
Research Article | DOI: https://doi.org/10.31579/2641-0419/039
1* Doctor of Medicine. Professor in Internal Medicine. Hermanos Ameijeiras Hospital. Havana. Cuba.
2 Doctor of Medicine. Specialist in Internal Medicine. Hermanos Ameijeiras Hospital. Havana. Cuba.
3 Doctor of Medicine. Specialist in Biostatistics. Hermanos Ameijeiras Hospital. Havana. Cuba.
1 Doctor of Medicine. Professor in Internal Medicine. Hermanos Ameijeiras Hospital. Havana. Cuba.
4 Doctor of Medicine. Resident of Cardiology. Hermanos Ameijeiras Hospital. Havana. Cuba.
*Corresponding Author: Jorge Luis León Alvarez, Hospital Ameijeiras. Address: San Lázaro 701, between Marques González and Belascoaín. Centro Habana, Habana. Cuba. ZIP: 10300. Phone: + 53-78761000. Fax: + 53-78735036.
Citation: León Alvarez JL., Michel C. López., Tania H. Costa., Yanes Quesada MA., Calderín Bouza RO., Yao Dzebu AS. (2020) Circadian Blood Pressure Variability in Hypertensive Patients with Coronary Heart Disease. J Clinical Cardiology and Cardiovascular Interventions, 3(2); DOI:10.31579/2641-0419/039
Copyright: © 2020 Jorge Luis León Alvarez. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 December 2019 | Accepted: 26 December 2019 | Published: 03 January 2020
Keywords: hypertension; ambulatory blood pressure monitoring; coronary heart disease; myocardial infarction; heart failure; dipper pattern; non dipper pattern; morning surge; riser
Introduction and objectives: Coronary heart disease is one of the complications of hypertension. Ambulatory blood pressure monitoring allows studying the different circadian patterns of blood pressure, but there is not enough evidence linking coronary heart disease with different circadian patterns. This research was carried out with the purpose of characterizing the circadian patterns of blood pressure in patients with essential hypertension and coronary heart disease.
Methods: Descriptive and transversal research in 68 hypertensive patients with coronary heart disease who underwent ambulatory blood pressure monitoring. The different circadian patterns of blood pressure were related to the different forms of coronary heart disease and to the control of blood pressure.
Results: In the sample, women (60.3%) predominated over men (39.7%). The ages were between 45 to 59 (63.3%) and those 60 and over (36.7%). 44.1% did not have their blood pressure under control, 45.6% were overweight and 38.2% were obese. The abnormal patterns were dipper 42.6%, non-dipper 41.2%, extreme dipper 7.4% and riser 8.8%. Morning surge was observed in 29 patients (42.6%), statistically significant in relation to the control of blood pressure (p = 0.033), but not with the different types of coronary heart disease studied.
Conclusions: A statistically significant relationship was found between morning surge and control of blood pressure.
Hypertension is a global health problem. Between 30 and 50% of the adult population in most countries suffer from hypertension. [1-3]. In Cuba, it was estimated that 30.9% of people 15 years of age or older suffer from hypertension according to the III National Survey of risk factors and preventive activities of non-communicable diseases carried out in 2010-2011 [4]. Hypertension is an important risk factor for cardiovascular and renal diseases. It´s closely related to the leading causes of death in Western countries and is considered as a globally rising tracer disease, intended to control largely decreases of morbidity and mortality in the adult population [5, 6]. Recent data shows that untreated hypertension shortens life expectancy by approximately 5 years [7]. On the other hand, more than 70% of hypertensive patients have other cardiovascular risk factors (CRF). In fact, cardiovascular complications of hypertension are more frequent in the presence of other CRF, so hypertension should be considered as another component of the Cardiovascular Risk (CR) of the subject [8].
Hypertension causes complications or injuries to target organ damage (TOD) such as brain, heart, eyes, kidney and blood vessels, which are life-threatening if the abnormally high blood pressure (BP) figures are not corrected [9-12]. Lesions produced specifically in the heart because left ventricular hypertrophy (LVH), coronary heart disease and heart failure (HF) [13, 14]. There is a close association between hypertension and coronary heart disease [15-17]. Patients with hypertension are exposed to a much higher risk of developing any type of occlusive vascular disease, including coronary heart disease. This can limit myocardial perfusion and, consequently, the oxygen supply. The demand for myocardial oxygen is increased for two reasons: first, because of the increase in the output impedance to the left ventricular ejection and, secondly, because hypertension can produce LVH. This combination of decreased oxygen supply and/or increased demand for it is particularly harmful and explains the reason why hypertensive patients are more likely than normotensive patients to suffer from angina pectoris, myocardial infarction (MI) or other coronary episodes, and are exposed to an increased risk of death from coronary heart disease [11-14]. On the other hand, atherosclerosis is the main pathophysiological and pathological basis of coronary heart disease and is usually the result of a set of CRF, among which hypertension stands out for its importance [17-19].
