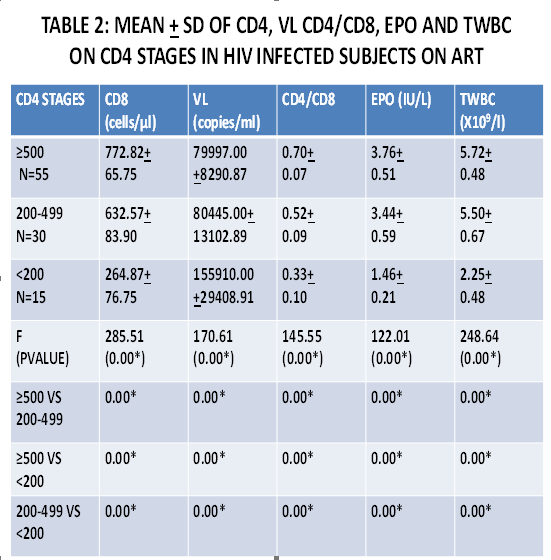
This study has revealed a significant high CD8 T-cell count in ART-naïve compared to subjects on ART in all the CD4 stages. However, mean value of CD8 in CD4>500 was higher compared with CD4200-499 and CD4 <200>500 in both ART and ART-naïve, this indicates that a higher occurrence of leucopenia with progression of HIV disease. Similar to this study Parinitha and Kulkarni reported that total white blood cell count showed significant difference between three groups with differing CD4 cell counts stages (Parinitha and Kulkarni, 2012). Supporting the findings in this study, it was reported that elevated white blood cell count typically means that body system is actively fighting an infection and low white blood cell count suggests that some disorder, either HIV-related or non-HIV-related, is affecting the bone marrow’s ability to produce white blood cells, indicating that the body system is less able to fight infection this showed that there is a correlation between CD4 count and total white blood cell. This present study revealed correlation between different stages of CD4 count and erythropoietin (EPO) among the study population. In supporting the findings in this study, Okafor reported that HIV has direct effect on the bone marrow through the expression of pro-inflammatory cytokines that suppress erythropoiesis (Okafor et al., 2019). Anaemia in HIV patients is caused by depressed bone marrow function by HIV infection leading to low production of erythropoietin which resulted into ineffective production of red blood cell (Esan et al., 2020), CD4>500 has higher mean value of EPO compared to CD4 200-499 and CD4<200>500 was higher compared to CD4 200-499 and CD4<200>hen viral load is low, CD4 counts will be high, this suggested that HIV viral load predicts how fast the disease will progress, while CD4 count, indicate how much damage the virus has already caused to immune system (Mocroft et al., 2010), The decline in CD4 count is linked to HIV viral load and is used as a measure of disease progression, the higher the HIV viral load, the faster the CD4 cell count will fall as we observed in this present study.
Immunological and erythropoietic growth factor assessed in this study were decline while viral load was increasing as HIV infection progresses with depletion in absolute CD4 count, this study shows the efficacy of ART on the treated subjects. However, based on this study, absolute CD8 T cells count, CD4/CD8 ratio and erythropoietin (EPO) can be used as surrogate makers to ascertain pathogenesis in HIV infected subjects because viral load cannot separately determine the rate of HIV progression to AIDS.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
