
Research Article | DOI: https://doi.org/10.31579/2692-9562/060
Department of ENT, Rostov State Medical University, Rostov-on-Don, Rostov Region, Russian Federation.
*Corresponding Author: Natalia V Boiko, Department of ENT, Rostov State Medical University, Rostov-on-Don, Rostov Region, Russian Federation.
Citation: Natalia V Boiko, Irina V Stagnieva, Olga E Lodochkina. (2023), Chronic Rhinosinusitis with Polyps and Comorbid Asthma: Results of Reslizumab Treatment. Journal of Clinical Otorhinolaryngology 5(2); DOI: 10.31579/2692-9562/060
Copyright: © 2023, Natalia V Boiko. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 06 January 2023 | Accepted: 16 January 2023 | Published: 28 January 2023
Keywords: chronic rhinosinusitis; heterogeneous diseases
The aim of this study was to determine if exposure to ten minutes of silence trigger the temporary tinnitus Transition from standardization to personalized treatment have led to the separation of such heterogeneous diseases as asthma and chronic rhinosinusitis (CRS) into clinically similar groups called phenotypes.
Transition from standardization to personalized treatment have led to the separation of such heterogeneous diseases as asthma and chronic rhinosinusitis (CRS) into clinically similar groups called phenotypes.
From the clinical viewpoint CRS is commonly divided into two phenotype-based groups on the presence (CRSwNP) or absence of nasal polyps (CRSsNP). The first phenotype is associated with eosinophilic or Th2- inflammation while the second - with neutrophilic or non-Th2- one [1]. In 80-90% of patients suffering from CRS with polyps, a significant systemic and local eosinophilia is identified, along with an increase in the local level of Th2-dependent cytokines, such as interleukin 4, 5, 9, 13, 25, 33 (IL-4, IL-5, IL-9, IL-13, IL-25, IL-33), increased expression of the receptors to IL-5 and local production of immunoglobulin E (IgE), while the key mediator of eosinophilic inflammation is IL-5, which provides activation, chemotaxis and survival of eosinophils [2].
CRS with polyps is often combined with asthma. In patients with asthma, CRSwN is detected in 7-16% of cases and more than 80% have X-ray signs of inflammatory diseases of the paranasal sinuses [3, 4], while in 26-48% of patients with CRSwNP the concomitant disease is asthma [5, 6]. These comorbid diseases mutually burden each other: on the one hand, asthma in patients with CRSwNP is much more severe [7, 8], on the other hand, this group of patients is characterized by more frequent reсurrence of polyps after surgical treatment [9].
Asthma is also a group of clinical variants that differ in pathophysiological parameters, the type and severity of inflammation, the response to corticosteroid therapy, and many other factors. Currently there are several phenotypes of asthma: allergic, non-allergic (eosinophilic), asthma with permanent obstruction, infection-dependent, asthma with late onset, asthma associated with obesity [10, 11]. Inflammation in eosinophilic asthma has similar features to that in patients having CRSwNP: an increased content of eosinophils in the mucosa, in sputum and in blood, Th2-type of inflammatory reaction with hyperproduction of IL-5 and eosinophil cationic protein (ECP) [12].
In the last decade, a new promising direction has appeared in the treatment of asthma – targeted therapy with humanized monoclonal antibodies (biologics) [13, 14].
The correlation between the severity of CRSwNP and eosinophilic asthma, the proximity of the endotypes of these diseases [15] along with the successful use of biologics for the treatment of severe asthma [13] explain the interest in the research of the possibility of using this group of drugs in patients with CRSwNP, although there are just a few studies of this kind [16, 17, 18, 19, 20]. Since there are no approved indications for the treatment of CRS other than dupilumab, numerous studies have been conducted on patients receiving monoclonal antibody-based medications for the treatment of severe asthma. Objective. The aim of the research was to study the dynamics of nasal symptoms in patients with CRSwNP combined with asthma during reslizumab treatment.
Reslizumab is a humanized monoclonal antibody with a high affinity for IL-5. Reslizumab specifically binds to IL-5, causing a restriction of differentiation, chemotaxis, activation and survival of eosinophils [21, 12], thereby reducing the level of eosinophilic inflammation and remodeling of the respiratory tract. Patients and methods. 18 patients aged 29 to 59 years undergoing treatment with reslizumab for severe eosinophilic asthma have been examined during the research. The study was conducted in pulmonological departments of multidisciplinary medical institutions in Rostov-on-Don (Regional clinical and diagnostic center and Regional clinical hospital) from May 2019 to May 2021.