The determination of BP continues to be one of the most important clinical measures in everyday medical practice. The BP follows a circadian pattern, with higher BP levels occurring during the day and lower values at night. In many hypertensive patients, there is no nocturnal decrease in BP (non-dipper pattern). This non-dipper pattern has been associated with a worse cardiovascular prognosis [20]. Therefore, in addition to the objective of reducing BP, we should consider knowing and modifying the patient's circadian pattern of BP [21-25].
Ambulatory Blood Pressure Monitoring (ABPM) is currently a useful tool in the diagnosis and monitoring of hypertension, although it is not considered a routine technique in the study of hypertension. The ABPM shows the existence of a sleep-wake pattern, with higher BP levels during wakefulness, especially in relation to physical activities or stressful situations, and lower figures during sleep. It has been observed how BP figures during wakefulness as measured by ABPM are similar to that of BP taken in the office. There is no clear consensus regarding normal reference values for ABPM [26-29].
Alterations of the circadian pattern of BP have been associated with coronary heart disease, a higher prevalence of ventricular arrhythmias and a high morbidity and mortality due to cardiovascular diseases; even in the accentuated dipper pattern, coronary heart disease can occur due to organ perfusion disorders, which may not only be a mechanism of vascular injury, but also a condition associated in patients with a worse prognosis. Therefore, the conversion of circadian patterns that are related to a higher CR according to the physiological circadian pattern is of vital importance and therefore constitutes an objective in the therapy of patient´s with hypertension and provides an adequate decrease in night averages obtained in relation to the averages achieved during the diurnal cycle [29, 30].
There is strong evidence that a persistent pattern of the absence of nocturnal descent is associated with a more pronounced cardiac involvement [31]. Several studies have consistently verified that MI has a higher prevalence between 6 am and 12 noon, than at other times during the day or night [32-35] .Data from prospective and population-based clinical studies show that ambulatory BP predicts the risk of cardiovascular events after adjustment in relation to conventional BP (assessed in the office) [36]. A classic prospective study, carried out by Perloff et al [37]. Established that the CR was higher in patients with higher values of ambulatory daytime BP than in those in which they were lower, independent of the levels of the BP measured in office. It has been found that outpatient BP is superior in predicting adverse cardiovascular clinical events when compared to conventional office BP measurements. In two studies, the prognostic value of ambulatory BP in the general population was considered [38, 39]. In both studies, after the adjustment for sex, age, smoking habit, initial office BP and antihypertensive treatment, ambulatory BP proved to be a better predictor of cardiovascular death than office BP [14-40]. On the other hand, nocturnal BP and ambulatory SBP were the best predictors of cardiovascular death. Similar results were also observed in the Dublin Outcome Study, carried out among 5,000 patients for 5 years [41]. However, the relationship between the coronary heart disease and the different circadian patterns of BP is not yet fully understood. In addition, the current accepted BP figures for the dipper status would not necessarily have to represent a normal nocturnal circadian profile [32-42]. Despite the accumulated evidence, the relationship between the presence of coronary heart disease in the hypertensive patient and the various circadian patterns of BP, in relation to the type of coronary heart disease and the control of the SP remains uncertain [43-47]. Motivated by characterizing in essential hypertensive patients with coronary heart disease how the different circadian patterns of BP behave in relation to the control of their BP and the type of coronary heart disease is why we conducted this research at “Hermanos Ameijeiras” Hospital.
A cross-sectional descriptive investigation was carried out between October 1, 2017 and September 30, 2018 at “Hermanos Ameijeiras” Hospital located in Havana, Cuba. The sample consisted of 68 patients of both sexes, 18 years old and older, who were attended in the hospital's hypertension offices, with the characteristic of being patients with essential hypertension, previously diagnosed with coronary heart disease, being treated or not, with typical or atypical symptoms of coronary disease, with diagnostic coronary angiography of coronary heart disease performed prior to the investigation. The following clinical forms coronary heart disease were considered: myocardial infarction (more than 3 months since it´s appearance), chronic stable angina pectoris, recovered sudden cardiac arrest and other forms of presentation of coronary heart disease: heart failure, arrhythmias and conduction disorders. Patients with diabetes mellitus or with other endocrinopathies, with severe acute or chronic diseases, pregnant women and patients with malformations that prevented the measurement of BP were excluded.
