
Case Report | DOI: https://doi.org/10.31579/2693-4779/248
1Medical Professor at the Bahiana School of Medicine and Public Health, Salvador – BA/Brazil.
2Medical student at Bahiana School of Medicine and Public Health, Salvador – BA/Brazil.
*Corresponding Author: Calil Darzé Neto, Medical Professor at the Bahiana School of Medicine and Public Health, Salvador – BA/Brazil.
Citation: Calil Darzé Neto, Mariana Sousa De Pina Silva, (2025), Chronic Inflammatory Demyelinating Polyradiculopathy Associated with Rhabdomyossarcoma of The Retroperitoneum: A Case Report, Clinical Research and Clinical Trials, 12(2); DOI:10.31579/2693-4779/248
Copyright: © 2025, Calil Darzé Neto. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 November 2024 | Accepted: 02 January 2025 | Published: 03 February 2025
Keywords: CIDP; rhabdomyosarcoma; autoimmune; case report
This case report is about a 24-year-old patient, with a previous diagnosis of idiopathic chronic inflammatory demyelinating polyradiculopathy (CIDP), which evolved with the appearance of a retroperitoneal tumor, characterized in the anatomopathological examination as a rhabdomyosarcoma, in addition development of conus medullaris and cauda equina syndrome.
Chronic inflammatory demyelinating polyneuropathy (CIDP) is an autoimmune disease with an incidence of 0.2-1.6 per 100.000 people [1], which mainly affects male patients [2,3], and has a poorly understood etiology. The most widely accepted theories include a humoral response by the individual, mediated by B and T lymphocytes, which attack structures in the myelin sheath of the peripheral nerves [3,4], thus generating a progressive or relapsing condition of paresthesia, hypo/reflexia, flaccid weakness, among others.5 CIDP is not considered a remote or direct effect of cancer, and there are few reports of its association with solid tumors [6,7]. This report describes the case of a patient with CIDP who developed a rhabdomyosarcoma of the retroperitoneum.
R.B.S., male, Brazilian, 24 years old, previously healthy and with no relevant family history, was admitted in March 1994 with a history of paresthesia in the upper limbs (UL) and lower limbs (LL), lumbar pain and progressive weakness in the LL which evolved to the UL over a period of eight months. The neurological examination revealed flaccid areflexic tetraparesis, hypotonia in all four limbs and tactile and painful hypoesthesia in boots and gloves. In complementary tests, the cerebrospinal fluid (CSF) examination showed 1100mg/100ml of proteins and 10 lymphocytes/mm³, the electroneuromyography (ENMG) was compatible with standard demyelinating polyradiculoneuritis and the ELISA for HIV was negative. He was treated with prednisone 01mg/Kg/day and returned to walking after six weeks. He was discharged on prednisone 20mg/day and advised to continue with physiotherapy and outpatient neurological follow-up.
Eleven months after starting treatment, the patient was readmitted with weight loss, generalized muscular atrophy, worsening weakness in the upper and lower limbs, pain in the lower limbs and lumbar region, intestinal constipation and urinary retention. Rectal examination revealed reduced tone in the external anal sphincter, and a neurological examination revealed saddle hypoesthesia. Due to low back pain, an x-ray of the lumbosacral spine was performed (02/16/95) which showed no alterations. He took analgesics and prednisone 60 mg/day, with partial improvement in his pain and general condition. During hospitalization, he developed urinary incontinence, abdominal pain, anorexia, and weight loss of 17 kg. On examination of the abdomen, a mass was palpated on the right flank and the patient developed crural paraplegia and a sensory level at T12 on neurological examination. The radiography of the lumbosacral spine, on this occasion, showed osteoblastic lesions of L1, L2, L3 and first sacral pieces (06/95) and total abdominal ultrasound revealed a retroperitoneum occupied by a large mass and bilateral hydronephrosis. The patient was transferred to the ICU due to prolonged periods of apnea and died two days later due to respiratory failure.
In the anatomopathological study, a large tumor mass was observed in the retroperitoneum, measuring 20x12x10cm and weighing 2.150g. The tumor involved the aorta and its main branches, the inferior vena cava, the right ureter and caused upward displacement of the kidneys. In the posterior region, there was involvement of the thoracic vertebrae (from the 8th vertebra onwards), the lumbar vertebrae with invasion of the iliac bone and coccyx. The periaortic lymph nodes were enlarged and fused to the mass. Examination of the chest cavity revealed a hemothorax of 2000ml, which was the factor responsible for the patient's respiratory failure and death.
