
Case Report | DOI: https://doi.org/10.31579/2692-9562/119
Family Physician & Public Health Consultant Bengaluru, India,
*Corresponding Author: Suresh Kishanrao, Family Physician & Public Health Consultant Bengaluru, India,
Citation: Suresh K, (2024), Chronic Sore Throat in Adults - A Challenge! To Primary Care Providers and Otolaryngologists Too!!, Journal of Clinical Otorhinolaryngology, 6(3); DOI:10.31579/2692-9562/119
Copyright: © 2024, Suresh K. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 22 March 2024 | Accepted: 04 April 2024 | Published: 08 April 2024
Keywords: chronic sore throat; etiology; chronic tonsillopharyngitis; gastroesophageal reflux; laryngopharyngeal reflux
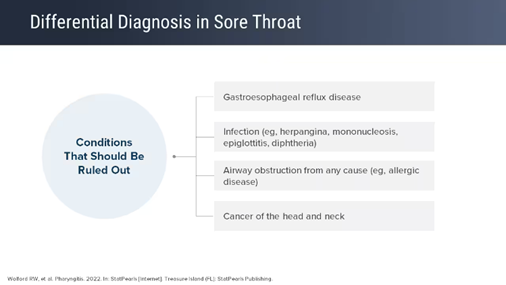
Background: Sore throat, medically called "pharyngitis" is an inflammation or infection of the lymphoid tissues of the posterior pharynx and lateral pharyngeal bands. Acute sore throats among children are one of the most common health conditions that primary health care physicians deal with. It usually resolves on its own without complications in adults. Some adults tend to be more prone to developing frequent infections, basically due to developing fewer antibodies and a less robust immune response in each infection resulting in ‘Chronic Sore Throat’, the subject of this article. Chronic sore throat is to an otolaryngologist, as headache is to neurologist, often seemingly trivial symptom but heavily demanding for bringing relief. The symptoms of chronic sore throat include painful swallowing, scratchy or hot, burning sensation, lancinating pain, a sort of “raw” feeling, and or deep boring pain that worsens with mastication, swallowing and talking. The pain often radiates to the ears and temporo-mandibular joints, aggravating its intensity. Each year, pharyngitis is responsible for more than 40 million visits to health care providers as most children and adults experience 3-5 and 1-2 upper respiratory infection every year and half of the episode may lead to seeking care from primary care physicians or ENT specialists. As with common cold, viral pathogens in pharyngitis appear to invade the mucosal cells of the nasopharynx and oral cavity, resulting in edema and hyperemia of the mucous membranes and tonsils and sometimes even adenoid glands. The etiology of pharyngitis can be either viral, Bacterial, fungal infections or noninfectious origin such as smoking, environmental pollution, and allergic reactions to pollen, mold and pet dander, Laryngopharyngeal reflux (LPR), and rarely throat cancer.
Materials and Methods: This article is based on the experience of managing an adult female patient with Chronic Pharyngitis, second time in last 4 years just on Sunday the 17 March 2024. Diagnosed based on Clinical judgement differentiating between bacterial and viral infections and using Centor Score a Clinical prediction scale. Following this the literature search helped to complete the article.
Results: A physical examination of the throat under a beam of light, recording temperature and auscultating chest. Based on her previous episode in 2020, she was treated with Inj. Benzathine Penicillin 1.2 million IU and Local southerners like warm water gargles and drinking warm milk with Turmeric. She felt better by the next morning and has recovered fully by 21 March 2024.
Conclusions:Chronic Pharyngitis in adults is not rare among adults, mostly viral but rarely lingering Streptococci infection. Clinical judgement in differentiating between bacterial and viral infections, symptomatic treatment with NSAIDs and local antibiotic and or analgesic lozenges and use of antibiotics only if bacterial infection is suspected, must be the guidelines to be followed.
URI= Upper Respiratory Infections, LRI= Lower Respiratory Infections, NSAIDs= Nonsteroidal anti-inflammatory drugs, HIV/AIDS= Human Immunodeficiency Virus, Acquired Immunodeficiency Syndrome, RMPs= Registered medical practitioners,
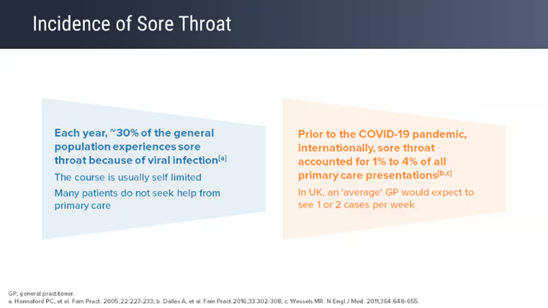
The medical term for a sore throat is "pharyngitis." It usually resolves on its own without complications in adults. Pharyngitis is an inflammation of the pharynx involving lymphoid tissues of the posterior pharynx and lateral pharyngeal bands [1]. Each year, pharyngitis is responsible for more than 40 million visits to health care providers. Most children and adults experience 3-5 viral upper respiratory tract infections, including pharyngitis which forms at least 50% of them per year.