For all patients, following the acquisition of informed consent, the following data were collected by anamnesis: age, sex and BP, and were recorded on the data collection form (it was considered controlled if SBP/DSP <140/90 and uncontrolled if SBP/DBP ≥ 140/90) and body mass index (BMI) per the Quetelet formula [48].
In addition, ABPM was performed using the HIPERMAX equipment according to the hospital protocol and was classified as dipper, non-dipper, extreme dipper, riser, morning surge and nocturnal hypertension [49-54].
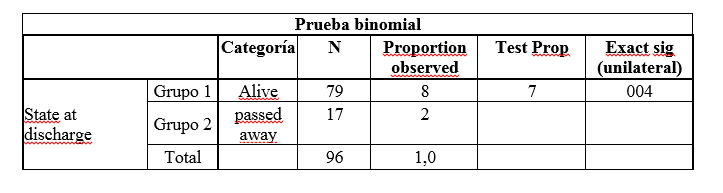
The information obtained was fed into a digital database and statistical processing was performed with the SPSS program version 20.0 (SPSS, Inc.; Chicago, Illinois, United States). Summary measures were used according to the type of variable that was analyzed. For the variable age: mean, standard deviation, minimum value and maximum value were calculated. For the variables sex, type of coronary heart disease, BMI and circadian patterns of BP: absolute numbers and percentages were calculated. For the search for association between the circadian patterns of BP with respect to BP control and the type of coronary heart disease, the Pearson Square Chi test (X2) or Fisher's exact test was performed on 2x2 tables that had presented 20 % or more of the cells with absolute numbers with values less than or equal to 5. In all the hypothesis tests a level of significance was set α = 0.05. The information was presented in statistical tables made using Microsoft Word text editor for Windows 10.
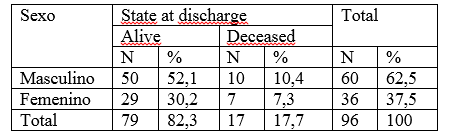
Table 1 shows the behavior of the different clinical variables in the patients studied (n = 68). 60.3% were females and 39.7% were males.
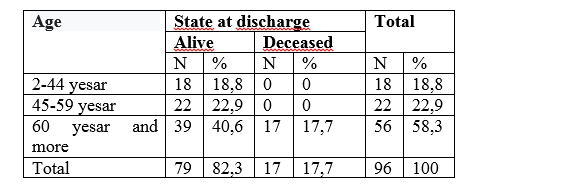
All the patients studied were over 45 years old, 63.3% being predominantly between 45 and 59 years old. Regarding BP control, 55.9% were controlled and 44.1% were not. Overweight and obesity were very striking characteristics in our patients, with 45.6% and 38.2% respectively. In addition, we observed the distribution of the different types of heart disease found in our patients, with angina pectoris being the most frequent with 61.8%, followed by heart failure with 23.5% and MI with 147%. Additionally, we observed the distribution of the different circadian BP patterns found in the patients studied. The dipper pattern considered the physiological pattern was present in 42.6%. According to the abnormal patterns (non-dipper, extreme dipper and riser) we highlight that 41.2% had a non-dipper pattern, among patients with an abnormal circadian pattern of BP (n = 39). We found that 42.6% had a morning surge pattern and we did not find patients with nocturnal hypertension.
Table 2 reveals the relationship between the different circadian patterns of BP and the control of BP. Although the dipper pattern predominated in patients with BP control with 47.4% and the non-dipper pattern in the uncontrolled patients with 43.3%, this difference was not statistically significant.
In the morning surge pattern found in 29 patients who had an abnormal circadian pattern of BP, 56.7% had no BP control and this was a statistically significant difference (p = 0.033).
Table 3 shows the relationship between the different circadian patterns of BP and the morning surge pattern, observing that there was no statistically significant relationship with any of the circadian patterns, although we found it more frequent in the non-dipper pattern with 41.4%.
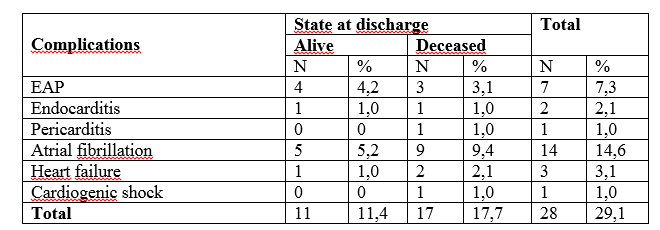
Table 4 shows the relationship between the different circadian patterns of BP and patients with chronic stable angina pectoris showing 47.6% who had a non-dipper pattern. In addition, the morning surge pattern was present in 40.5%, although both results had no significant difference. This table highlights that the dipper pattern independently, whether or not angina pectoris was present showed significant results of 42.6% (p = 0.048).