Selection criteria for reslizumab treatment. Patients over 18 years old with a confirmed diagnosis of eosinophilic asthma, eosinophilia of blood and sputum, lack of adequate control of asthma symptoms or exacerbations more than once a year, despite standard treatment relevant to stages 4-5 according to 2019 GINA classification [22]. Reslizumab was injected intravenously at a dose of 3 mg per 1 kg once in every 4 weeks as a supplement to the baseline therapy of asthma (medium and high doses of inhaled corticosteroids in combination with long-acting β2-agonists), which patients had previously received.
Patients’ examination before the start of the treatment and after 6 injections of reslizumab included endoscopy of the nasal cavity with determination of the total polyp score (TPS), computed tomography (CT) of the paranasal sinuses, rhinocytogram, determination of the content of eosinophils in the blood and ECP in the blood serum, allergological examination via the Immuno CAP method and spirometry. The total polyp score (TPS) was evaluated in points according to the standard scheme: 0 - no polyps, 1 – small polyps in the middle meatus not reaching below the inferior border of the middle concha; 2 - polyps reaching below the lower border of the middle turbinate; 3 - large polyps reaching the lower border of the inferior turbinate or polyps medial to the middle concha; and 4 - large polyps causing complete obstruction of the inferior meatus.
The TPS index was determined as the sum of the right and left nostril scores. The CT images of the paranasal sinuses and the ostiomeatal complex were evaluated on the Lund-Mackay score. The rhinocytogram was carried out via the method of liquid cytology with the sample staining according to the Papanicolaou method (Pap test). Special cytobrushes placed in a bottle with a transport medium were used for collecting nasal mucus. The level of systemic eosinophilia was assessed according to the cell content in 1 µl. The cell content was calculated by the formula: the number of leukocytes 109 × the number of eosinophils in percent ×10. To analyze the dynamics of clinical symptoms, the SNOT-22 questionnaire (Sinonasal Outcome Test-22) and the ACT (Asthma Control Test) were used. The effectiveness of asthma symptom control was evaluated by a pulmonologist by the reducing frequency of asthma exacerbations (including those exacerbations requiring the use of systemic corticosteroids), improvement of the quality of life, spirometry, and ACT results.
Statistical analysis of the results was carried out via "Statistica 12.0” program (StatSoft, USA). The normality of the distribution of values in the sample was checked with Shapiro-Wilk test. The values in the sample were represented as the average sample value with its errors, median, interquartile range. The statistical significance of the difference in the dynamics of indicators was evaluated using the Wilcoxon test for dependent samples.
During the initial examination, subjective symptoms of nasal and paranasal sinus pathology were revealed in patients: watery (more often) or thick nasal discharge (18/18), persistent (12/18) or intermittent nasal obstruction (6/18), postnasal congestion (12/18), decreased sense of smell (14/18).
The duration of the disease ranged from 2 to 17 years, and in 7 patients the disease began with the appearance of symptoms of rhinitis in the form of abundant watery discharge from the nose and sneezing attacks, however multiple allergological examination did not reveal any signs of sensitization. Subsequently, those patients had nasal congestion, followed by asthma symptoms and nasal polyps. During the endoscopic examination, nasal polyps were found in 15 patients with a TPS index from 2 to 5. CT of the paranasal sinuses in this group of patients showed signs of involvement to all sinuses, with a Lund-Mackay index from 11 to 20.
In 3 patients, no polyps were found in the nasal cavity, there was swelling of the nasal mucosa during endoscopy and thickening of the paranasal sinus mucosa on CT. Those patients were observed for a long time with a diagnosis of allergic rhinitis. However, the detected eosinophilia of the rhinocytogram (up to 75%), a significant increase of ECP in blood and two-fold negative results of the allergic tests allowed us to diagnose those patients with non-allergic rhinitis with eosinophils (NARES). Here it should be mentioned that in those patients, a more evident effect of reslizumab was noted in the regression of nasal symptoms according to SNOT-22, but the indicators of ACT and Forced expiratory volume in 1 second (FEV1) did not improve significantly.