Examination of the brain showed no alterations, but the spinal cord showed thickening of the nerve roots due to tumor infiltration in the lumbosacral region. The histopathological diagnosis of the neoplasm was characterized as rhabdomyosarcoma of the alveolar type (Figures 1, 2). The autopsy was performed at the Pathological Anatomy Service of the Hospital das Clínicas of the Federal University of Bahia (UFBA).
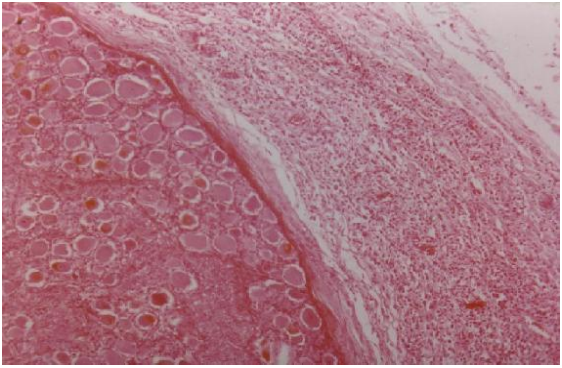
Figure 1: Nervous ganglion of the sympathetic chain, showing neoplastic infiltration in the periphery.
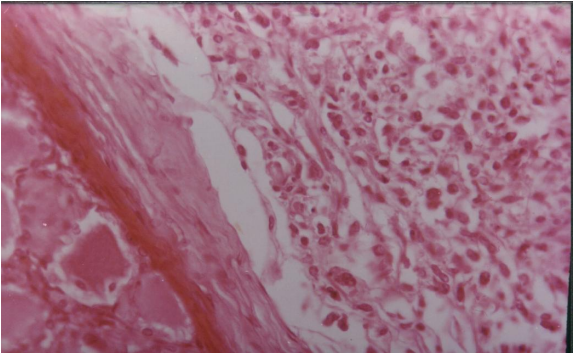
Figure 2: Details of the previous figure showing the alveolar sarcomatous pattern of the infiltrative neoplasm.
We present the case of a patient with typical CIDP, who two years after the onset of symptoms developed a rhabdomyosarcoma of the retroperitoneum. Although rare, the association between CIDP and solid tumors has been described. [6,7].
Some authors suggest that the expression of tumor antigens similar to Schwann cells leads to the production of antibodies that react with these cells, promoting the appearance of CIDP. [8,9]. However, it is difficult to determine whether the association between carcinoma and CIDP is a coincidence or depends on a paraneoplastic process, since cancer is a common clinical entity. 9 In the case reported, the clinical and laboratory findings, as well as the evolution and response to corticosteroids justify the diagnosis of CIDP. [10.11]
At the beginning of the illness, there were no signs of a solid tumor. Rhabdomyosarcoma is a malignant soft tissue tumor, more common in patients under the age of twenty, which usually develops in the head, neck, genitourinary tract, retroperitoneum and extremities. Identifying the histological type is important because the alveolar subtype, in addition to having the worst prognosis, spreads rapidly, [12,13] thus pointing to the evolution of a paraneoplastic association.
We believe that metastases to the lumbar spine occurred mainly by contiguity due to its proximity to the primary tumor, although hematogenous spread may also have occurred.
The involvement of the thoracic and lumbar vertebrae with invasion of the iliac bone and coccyx, as well as the thickening of the nerve roots due to tumor infiltration in the lumbosacral region would explain the crural paraplegia and the conus medullaris and cauda equina syndrome that the patient presented during the evolution of the clinical picture.
In the case presented, specific antibodies for paraneoplastic syndromes were not tested, because the suspicion of a solid tumor was made when the patient developed signs of compression of the nervous system by an abdominal mass, so a biopsy was the necessary intervention.
Although there is no proof of CIDP manifesting as paraneoplastic syndrome 6, we believe that the association reported in this case is not coincidental. The response to corticosteroid therapy and the finding of specific antibodies point to an autoimmune pathogenesis in paraneoplastic neuropathies [11,12,13]. In conclusion, this case report raises the possibility of CIDP related to solid tumors, thus expanding the possibilities of presentations of paraneoplastic syndromes related to solid tumors.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