Table 6 shows the relationship between BPP circadian patterns and the presence of heart failure (n = 16). Both dipper and non-dipper patterns showed the same results with 43.5% and the morning surge pattern was 37.5% although without statistical significance.
Knowledge about hypertension has been increased by the contribution of ABPM [55-58]. Thus, for example, the concept of BP variability and its importance as a predictor of morbidity and TOD have been conclusively established [51-53]. The results obtained in this work are valid for this sample and are not intended to be extrapolated to other populations. ABPM has introduced a considerable change in the diagnosis and treatment of hypertension, shifting the interest from random measurement of BP to the BP that patients present in their usual environment. This has allowed us to avoid the phenomenon of white coat hypertension, confirm the diagnosis of hypertension, detect masked hypertension, assess the response to treatment and study the variability, etc [54-60].
One of the aspects that has required more attention in recent years has been the assessment of the circadian pattern of BP in sleep-wake cycles. Thus, some studies have shown that the absence of nocturnal decrease in BP is associated with a worse cardiovascular prognosis and TOD, both in hypertensive patients and in the general population, and it has been shown that the decrease in nighttime SBP is associated with a lower risk of cardiovascular events compared to subjects who do not experience such physiological decline [61-64]. It is known that there is an inverse correlation of BP in sleep and cardiovascular events in relation to the prognosis linked to this variable, which normal value is a reduction between 10 to 20% of BP during sleep in relation to wakefulness, even in the presence of normal average BP values obtained by ABPM [40, 42, 65, 66].
In this sample the difference in the distribution by sex of the patients was not significant, if we had a predominance in the ages above 45 years. Which think is because hypertension in its natural course during many years has little clinical expression and the appearance of TOD such as LVH in these patients is an expression of structural changes at the level of the vascular endothelium and the heart, which takes years to establish. A high frequency of uncontrolled BP was found (44.1%), which we consider to be one of the most important factors that favors the onset of TOD and in specific coronary heart disease.
The results of this research showed a circadian profile in 57.4% of the studied subjects that did not show an adequate reduction in BP at night or at rest. These results are related to those reported by other authors [51, 52, 53] .
Multiple pathophysiological abnormalities in essential hypertension could explain the abnormal pattern of BP decrease during sleep associated with coronary heart disease, since it is considered that the non-decrease of nocturnal decrease in BP is a consequence of alterations in the activation of the sympathetic nervous system, stimulation of the renin angiotensin system, insulin resistance and induction of the proliferation of smooth muscle cells in the blood vessels, which can cause alterations in the structure and function of the arteries. This occurs by several mechanisms. Firstly, insulin stimulates the production of nitric oxide by the endothelial cell producing a decrease in peripheral vascular resistance and a decrease in BP. It also inhibits the formation of migration-dependent lesions and the proliferation of vascular smooth muscles and decreases vasoconstriction mediated by the sympathetic nervous system. For this reason, an increase in resistance to insulin uptake by the endothelial cell has an inverse effect on these vasomodulatory mechanisms while the resulting hyperinsulinemia increases the vasoconstrictor vascular response by stimulating the sympathetic nervous system. This hyperinsulinemia could explain the adequate non-decrease in BP during sleep, highlighting the non-dipper and reverse dipper effect in these patients [66-70]. Another very important factor is the activation or inhibition of the anti-aging gene related with the different circadian patterns of BP and the coronary heart disease [71-73].
Recently, known dipper and non-dipper patterns have given attention to two additional behaviors that may coexist with abnormal circadian patterns such as nocturnal hypertension and morning surge conditions that have been described in a varied spectrum of situations that include sleep apnea and TOD [74]. and more importantly the increased risk of fatal and non-fatal cardiovascular events75 and their proven occurrence in the first hours of waking and during the day [76,77]. On the other hand, the relationship between coronary heart disease and the different circadian patterns of abnormal BP is strongly demonstrated [78, 79]. but not with the morning surge nor with nocturnal hypertension, which have been considered by several researchers as different expressions of the same phenomenon of morning surge [80] . These alterations could be explained because during the first hours of the morning, physiological alterations take place, such as an increase in BP, platelet aggregation, secretion of catecholamine, cortisol, activation of the renin angiotensin system and other hormones [81, 82]. The morning accentuation of these physiological processes, acting on a vulnerable plaque of atheroma can alone or together, contribute to the higher incidence of cardiovascular disease during this time [83]. There are several studies that have consistently verified that MI has a higher prevalence between 6 am and 12 noon than at other times of the day or night [84]. In addition, the incidence of subarachnoid hemorrhage [85]. ischemic cerebrovascular disease [86]. hemorrhagic cerebrovascular disease [87]. And transient ischemic attacks [88]. Is higher in the morning after waking up [89].