Acute Sore throats: Acute sore throats among children are one of the most common health conditions that primary health care physicians deal with. Bacterial sore throats comprise of only 5–15% of sore throat cases, though antibiotic prescription is common in almost all the sore throat cases. Group A beta-hemolytic streptococcus or Streptococcus pyogenes is the most important bacterial agent associated with acute pharyngitis and tonsillitis. Similarly, Corynebacterium diphtheriae causes occasional cases of acute pharyngitis, as do mixed anaerobic infections (Vincent's angina), Corynebacterium hemolytic, Neisseria gonorrhoeae, and Chlamydia trachomatis. Approximately 50-80% of pharyngitis symptoms are caused by a variety of viral pathogens, common among them are Respiratory Syncytial Virus (RSV), Para-Influenza Virus- (PIV), SARS COV 2 (Covid 19), Human Rhino Virus (HRV), Human Metapneumo virus (hMPV), and Influenza virus and accompany a common cold or influenza. However, the etiology can be either viral, Bacterial, or even fungal infections as well as noninfectious etiologies such as smoking, environmental pollution, and allergic reactions to pollen, mold and pet dander, Laryngopharyngeal reflux (LPR), and rarely throat cancer can result in chronic pharyngitis [2]. 2020-2022 witnessed under reporting of Sore
throat due to Covid 19 set and there after the incidence has again started rising mainly due to lifting restrictions and people not following respiratory hygiene. In 2023 H3N2 Virus infection led to respiratory infections, with fever, sore throat, persistent cough, headache, confirmed by ICMR’s Pan India Respiratory surveillance through 30 viral Research Laboratories in India [3]. This is not the topic of discussion for this article.
Chronic sore throat is to an otolaryngologist, as headache is to neurologist, often seemingly trivial symptom but heavily demanding for bringing relief. Often used irreversibly with odynophagia, the symptom of chronic sore throat includes painful swallowing, scratchy or hot, burning sensation, lancinating (piercing or stabbing) pain, a sort of “raw” feeling, and deep boring pain that worsens with mastication, swallowing and talking. The pain often radiates to the ears and temporomandibular joints, aggravating its intensity [4,5]. This article is based on managing such a case with both oral Penicillin in the past and with Benzathine Penicillin 1.2 million units last week and literature search about the global and Indian current Practices.
On Sunday 17 March 2024 late evening (2030 hrs.) Ms. Divya, in her early 30’s called complaining of sore throat, scratchy sensation, tolerable but piercing pain, mild fever, and deep boring pain that worsened with mastication, swallowing & talking. She had a similar episode in early 2020. A working lady managing office work, household chores, a school going son’s homework etc. and demanding in-laws, keeps her most often under stress. On physical examination her throat showed a little inflammation on the posterior side, Tonsils were almost normal, her voice was bit hoarse, body temperature was 390 C, indicative of chronic inflammation. Knowing her history, clinically diagnosed it as Chronic Pharyngo-tonsillitis and gave her an injection of Benzathine Penicillin 1.2 million units, after a test dose. Asked her to do saltwater gargles and drink Turmeric added Milk before going to bed. The first such episode she had in early 2020 and at that time was treated with Penicillin G Oral tablets for about a week with marginal benefit, then an injection Benzathine Penicillin 1.2 million units was given, which had given a remission till this episode of nearly 4 years. Her throat pain reduced by about half by the next morning. Despite mild fever’s persistence, she had to attend the office the next day after taking care of her morning household chores. By afternoon she was not having fever also. By late evening on Monday, she was almost normal with neither fever nor throat pain, except a bit of weakness. As on Wednesday 20 March 2000 hrs. she confirmed over the phone to be almost normal.
Sore Throat (Pharyngitis) is a common upper respiratory inflammation or infection that usually goes away after a few days. But when the soreness lingers or comes back frequently, it’s called chronic pharyngitis. Acute pharyngitis is more common than chronic pharyngitis. The best recommended management involves treating the symptoms, as it usually subsides within 10 days. Antibiotics are recommended only if bacterial infection is suspected.