The dynamics of the studied indicators is presented in Table 1. A significant decrease in blood eosinophilia was registered in all patients after the first administration of reslizumab and the low level of eosinophils remained throughout the entire follow-up period, despite some fluctuations in this parameter. Improvement of nasal breathing was noted by 16 out of 18 patients, what was displayed in the dynamics of SNOT-22. Disappearance of hyposmia after the first injection of the drug was noted by 8 patients, in 4 more patients hyposmia disappeared 2 months after the start of the treatment. The positive dynamics was confirmed by endoscopy data (reduction of TPS) and CT of the paranasal sinuses. In 12 out of 18 patients, a decrease in the severity of asthma symptoms was noted: a significant improvement in the FEV1 index, improved exercise tolerance, reduced need for salbutamol or other short-acting b2 agonists, improved quality of sleep and emotional background. Along with that there were no exacerbations of asthma registered during the entire follow-up period. An increase in the AST index of more than 20 was observed in 12 out of 18 patients, which indicates that control over asthma symptoms had been achieved, and moreover all those patients were diagnosed with CRSwNP. The absence of subjective and objective improvement was registered in 1 patient with aspirin-exacerbated respiratory disease (AERD).
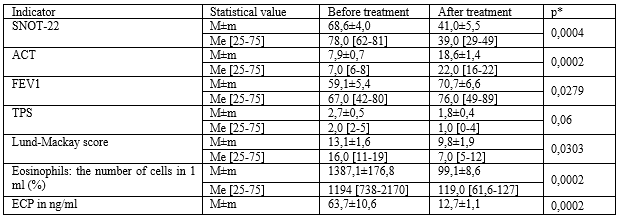
* - the confidence probability of differences in the dynamics of observation, the Wilcoxon signed-rank test was used, M±m is the average sample value and the error of the average value, Me stands for the median, [25-75] is the interquartile range, statistically significant differences are highlighted in bold.
Table 1: Changes in the main indicators characterizing the effectiveness of reslizumab treatment.
To illustrate the results described above, we present an extract from the medical history of patient X, who showed the most evident effect of the reslizumab treatment. Patient Х., 41 y. o., suffers from severe persistent controlled bronchial asthma, GINA step 5, CRSwNP. The disease began at the age of 27 with attacks of rhinorrhea and sneezing. The patient noted abundant watery discharge from the nose, not accompanied by nasal congestion and itching in the nose, which lasted for 11 years. Repeatedly conducted tests did not reveal any sensitization. At the age of 38, a paroxysmal cough appeared, more often at night. The pulmonologist diagnosed asthma, started treatment with inhaled glucocorticosteroids in combination with long-acting β2-agonists. Meanwhile, the patient noted increasing difficulty of nasal breathing, progressive hyposmia; nasal topical corticosteroids were added to the course of treatment, which he used irregularly. After 2 years, while undergoing the general therapy for asthma, he experienced several episodes of eosinophilic pneumonia. Asthma exacerbations requiring hospitalization became more frequent up to 3-4 times a year, a need for treatment with systemic corticosteroids (in courses) became necessary. Considering the severe course of asthma, the patient was selected for the reslizumab treatment group. While being examined, the patient complains of nasal obstruction, lack of smell, postnasal congestion (64 points according to the SNOT-22). Endoscopic examination revealed swelling of the nasal mucosa, the presence of medium-sized polyps (TPS 5). The results of CT of the paranasal sinuses on the Lund-Mackay score: R10L10T20. The initial number of eosinophils in the blood is 2487 cl/mcl, in the rhinocytogram - 36%, the ECP of the blood equals 168 ng/ml. The patient received 6 injections of reslizumab at a dose of 3.0 mg/kg with an interval of 4 weeks. The evaluation of the treatment results was carried out 6 months after the start of treatment.
After the first administration of reslizumab, the patient noted the the disappearance hyposmia and rhinorrhea and improvement of nasal breathing (29 points in the SNOT control study). During endoscopic examination of the nasal cavity, there are no polyps on the right, on the left they are identified in the middle nasal meatus, they do not go beyond the lower edge of the middle nasal concha - TPS 1 (Fig. 1). CT revealed a significant improvement on the Lund-Mackay score: R2L3T5 (Fig.2). The number of eosinophils in the blood decreased to 136.4 cl / ml, in the rhinocytogram-to 17%, the ECP of the blood was 20.1 ng/ml.