The clinical implications of recognizing a circadian cycle of presentation of cardiovascular disease are reflected in the importance that can be given to pharmacological interventions for better protection at times of increased risk. Perhaps, long-term medications administered at night or that do not lose their action by morning, are of clinical utility [90, 91].
There are reports that MI occurs 2 to 3 times more frequently in the morning than at night [91, 92]. In the early hours of the morning, an increase in BP and heart rate results in an increase in the demand for oxygen and energy by the heart, while the vascular tone of the coronary arteries increases, resulting in a decrease in coronary blood flow and oxygen supply. This inconsistency between supply and demand causes the high frequency of MI onset in the morning [93-94]. Other factors are also involved favoring hypercoagulability, such as plasminogen activator inhibitor 1 and platelet surface activators such as P-selectin [95].
In a longitudinal cohort, the Ohasama Study [96] conducted in Japan in which BP was measured every morning, showed that morning BP levels predict cardiovascular death events more accurately than that obtained randomly in that same population. This same cohort was analyzed after 10 years of follow-up, with 1,352 patients (872 women and 460 men), ages over 40 years could be followed, demonstrating that the values of nocturnal BP exceeded daytime BP in the prediction of cardiovascular mortality [97].
Verdecchia et al [98]. studied the relationship between daytime and nighttime BP and BP figures at dawn in a cohort of 3012 patients with essential untreated hypertension and followed them for 8.44 years, of which 268 developed a major cardiovascular event (heart failure, MI or cardiovascular death). They applied the Cox model after adjusting predictive covariates such as age, sex, diabetes, smoking, total cholesterol, LVH and glomerular filtration and observed that the morning surge pattern is an independent predictor of cardiovascular events.
Li et al [99]., studied the prognostic significance of the morning surge pattern using the ¨International Database on Ambulatory Blood Pressure in Relation to Cardiovascular Outcome¨, analyzed 5645 randomly selected patients in 8 countries with an average follow-up period of 11.4 years and concluded that the morning surge pattern independently and significantly predicted cardiovascular events (heart failure, MI or cardiovascular death), suggesting its probable role in stratification of CR through ABPM.
Other researchers have downplayed these findings. Cuspidi et al [100] .in an investigation conducted in 343 patients with TOD to evaluate the pattern of nocturnal hypertension between dipper and non-dipper patients did not find significant differences between these two patterns and the presence or absence of nocturnal hypertension regardless of the TOD they had.
The control of BP is one of the essential therapeutic objectives to reduce cardiovascular risk and cardiovascular morbidity and mortality. In our investigation, it was evident that a considerable number of patients (44.1%) at the time of the study had high BP levels, although the random measurement of BP in the office is not a faithful indicator of the true behavior of BP in patients, due to the existence of various factors among which are the white coat hypertension and others, considering that this is an essential factor in the development of TOD and especially coronary heart disease.
We are aware of the limitations of our study since several factors, some difficult to control, such as physical activity, sleep quality, the prevalence of sleep apnea and the use of fixed periods have not been taken into account for the daytime-nighttime period, the lack of reproducibility that the night/daytime ratio implies, or the phenomenon of “mean regression” when the BP determinations are repeated. On the other hand, some research affirms that the study of patients based solely on an exam is not reliable. The conclusions of the study should be interpreted as hypothesis generators and should be confirmed in future studies with longer follow-up.
In summary, this study shows a very high percentage of hypertensive patients with abnormal circadian BP patterns (non-dipper, riser and extreme dipper) without having statistical significance in the study. The morning surge pattern in relation to the BP control showed values with statistical significance with respect to the rest of the patterns studied, but not with the different types of coronary heart disease. These results suggest the convenience of performing ABPM in order to identify patients with these patterns. Since in clinical practice it is impossible to perform this technique on all hypertensive patients due the lack of access to it, perhaps patients with TOD and especially those with coronary heart disease would benefit more.
The authors have declared that no competing interests exist.
This study did not have external sources of funding.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