Chronic & Recurrent Infections: Chronic and recurrent tonsillitis is a condition that causes swelling of the pharyngeal tonsils and back of the throat and sometimes even the adenoids and the lingual tonsils are also inflamed or infected. The true recurring strep throat means an individual must experience multiple infections during a single respiratory season. Recurring strep throat infections are treated the same way as a primary infection but responds better to long acting Benzathine Penicillin Injections and oral penicillin tablets.
Chronic sore throat, alternatively referred to as “chronic pharyngitis” by otolaryngologists, connotes a recalcitrant medical condition that often defies all possible forms of management. Approximately 30% of patients with chronic pharyngitis have no identifiable cause. “Inflammation of the pharyngeal mucosa and/or the sensation of burning or pricking sensation in the throat that has persists for more than 10 days despite medication” is a working definition one can use. The symptoms of chronic sore throat include painful swallowing, scratchy or hot throat, or a sort of “raw” feeling, burning sensation, lancinating pain, and the typical deep boring pain that worsens with mastication, swallowing and talking. The pain often radiates to the ears and temporo-mandibular joints, aggravating its intensity [7]. Some other specialists use the definition Chronic Pharyngo-tonsillitis if an individual suffers from one or more attacks of Pharyngo-tonsillitis per year or less frequently (once in 2-4 years as the immunity wanes) and the symptoms linger for longer than 10 days.
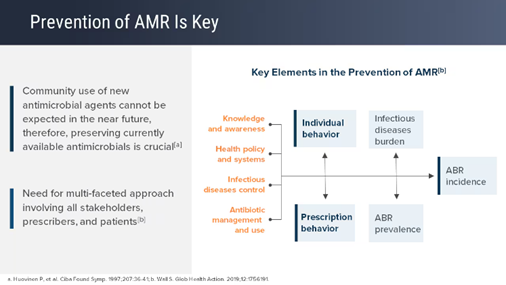
Risk Factors: Some people tend to be more prone to developing frequent infections, basically due to developing fewer antibodies and a less robust immune response to each infection. People who have any underlying condition that weakens the immune system, are at higher risk of such recurrence. Immune system becomes a poor responder if the person is under a great deal of stress, regularly taking a corticosteroid for any medical condition, suffering from illness such as HIV or AIDS, taking immunosuppressive drugs after an organ transplant and chemotherapy for cancer treatment and aging, as our immune system becomes less effective with advancing age. Antibiotic resistance following an inadequate dose, or not completing a full course of antibiotic treatment is common in India. Resistance develops as some patients with strep infection stop taking antibiotics once they start feeling better rather than finishing the entire course. This type of inadequate treatment will be less effective in completely eradicating the infection and leads to Chronic Sore throat. Sometimes even a doctor especially RMPs or quacks in India do not prescribe a strong enough dose to eradicate the bacteria. Either way, the persons keep experiencing relapses over years [8].
Carriers of strep throat bacteria: Some people carry strep bacteria without symptoms. Frequent regular strep throat indicates frequent contact with someone who is a strep carrier, and repeated exposure to the bacteria is infecting [8]. Our case belongs to this group.
Genetic predisposition: A 2019 study reported that many children who had their tonsils removed due to recurrent tonsillitis had a family history of recurrent tonsillitis.
Etiology: Approximately 50-80% of pharyngitis symptoms are caused by a variety of viral pathogens, common among them are Respiratory Syncytial Virus (RSV), Para-Influenza Virus- (PIV), SARS COV 2 (Covid 19), Human Rhino Virus (HRV), Human Metapontum virus (hMPV), and Influenza virus and accompany a common cold or influenza. However, the etiology can be either viral, Bacterial, or even fungal infections as well as noninfectious etiologies such as smoking, environmental pollution, and allergic reactions to pollen, mold and pet dander, Laryngopharyngeal reflux (LPR), and rarely throat cancer can result in chronic pharyngitis [2]
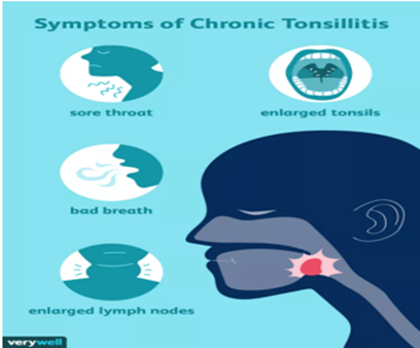
Pathogenesis: As with common cold, viral pathogens in pharyngitis appear to invade the mucosal cells of the nasopharynx and oral cavity, resulting in edema and hyperemia of the mucous membranes and tonsils. Bacteria attach to and result in super-infection. In the case of group A beta-hemolytic streptococci, they invade the mucosa of the upper respiratory tract. While many clinical manifestations of infection appear to be due to the immune reaction to products of the bacterial cell, in diphtheria, a potent bacterial exotoxin causes local inflammation and cell necrosis. Chronic pharyngitis symptoms are like acute pharyngitis symptoms but a bit milder. Common signs include Pain or scratchiness in your throat, Swollen glands in your neck, Hoarseness, Difficulty in swallowing, A tickling sensation in the throat, A tired voice, A sensation that something is stuck in the throat as was complained by our case. If there is an infection over a sore throat the patient develops Fever, Headaches, Coughing, Sneezing. Nausea and vomiting. Chronic tonsillitis tends to have ongoing Sore throat, enlarged tonsils, bad breath, which may be related to cryptic tonsils- pockets in the tonsils where food and debris can accumulate and enlarged and tender neck lymph nodes.Chronic pharyngitis is contagious if it is due to a viral or bacterial infection, and it can be transmitted from one person to another through saliva, mucus, and nasal discharge. Some viruses and bacteria can survive on surfaces for a period, so contact with towels, toothbrushes, clothing or eating utensils can spread the disease [3].