Figure 1: Endoscopy of the left half of the patient X’s nose, 41 y.o.: a - before the treatment, b -6 months after the treatment with reslizumab.

Figure 2: SCT of the paranasal sinuses of patient X: a, b, c, - before the treatment, d, e, f, - 6 months after the start of the treatment with reslizumab
According to the pulmonological study of the changes in AST from 7 to 22 points, a significant improvement in lung function was registered (FEV1 86% and 103%, respectively). During the follow-up period of 6 months, there was no need for systemic corticosteroid therapy.
In our research we have evaluated the dynamics of nasal symptoms when using reslizumab in patients with severe eosinophilic asthma. The presence of CRSwNP was detected in 15 of the 18 studied patients, 3 patients had symptoms of chronic rhinitis as a manifestation of NARES. Changes in the CT were present in 100% of cases. Along with a noticeable improvement in asthma control, which was confirmed by studies of lung function, patients showed clinical, endoscopic, radiological signs of a decrease in the severity of nasal symptoms. The improvement in the quality of life was confirmed by the results of SNOT-22, which revealed a decrease in symptoms such as rhinorrhea, nasal obstruction, hyposmia and sleep disorders.
The data of endoscopic examination revealed a reduction of polyps in 1 out of 15 patients, which indicates the possibility of reverse development of remodeling of the nasal mucosa during targeted therapy. No positive dynamics of nasal symptoms and the course of asthma was noticed in one patient with AERD. In the case of another patient control over asthma symptoms was achieved (an increase in AST from 8 to 22 and FEV1 from 86% to 106%), however the growth of polyps continued (TPS increased from 2 to 5).
The improvements observed in patients with CRSwNP and comorbid asthma testify that reslizumab affects eosinophilic inflammation of both the lower and upper respiratory tracts. The results of our clinical study coincide with the conclusions of earlier observations [17, 23].
In the literature there is certain evidence that the presence of polyps in patients with eosinophilic asthma allows predicting a positive result in the treatment with reslizumab. Thus, S. F. Weinstein et al. [4] performed a retrospective analysis of the patient-reported medical histories of 953 patients with inadequately controlled asthma treated with reslizumab for 52 weeks. 150 patients (16%) had self-reported CRSwNP, endoscopic examination of the nasal cavity and CT of the paranasal sinuses were not conducted. Despite these serious limitations, the authors proved that patients with CRSwNP were highly responsive to treatment with reslizumab. We also noted more significant positive changes in AST and spirometry indicators in patients having CRS with nasal polyps.
Patients without nasal polyps with recurrent symptoms of rhinitis (rhinorrhea, sneezing, nasal congestion) are of particular interest. These patients were observed for a long time with a diagnosis of allergic rhinitis. However, the detected eosinophilia of the rhinocytogram (up to 75%), an increase in the ECP content in the blood and at least twice the negative results of the allergic tests allowed us to diagnose these patients with NARES. In the group of patients with CRS with nasal polyps, it was possible to detect the anamnestic presence of similar symptoms at the beginning of the disease. These results confirm the previously suggested assumption that NARES may be a predictor of the development of AERD, non-IgE-related asthma and nasal polyps [24].
The study of the cytokine profile of inflammation clarifies the pathogenetic features of various phenotypes of the disease, which determines the direction of targeted therapy [25, 5, 26]. However, the studies of the content of cytokines in the tissues of polyps and the nasal mucosa [5] are currently beyond the scope of practical health care. Today the prediction criterion for the effectiveness of reslizumab is an increase in the number of eosinophils in the blood of more than 400 cells/ml. Further studies of the use of monoclonal antibodies should reveal additional clinical criteria for the selection of patients with CRS with polyps for the use of this group of drug
Reslizumab treatment of patients with eosinophilic asthma and concomitant chronic rhinosinusitis with nasal polyps and chronic non-allergic rhinitis (NARES) leads not only to improved control of asthma symptoms, but also to a significant regression of nasal symptoms.
Clinical significance. Currently, the indications for the treatment of chronic rhinosinusitis with polyps have been registered in dupilumab alone. Studies of the effects of other biologics can not only expand the their indications, but also identify possible advantages in the selection of drugs for the treatment of different types of CRS.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