Viral pharyngitis is contagious for the entire period of symptoms presence and antibiotics are not effective. If it is bacterial pharyngitis, a course of antibiotics reduces the length of time of contagiousness to 24 hours of taking an effective antibiotic.
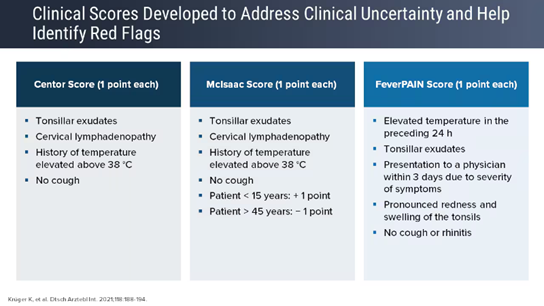
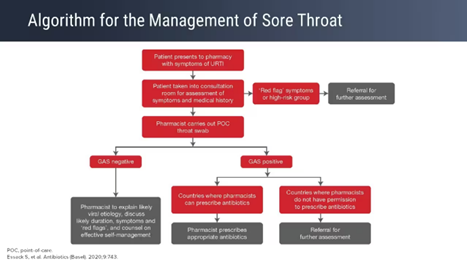
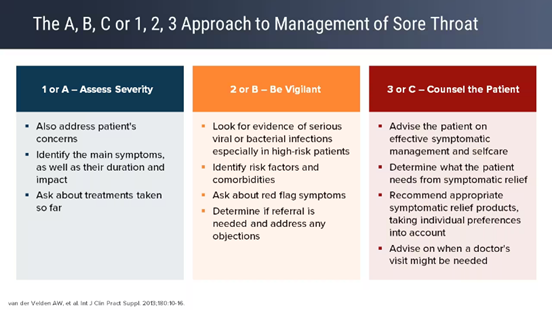
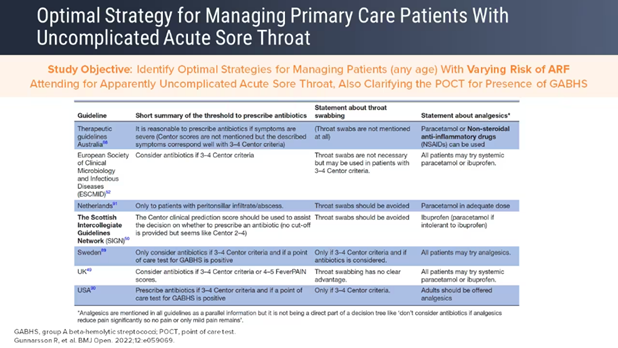
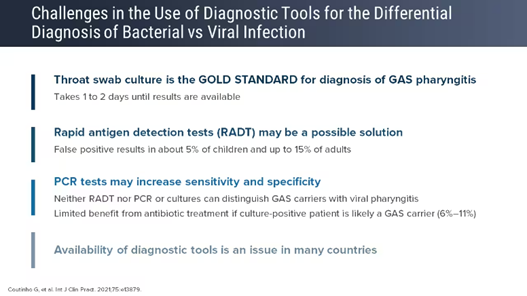
Diagnosis and Tests: A. Clinical judgement is the best for differentiating between bacterial and viral infections. Clinicla prediction scales can also be used. A physical examination includes inspection of the throat under a beam of light, recording temperature and auscultating for LRI if any. Recently three clinical scoring systems have been developed for identifying red Flags for urgent referrals.1. Centor Score: use one point for each of i)
Tonsillar exudates (TE), cervical lymphadenopathy, temperature of 380C or more and No cough 2. McIsaac Score: apart from the four point this sues the age as 5th point giving +1 to age<15>45 yrs. 3. FeverPAIN Score: this scoring system uses i) elevated temperature in preceding 24 hrs. ii) TE iii) consultation in first 3 days due to severity of symptoms, iv) pronounced redness and swelling of Tonsils v) No cough or Rhinitis.
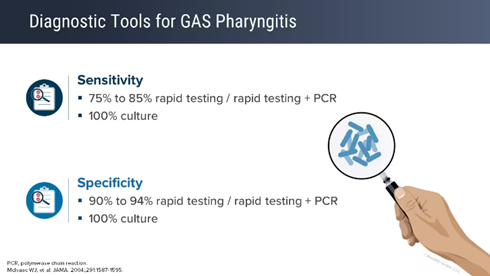
B. Laboratory examinations like CBC, Rapid antigen detection test and a throat swab culture (PCR) if it is a non- viral infection for strep throat may be advised. Rapid testing has a sensitivity of 80-85% and specificity of 90%. PCR has 100% sensitivity and specificity. This test helps in choosing appropriate antibiotics also. However, Indian situation these tests are available only in major urban localities.
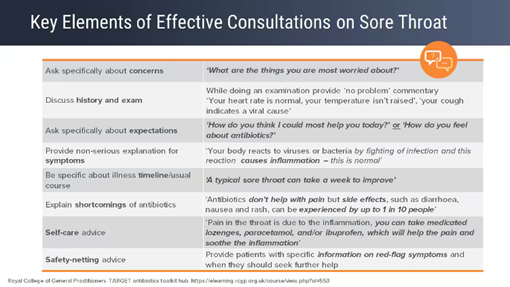
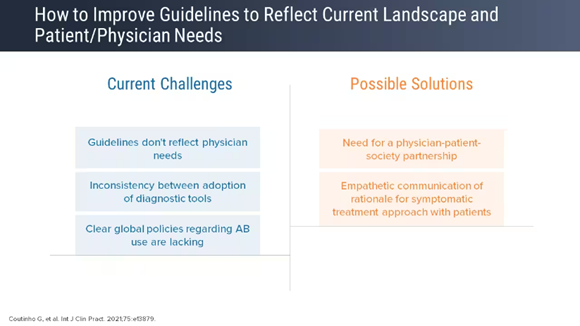
Management and Treatment: There is no single accepted, practical guideline, or a standardized and generalized algorithm on how to approach a patient presenting with chronic sore throat. The multiplicity and heterogeneity of the spectrum of etiologies of chronic sore throat make the task of enumerating them far from exhaustive. Rest, oral fluids, and salt-water gargling, Turmeric added warm milk gargling and then gulping, are the main supportive measures in patients with viral pharyngitis.
Systemic Therapy: NSAIDs- Ibuprofen or Naproxen & Paracetamol (Acetaminophen) Topical Oral Therapy: 1. NSAID Lozenges, sprays, and granules, 2, Anaesthetics and Antibiotics 3. Non medicated Lozenges- traditional gargles, motuh washes
Multiple doses of flurbiprofen lozenges (Vittfen Lozenges, Flurwell 100mg Tab) provide effective relief of sore throat pain intensity as well as difficulty swallowing, a painful or swollen sore throat. Flurbiprofen is a non-steroidal anti-inflammatory drug (NSAIDs) used to relieve pain and inflammation.
Benzocaine Lozenges (Shalusil Black Curren Lozenges, Strepsil Lozenges etc. Orac Turmeric Lozenges)
Antibiotics: Penicillin or amoxicillin is the antibiotic of choice to treat group A strep pharyngitis. There has never been a report of clinical isolation of group A strep that is resistant to penicillin. However, resistance to azithromycin and clarithromycin is common in India. Macrolides is reserved for patients allergic to penicillin. Therefore, for sore throat caused by group A streptococcus, Oral Penicillin for 10 days is the common antibiotic treatment. Alternately a single dose long acting Benzathine Penicillin Injection D-1(1.2 million units for adults and 0.6 million IU for children weighing less than 27 Kg) is advised. Due to slow absorption and hydrolysis, the concentration of the drug in the blood remains lower but for a prolonged period. After a 1.2-million-unit injection, adults have detectable drug concentrations for 14 days, often longer. Please note that only organisms that are very sensitive to penicillin will be inhibited by the low tissue concentrations achieved. The medication is excreted by renal tubular excretion.
The process of Injection: Since the drugs comes in crystalline powder, it needs to be diluted, preferably in 4-5 ml. distilled water, in contrast to procaine penicillin which is usually diluted with 2 ml. water. The Injectoion needs to be given in Deep intramuscularly in gluteal region. In view of the risk of reactions, the need for test dose every time and the difficulty in pushing the thick solution, not many practitioners give this injection these days.
Pharmacokinetics of Benzathine benzylpenicillin: Benzathine is the least soluble salt form of penicillin G, thus providing the longest duration of action. Maximum concentration is observed between 12 and 48 h after injection. Benzathine penicillin G has a long apparent half-life of approximately 336 h with drug input into blood circulation for more than 30 days following a single intramuscular injection. In contrast Penicillin G or Procaine Penicillin will be out of our system after about 7.7 hours after the last dose injection. Injection Procaine Penicillin has an elimination half-life of approximately 1.4 hours or less. 5.5 x 1.4 hours = 7.7 hours for penicillin. Procaine benzylpenicillin interferes with the synthesis of the bacterial cell wall peptidoglycan. It acts through the inhibition of biosynthesis of cell-wall peptidoglycan, rendering the cell wall osmotically unstable [10].
Prevention:
Primary care Physicians & Otorhinolaryngologist must use masks and insist the patients also wear mask, except for a minute or two pf throat examination. Avoid contact with people who are sick, Family members must not share food, beverages or eating utensils, and wash your hands frequently or use antibacterial hand sanitizer when soap and water isn’t available. When chronic pharyngitis persists despite optimum management, especially in chronic granular pharyngitis, an allergic etiology (atopy) may be found associated with rhinosinusitis a course of steroids in conjunction with long-acting antibiotics like Benzathine Penicillin and topical gargle will lead to temporary remissions. Further investigations like absolute eosinophil count, immunoglobulin E assay, skin prick test for allergens, radio-allergosorbent test (RAST) can be carried out, and subsequent prolonged antiallergic/immunomodulatory treatment with rehabilitation might lead to long-term resolution.
Recent studies:
Chronic Tonsillitis (CT):
Sudan Study: A cross-sectional descriptive study in June-September 2022 which screened using a structured questionnaire of 297 Patients who presented to all ENT clinics in Secondary Care Hospitals in Rabak City, Sudan. 77 patients were confirmed to be having CT based on the inclusion criteria. The prevalence of CT was 25.9 % (77) among all screened patients. The majority (67.5%) of the patients with CT were male, and remaining one third were female. While most cases were in the age group of 11-20 years (32.4%), 15 cases (20%) were in the age group of our case 31-40 yrs. One third of them (32.4%) were residing in the urban-industrial part of the city, as was our case. All the patients with CT complained of throat pain, while 88% presented with red inflamed tonsils, 67% had Fever, 65% had Jugulodigastric lymph nodes enlargement, 56% had other constitutional symptoms, and 46% had Odynophagia. Laboratory investigations of these patients revealed 64% to have Neutrophilia, while 54 and 50% had high ESR and positive ASO titer, respectively. While (30%) were managed medically 57% of the patients had to undergo tonsillectomy [9].
Kolkata, India Study: In another hospital-based descriptive study in Kolkata, India over a period of 3 years (January 2014 to December 2016). In this study 1580 patients with chronic sore throat (>12 weeks duration, despite conventional medication) were evaluated in a tertiary care teaching institute of Kolkata eastern India. A detailed history, appropriate investigations, and a self-designed algorithm were used. There was a minimal female preponderance, the female: male ratio being 1.25. About 39% of patients were chronic smokers, and 31% were addicted to alcohol. Forty-three (2.72%) patients were reactive to HIV 1/2. The study provided a detailed account of the heterogeneous etiology of chronic sore throat, and an overall structured idea on how to approach its work-up and diagnosis. Chronic tonsillopharyngitis, gastroesophageal reflux disorder, submandibular sialadenitis, and laryngopharyngeal reflux disorder were the chief causes of chronic sore throat. Allergy, psychiatric illnesses, oral submucous fibrosis, comorbidities (diabetes mellitus, hypothyroidism, uremia, arthritides), stylalgia, Koch’s pneumonitis, recurrent aphthous ulcers, and dietary deficiencies formed the other major causes The study also developed an approach to the Chronic sore throat problem in the day-to-day clinical practice of otolaryngology and general medicine. However, since the study was chiefly population-based and considered a multiplicity of causes for chronic sore throat, the “investigation of choice” for certain ailments were out of scope for the study design [5]. Being a study that primarily aimed at delineating the oled of one of its symptoms; they relied on the patients’ history and nasopharyngolaryngoscopy findings for diagnosis. Despite some limitations like24-hr double probe pH monitoring, the gold standard for the diagnosis of laryngopharyngeal reflux disorder, the researchers believe that the study would provide a useful overview of the wide spectrum of differential diagnoses of chronic sore throat and would be helpful in a practical set-up that deals with a huge number of patients with such complaints. The study population, although large enough to predict reproducibility of the results, could have been further increased by making more representative of the prevailing economic strata of society, had it been designed as multicentric, involving the other teaching referral hospitals of the area as well as the corporate institutions. [5].
The research team of the study recommended the following Logarithmic chart for use by general practitioners and Otorhinolaryngologist, which this author has tried in about 11 patients including the one reported in this article and found it to be useful.

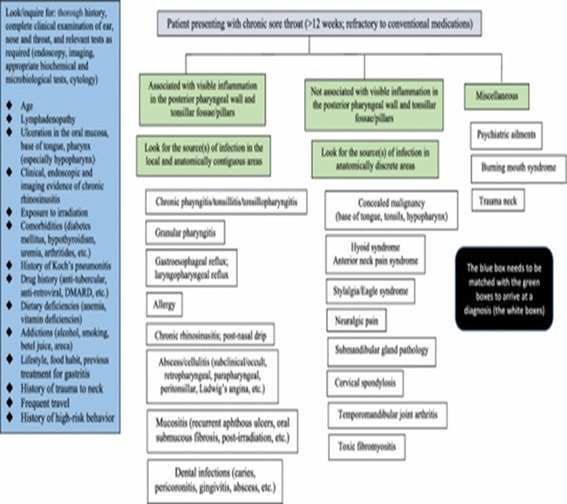
Source: Encountering Chronic Sore Throat: How Challenging is it for the Otolaryngologists? [5]
Haryana, India Study: A community-based survey over a two-year period, (Aug 2012 to Aug 2014) of 3765 children under 10 years followed up for 5578 child years. 1069 episodes of sore throat were reported, and swabs were collected from 8% of the cases randomly. The incidence of sore throat and viral sore throat was 191.7 and 60.1 episodes per 1000 child-years (EPTCY), respectively, indicating that nearly one third of the sore throat episode in India are viral in origin. Fever (OR 5.40,) and running nose (a OR 10.16) were significantly associated with viral sore throat. The clinical score of fever, running nose, and headache had an overall sensitivity of 86.2%, specificity of 62%, and Area under the Curve (AUC) of 0.78 in predicting viral sore throat [6]. This study adds to the information and knowledge about epidemiology of viral sore throats in India and infers that Viral sore throat contributes to a significant problem in the community and emphasizes on symptom attributes of URIs due to viral etiology. It recommends that clinical scores could be utilized in primary care settings for predicting viral URI, thereby guiding antibiotic prescription. These algorithms will be cost-effective, less time consuming and have a greater impact in aiding primary care physicians for optimal utilization of antibiotics.
The Challenges: Chronic sore throat is to an otolaryngologist, as headache is to neurologist, often seemingly trivial symptom but heavily demanding for bringing relief. Often used irreversibly with odynophagia. Considering the extent to which the quality of life of the patients is impaired, it is often challenging for the practicing general physician and even otolaryngologists to deal with this recalcitrant, nagging problem without dismissing the symptoms as “fictitious” and “psychogenic”. But where no such cause can be established, it might be judicious to take a throat swab for aerobic culture and sensitivity. Organisms like Pseudomonas Areosa may be detected and can be treated with for about 2 months. An antibiogram with causative organism(s) promises a good prognosis. However, when there is an absence of growth at 48 h, a trial of second or third generation cephalosporins or macrolides with azoles or antifungals might produce surprising results. Another challenge is with persistence of sore throat sans clinical pharyngitis or following remission of clinically evident pharyngitis. In such situations, exploring the adjacent anatomic areas/structures for other causes becomes necessary. These include the submandibular glands (chronic sialadenitis), elongated styloid (stylalgia/Eagle syndrome). and treating them accordingly with fluoroquinolones might benefit with/without surgical excision for chronic sialadenitis, and carbamazepine/tricyclic antidepressants. Neoplasms at the base of tongue, vallecula and tonsils require special mention as they often remain hidden and need to be visualized through indirect laryngoscopy and flexible nasopharyngolaryngoscopy. Chronic laryngitis and laryngopharyngeal reflux might, rarely, give rise to this peculiar “sore throat” sensation These conditions are identifiable clinically by flexible nasopharyngolaryngoscopy from the characteristic mucosal changes, and treated subsequently after exclusion of other surgical pathologies like hiatus hernia. Dietary deficiencies, often associated with clinical pallor, cheilosis, glossitis, dysphagia, aphthous ulcers, dermatitis, and diarrhea, might also result in chronic sore throat like Plummer Wilson Syndrome can be managed by supplementation with hematinic, multivitamins with microelements like zinc, apart from treating the primary cause. Certain common systemic disorders and comorbidities causing immunosuppression can also affect the throat, like type 2 diabetes mellitus, hypothyroidism with history of subacute thyroiditis and uremia. These need to be identified promptly as the possible cause(s) or contributing factor(s) for persistence of sore throat, and respective directed treatments should be initiated at the earliest [7,9]. Patients on disease modifying antirheumatic drugs (DMARD) as in arthritides, skin ailments like pemphigoid or lichen, and connective tissue disorders, and long-term oral steroids for asthma are also prone to repeated attacks of sore throat and its persistence, along with recurrent aphthous ulcers, oral candidiasis, and xerostomia. In these patients, systemic examination of musculoskeletal, urogenital, integumentary and uveoretinal systems becomes mandatory. Infectious viruses, especially hepatitis C and human immunodeficiency virus (HIV) bring with them their own oral and oropharyngeal manifestations which might result in chronic sore throat. In India use of betel quid, tobacco as pan masala and smoking, complicated by chronic alcohol intake, might lead to oral submucous fibrosis. The condition is characterized by intense burning sensation in mouth and mucosal changes where the oral and oropharyngeal mucosa becomes smooth, atrophic, characterized by hyaline degeneration resulting in decreased elasticity, often associated with vesicles, erosion, and hyper melanosis. Abstinence from the primary cause with topical/systemic/intralesional steroids along with long-term antioxidant therapy can potentially lead to clinical remission in most patients. Besides, toxic fibro myositis following influenza (H3N2) might result in prolonged tenderness over anterior aspect of neck, especially over the greater corn of hyoid, producing pain during swallowing [3,9] as was experienced by many people in India after H3N2 outbreaks. Other relatively less common entities associated with chronic sore throat but often ignored include burning mouth syndrome and chronic fatigue syndrome, which need to be treated with antidepressants, oral artificial saliva application, lifestyle modification, and treatment of the respective causes of dry mouth, provide rewarding results on many occasions [7,9].
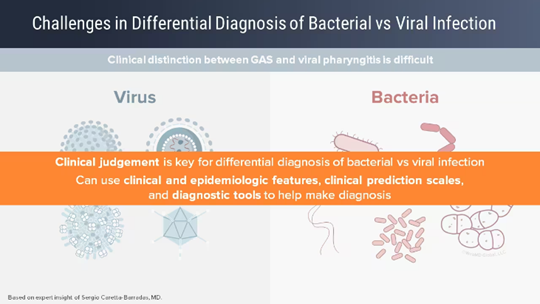
A community-based study indicates that in India the incidence of sore throat and viral sore throat was 191.7 and 60.1 episodes per 1000 child-years (EPTCY), respectively, indicating that nearly one third of the sore throat episode in India are viral in origin. Fever (OR 5.40,) and running nose (a OR 10.16) were significantly associated with viral sore throat. Managing a patient with chronic, recalcitrant sore throat is often one of the most challenging encounters for the family physician and even Otorhinolaryngologists.Logical structuring of the clinical problem, through detailed history, examination, specific, investigations, and appropriate drug therapy, will result in satisfying outcome. A structured algorithm based on a wide spectrum of possible differential diagnoses is a good protocol developed indigenously. Chronic tonsillopharyngitis, gastroesophageal reflux disorder, submandibular sialadenitis, laryngopharyngeal reflux and allergy constituted the most frequent reasons for chronic sore throat and its persistence in India. There is no single accepted, practical guideline, or a standardized and generalized algorithm on how to approach a patient presenting with chronic sore throat. Rest, oral fluids, and salt-water gargling, Turmeric added warm milk gargling and then gulping, are the main supportive measures in patients with viral pharyngitis. The current guidelines suggest that treatment should be symptomatic and antibiotic to be prescribed only if bacterial infection is suspected clinically. Where available rapid test kits and PCR may be used especially if the patient does not respond to antibiotics. Gentle exercises such as walking, yoga, swimming, or Tai Chi boost your endorphins, providing natural stress relief.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
